Empirical Research on Medical Ethics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DESCRIPTIVE ETHICS in the SUDAN: an EXAMPLE by TORENORD~NSTAM
DESCRIPTIVE ETHICS IN THE SUDAN: AN EXAMPLE by TORENORD~NSTAM The study of ethical beliefs in the Sudan is a fascinating and more or less unexplored field of research. The purpose of this paper is to give an introductory survey of some of the problems and possible lines of research \vithin this field. I shall first give a general outline of the nature of descriptive ethics, as I see it, then I shall highlight somc of the problems in the field by discussing onc particulnr exainple. Finally, I shall bricfly indicate why research of this nature is of speci~il importance in a developing country like the Sudan. The field of descriptive ethics Descriptive ethics can be defined as the description and analysis of the ethics of individuals and groups. Such a brief definition will introduce the nature of the field, but it certainly stands in need of further explanation. This applies partie- ularly to the key word in the definition, the term "ethics," which can be used in a variety of ways with more or less clear meanings. 1 propose to take the term "ethics" in a wide sense so that any view about what is right and wrong, good and bad, praiseworthy and blame~vorthywill count as a inoral vieu.. An individual's ethics is, then, the system comprising all his values and ideals, all his opinions about right and wrong conduct, all his beliefs about deserts and punishment, responsibility and free will, and so on. In short, an individual's ethics. in this sense, consists of his ideal of life: it is the sum total of his personality ideals, his social ideals, his political ideals, Iiis economic ideals, and so forth. -

Normative and Descriptive Aspects of Management Education: Differentiation and Integration
Journal of Educational Issues ISSN 2377-2263 2015, Vol. 1, No. 1 Normative and Descriptive Aspects of Management Education: Differentiation and Integration Gavriel Meirovich (Corresponding author) Department of Management, Bertolon School of Business, Salem State University 352 Lafayette Street, Salem, MA 01930, United States Tel: 978-543-6948 Fax: 978-542-6027 E-mail: [email protected] Received: April 7, 2015 Accepted: May 27, 2015 Published: June 3, 2015 doi:10.5296/jei.v1i1.7395 URL: http://dx.doi.org/10.5296/jei.v1i1.7395 Abstract This study advocates strongly for clear differentiation and synthesis of descriptive and normative approaches in management education. There is a certain isolation of normative and descriptive theoretical frameworks presented in management courses. Normative frameworks in management explain how organizations should be managed, while descriptive frameworks show how they actually are managed. Significant portions of what we teach in the business curriculum are predominantly descriptive; other parts are mostly normative, or prescriptive. If these domains are not sufficiently connected, the relevance of both approaches diminishes. When one piece of material explains only the current reality without providing tools to improve it, while another piece prescribes steps for improvement that are not grounded in a particular context, students lose interest in both. The paper presents various modes of differentiation and integration between two realms and pertinent ways to recalibrate management courses. Keywords: Normative and descriptive framework, Differentiation, Integration 1. Introduction The purpose of business education is preparing future business professionals for successful careers and meaningful lives. The continued rise of its cost poses difficult questions about the relevance of contemporary business education in general and management education in particular. -

Normative Ethics
Normative ethics From Wikipedia, the free encyclopedia Normative ethics is the new "it" branch of philosophical ethics concerned with Ethics classifying actions as right and wrong. Theoretical Normative ethics attempts to develop a set of rules governing human conduct, Meta-ethics or a set of norms for action. It deals with what people should believe to be right Normative · Descriptive Consequentialism and wrong, as distinct from descriptive ethics, which deals with what people do Deontology believe to be right and wrong. Hence, normative ethics is sometimes said to be Virtue ethics prescriptive, rather than descriptive. Ethics of care Good and evil · Morality Moreover, because it examines standards for the rightness and wrongness of actions, normative ethics is distinct from meta-ethics, which studies the nature Applied of moral statements, and from applied ethics, which places normative rules in practical contexts. Bioethics · Medical Engineering · Environmental Human rights · Animal rights Normative ethical theories Legal · Media Business · Marketing Consequentialism (Teleology) argues that the morality of an action is Religion · War contingent on the action's outcome or result. Some consequentialist theories include: Core issues Utilitarianism, which holds that an action is right if it leads to the most value for the greatest number of people (Maximizes value for Justice · Value all people). Right · Duty · Virtue Egoism, the belief that the moral person is the self-interested Equality · Freedom · Trust person, holds that an action is right if it maximizes good for the Free will · Consent self. Moral responsibility Deontology argues that decisions should be made considering the factors Key thinkers of one's duties and other's rights. -

Environmental Ethics − Professional Issues Based On: Lawrence M
ETHICS, PROFESSIONALISM AND CRITICISM OF THE SOURCES Professional Ethics Course MIMA LECTURE Information about the course: http://www.idt.mdh.se/kurser/cd5590 Gordana Dodig-Crnkovic http://www.idt.mdh.se/kurser/ethics/ Department of Computer Science and Electronics [Website provides ethics resources including case studies and Mälardalen University contextualised scenarios in applied/professional ethics, working examples of applied ethical problems used in teaching to highlight 15 August 2007 relevant ethical principles, materials on informed consent, confidentiality, assessment, privacy, trust and similar. ] 1 2 CONTENT – Identifying Ethical Issues Identifying Ethical Basic Moral Orientations Ethical Relativism, Absolutism, and Pluralism Issues Immanuel Kant The Ethics of Duty (Deontological Ethics) Utilitarianism Rights Justice The Ethics of Character: Virtues and Vices Egoism Moral Reasoning and Gender Environmental Ethics − Professional Issues Based on: Lawrence M. Hinman, Ph.D. − Criticism of the Sources Director, The Values Institute − Conclusions University of San Diego 3 4 Ethics and Morality Ethics and Morality Etymology The terms ethics and morality are often used Morality and ethics have same roots, mores which interchangeably - indeed, they usually can mean the means manner and customs from the Latin and same thing, and in casual conversation there isn't a etos which means custom and habits from the Greek. problem with switching between one and the other. However, there is a distinction between them in Robert Louden, Morality and Moral Theory philosophy! 5 6 Ethics and Morality Ethics and Morality Strictly speaking, morality is used to refer to what we Morality: first-order set of beliefs and practices about would call moral standards and moral conduct while how to live a good life. -
Ethical Realism/Moral Realism Ethical Propositions That Refer to Objective Features May Be True If They Are Free of Subjectivis
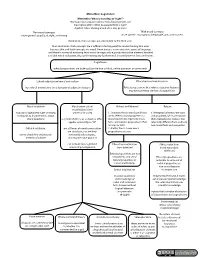
Metaethics: Cognitivism Metaethics: What is morality, or “right”? Normative (prescriptive) ethics: How should people act? Descriptive ethics: What do people think is right? Applied ethics: Putting moral ideas into practice Thin moral concepts Thick moral concepts more general: good, bad, right, and wrong more specic: courageous, inequitable, just, or dishonest Centralism- thin concepts are antecedent to the thick ones Non-centralism- thick concepts are a sucient starting point for understanding thin ones because thin and thick concepts are equal. Normativity is a non-excisable aspect of language and there is no way of analyzing thick moral concepts into a purely descriptive element attached to a thin moral evaluation, thus undermining any fundamental division between facts and norms. Cognitivism ethical propositions are truth-apt (can be true or false), unlike questions or commands Ethical subjectivism/moral anti-realism Ethical realism/moral realism True ethical propositions are a function of subjective features Ethical propositions that refer to objective features may be true if they are free of subjectivism Moral relativism Moral universalism/ Robust and Minimal Robust moral objectivism/ nobody is objectively right or wrong universal morality 1. Semantic thesis: moral predicates 3. Metaphysical thesis: the facts in regards to diagreements about are to refer to moral properties so and properties of #1 are robust-- moral questions a system of ethics, or a universal ethic, moral statements represent moral their metaphysical status is not applies universally to "all" facts, and express propositions that relevantly dierent from ordinary are true or false non-moral facts and properties Cultural relativism not all forms of moral universalism 2. -

Meta-Theoretical Frameworks and Theological Ethics: Bioethical Decision-Making from a Reformed Perspective
Meta-theoretical frameworks and theological ethics: Bioethical decision-making from a reformed perspective M. C. de Lange Thesis submitted for the degree Doctor of Philosophy in Ethics at the Potchefstroom Campus of the North-West University Promoter: Prof. Dr. J.M. Vorster Co-promoter: Prof. Dr. H.J.M. van Deventer POTCHEFSTROOM December 2010 '11iis tfiesisis aer£icater£to'Dr. 'Dank{.:A..'Vorobiof, M.'D. (Mer£ica{Oncofogist) at Sanr£tonOncofogy Centre, Jofiannes6urg, Soutfi:Africa for fiis professiona{anr£ compassionate care over tfieyast fourteen years, anr£ for being an instrument in <god's fianr£s. ACKNOWLEDGEMENTS I would like to extend my heartfelt gratitude and appreciation to the following people and institutions whose assistance enabled me to complete this study: • Professors Koos Vorster and Hans van Deventer, my promoters, for their scholarly insight, critical guidance and their genuine interest in my scholarly development; • Professors Dries du Plooy and Fika J. van Ransburg, Deans of the Faculty of Theology, Potchefstroom Campus, NWU for their belief in me and this interdisciplinary project, and for their sincere interest in me, both as a colleague and as a postgraduate student; • Professors Herrie van Rooy and Francois Viljoen, Research Directors of the Research Unit for Reformed Theology and the Development of South African Society, for financial support and encouragement; • The Research Support Directorate, Institutional Office, NWU for financial support; • The management and staff of the following libraries for permission to use the libraries and for assistance in locating material: The Theological Library, especially Mesdames Gerda van Rooyen and Malie Smit for assistance with locating material, as well as the staff of the Interlibrary Section of the Ferdinand Postma Library, Potchefstroom Campus, NWU and Stellenbosch University Library; • The staff of Statistical Consultation Services, Mrs. -

Descriptive Ethics What Does Moral Philosophy Know About Morality?
N. Hamalainen Descriptive Ethics What does Moral Philosophy Know about Morality? ▶ Contributes to the growing scientific and philosophical literature on valuation studies ▶ Addresses analytic ethical theory in a fresh way ▶ Brings together methodological questions raised in post- Wittgensteinian ethics, Pragmatist ethics, and post-Foucaudlian discussions of personhood and subjectivity with communitarian approaches to ethics This book is an investigation into the descriptive task of moral philosophy. Nora Hämäläinen explores the challenge of providing rich and accurate pictures of the moral conditions, values, virtues, and norms under which people live and have lived, along with relevant knowledge about the human animal and human nature. While modern 1st ed. 2016, X, 132 p. moral philosophy has focused its energies on normative and metaethical theory, the task of describing, uncovering, and inquiring into moral frameworks and moral practices Printed book has mainly been left to social scientists and historians. Nora Hämäläinen argues that this division of labour has detrimental consequences for moral philosophy and that a Hardcover reorientation toward descriptive work is needed in moral philosophy. She traces resources ISBN 978-1-137-58616-2 for a descriptive philosophical ethics in the work of four prominent philosophers of the ▶ 54,99 € | £49.99 twentieth century: John Dewey, Ludwig Wittgenstein, Michel Foucault, and Charles Taylor, ▶ *58,84 € (D) | 60,49 € (A) | CHF 65.00 while also calling on thinkers inspired by them. Nora Hämäläinen is Associate Professor (docent) in philosophy at the University of Helsinki, Finland. She is the author of Literature and Moral Theory and has co-edited the volume Language, Ethics and Animal Life — Wittgenstein and Beyond (with Niklas Forsberg and Mikel Burley). -

Human Destinies
HUMAN DESTINIES Philosophical Essays in Memory of Gerald Hanratty edited by Fran O’ROURKE University of Notre Dame Press Notre Dame, Indiana © 2012 University of Notre Dame Copyright © 2012 by University of Notre Dame Notre Dame, Indiana 46556 www.undpress.nd.edu All Rights Reserved Manufactured in the United States of America Published with financial support from the College of Arts, University College Dublin, and the College of Human Science, University College Dublin. Library of Congress Cataloging-in-Publication Data © 2012 University of Notre Dame Introduction To his colleagues and many friends, the news of Gerald Hanratty’s un- expected death on 9 October 2003 came as a deeply personal shock. Gerry was a profound, simple, and uncomplicated person, universally held in fond regard; one never heard even the slightest negative com- ment about him—lamentably a rare tribute even among philosophers. There was nothing special or extraordinary about Gerald Hanratty’s life; in the manner of his living, devotion to learning, and dedication in the service of others, however, he was unique. Born in Co Roscommon on 26 May 1941, where his father was a primary school teacher, Gerry attended Blackrock College, Dublin. In 1958 he entered Clonliffe, seminary of the Dublin Diocese, and also began his philosophical studies at University College Dublin. He graduated with an MA in 1962. He attended the Pontifical Irish Col- lege in Rome from 1962 to 1966, pursuing theological studies at the Pontifical Lateran University. He received a BD in 1964 and an STL in 1966; in the same year he was ordained a priest for the Dublin Dio- cese. -

Universal Values, Contextualization and Bioethics: Knowledge Production in the Age of Genetics
JAHR Vol. 1 No. 1 2010 UDK: 179:61 Review Article/ Pregledni članak Received/Primljeno 22/03/2010 Enikő Demény* Universal Values, Contextualization and Bioethics: Knowledge Production in the Age of Genetics »Th ere can be no culturally and psychologically perceptive ethics without taking into account the diversity of moral lives, but there can be no ethics at all without universals ... Th e hard part is to devise a theory that can readily join universality and the moral complexity of everyday life« (Callahan 2000, p. 38, 41). ABSTRACT Th e impact of biotechnology on all living things is an interdisciplinary inquiry into some of humanity’s most fundamental questions: Who are we? How do we live together? How do we relate to the biosphere, to the rest of the living world? Are the answers given to these questions shaped by various contexts: social, cultural, economic, so on? Are there universal answers to these questions? Choosing this interdisciplinary fi eld of knowledge production as object of inquiry off ers an opportunity to investigate how traditional theories and disciplines are challenged to evolve in new directions as a response to techno-scientifi c developments of our times. It also allows us to study patterns of knowledge production, to examine hierarchies of knowledge and expertise, as well as the possibilities of interdisciplinary/transdisciplinary practices in a multicultural context. I will argue that a framework that incorporates universal principles shall constitute one di- mension of an adequate ethical theory in the context of new genetics providing that its princi- ples are formulated in non-exclusionary terms that refl ect the relational context of individual lives. -

Normative Ethics and Sport: a Moral Manifesto
PHYSICAL CULTURE AND SPORT. STUDIES AND RESEARCH DOI: 10.2478/pcssr-2014-0008 Normative Ethics and Sport: A Moral Manifesto Jerzy Kosiewicz Josef Pilsudski University of Physical Education in Warsaw, Poland ABSTRACT This article constitutes a strictly cognitive and completely non-ideological moral (or rather, amoral) manifesto that makes no value judgments. The article concerns relationships that, according to sport enthusiasts with varying levels of competence, occur between sport and normative ethics. The author of this article supports a standpoint he terms ethical negationism that rejects the need for moral rules to externally support and bolster the rules of sport competition. The author assumes that the rules of sport play and competition are, and should be, completely amoral and independent from ethics. While this article is a fully autonomous ethical manifesto, it also constitutes an introduction to other articles in this issue of the journal arguing that sport competition takes place beyond the scope of moral good and evil. The author debates value judgments commonly held by sport enthusiasts who, albeit presumably driven by noble intentions, take great effort to bolster the formal, functional, and axiological status of sport. Most sport enthusiasts claim that sport has a unique moral and normative mission to propagate intuitively understood religious and non-religious good. They argue that sport constitutes something more than sport play and competition. The author rejects this point of view and assumes that normative ethics is unnecessary because what only matters is strictly following the rules of competition (referred to as pure play) and skillfully and praxeologically (i.e., effectively) using them during play, thus working towards the assumptions and aims of a given sport activity. -

CORMAC MCCARTHY and the ETHICS of READING By
CORMAC MCCARTHY AND THE ETHICS OF READING by MATTHEW RUSH HORTON (Under the Direction of Carl Rapp) ABSTRACT To demonstrate his interest in the ethical dimension of fiction and reading, this study examines the narrative strategies of Cormac McCarthy in three of his novels: Outer Dark, Child of God, and Blood Meridian. Each novel dramatizes a dilemma related to the act of reading; accordingly, “the ethics of reading” is treated as an element of his fiction, not as a theoretical category. Instead of prescribing an approach to reading, this study focuses on how these novels raise ethical questions about the act of reading. As ethical criticism, it addresses the central concern of all ethical inquiry (“what is the good?”) by exploring how his narrative form and storytelling methods complement the theme of accountability. Although the reader of these novels might grow as a reader, he is under no moral obligation to reflect on how he should read them. Scholars have shown an interest in the ethical and formalist dimensions of McCarthy’s work for some time, but few have considered how he addresses ethical questions through his formal technique. Comprising a stylistic and thematic trilogy, Outer Dark, Child of God, and Blood Meridian demonstrate how story and narration intersect and interact in his fiction. Implications for scholarship and teaching are discussed in the final chapter. INDEX WORDS: Ethics of reading, Ethical criticism, Narrative structure, Ethics of fiction, Cormac McCarthy CORMAC MCCARTHY AND THE ETHICS OF READING by MATTHEW RUSH -
Types of Judgments, Prerequisite for Ethical Scrutiny, Meta Ethics, Applied Ethics, Normative-Descriptive Ethics
Human Interface: Types of Judgments, Prerequisite for Ethical scrutiny, Meta Ethics, Applied ethics, Normative-Descriptive ethics By Prof. Sheela Misra Dept of Statistics University of Lucknow Email:[email protected] Outline: • Types of Judgments • Areas in Study of Ethics – S1:Meta-Ethics / Critical Ethics – S2: Applied Ethics – S3: Normative vs. Descriptive Ethics – Ethics vs. Morality? – Legality vs. Morality • Preconditions for Ethical Scrutiny – Pc1: Free Will – Pc2: Knowledge – Pc3: Voluntary Action • Case study: • Reference; https://mrunal.org/2015/09/e1p1-meta-ethics-judgement- types-freewill-knowledge-normative-ethics.html • First part would be Ethics and Human interface- further subdivided into three articles • E1/P1: Types of Judgments, Pre-requisite for Ethical scrutiny, Meta Ethics, Applied ethics, Normative- Descriptive ethics. • E1/P2: Theories of Ethics: virtual ethics, deontological vs. teleological ethics, utilitarianism, hedonism, epicureanism, egoism, conduct ethics etc. • E1/P3: Values, Role of family-society-educational institutions in inculcating values, ethics and private and public relationships. • 1.Factual or Epistemological Earth rotates around Sun. Whether you test or an alien species tests, the fact will remain the same. There are only two outcomes: True / False • They’re not morally right or wrong. They’re morally empty, they’re “amoral”. • 2.Aesthetic Judgment Concept of beauty, taste, color, sensualities. • One person may like red color the other person may like blue color. • 3.MoralJudgment • Our sense of good/bad/right/wrong. Question: Are these three judgments inter-related? • Traditional thinkers considered them one and same i.e. what is ‘true’ (factual) is ‘beautiful’ (aesthetic) and therefore it is Good (moral). Something like Satyam-Shivam-Sundaram.