Army Cadet Form:Layout 1 20/4/12 08:43 Page 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Army Cadet Force Our Motto: Inspire to Achieve
Cullybackey College Detachment 1st (Northern Ireland) Battalion Army Cadet Force The Army Cadet Force Our Motto: Inspire to Achieve The Army Cadet Force is a long established National Voluntary Youth Organisation who have over 154 years’ experience in offering “Fun, Friends, Action, Adventure, Qualifications” to cadets ranging in age from 12 years to 18 years old. Throughout the UK over 46000 young people have taken up the challenge of becoming an Army Cadet, with over 1500 cadets from a wide range of backgrounds and areas here in Northern Ireland it is also one of the most inclusive, cost effective and progressive youth organisation your son or daughter could join. The Cullybackey College Detachment has continued to flourish and have been producing some fine cadets, such as Cadet Lance Corporal Brandon Lee (Left) who won the Best Overall Cadet at the National Mini Micks competition at Magilligan The Detachment are proud to be badge Irish Guards and to be known as Mini Micks (Irish Guards cadets are known as Mini Micks following the nickname of the regiment “The Micks”) Cullybackey cadets are amongst some of the best qualified in C Company as many of the cadets have achieved their Star levels and have attended many different courses ranging from canoeing, climbing, and Signals They had the honour to attend the St Patrick’s Day Parade with the 1st Battalion Irish Guards at Aldershot and got presented a sprig of shamrock by the HRH Duchess of Cambridge. (Pictured Right) WHAT CAN YOU DO AS A CADET Army Cadets work towards a common Cadet -

Celebrating 150 Years of the Cadets 1 8 6 0 - 2 0 1 0
Celebrating 150 years of the Cadets 1 8 6 0 - 2 0 1 0 Greater London Reserve Forces and Cadets Association Contents 1 Foreword 2 A proud history 6 Sea Cadet Corps 10 Army Cadet Force 14 Air Training Corps 18 Combined Cadet Force 20 Cadet150 Events 21 Contacts Above: The ‘Unity Band’, comprising Sea, Army and Air Cadets plus other youth organisations, on parade in London for Remembrance Sunday, November 2008. Foreword Celebrating 150 years of the Cadets The Cadet Forces have, not unnaturally, come a long way from their 1860s origins. They have evolved into unique voluntary youth organisations, offering young people opportunities to develop themselves, to try new adventures and activities, and to learn key lessons in citizenship and the importance of society. But their links to the Armed Forces are as strong as ever. In many areas of the country they are the only face of the Services in the community. They take pride in the values and ethos of the Armed Forces and the lessons of good citizenship and responsibilities these bring. Their essential links with the Reserve Forces’ and Cadets’ Associations, which help administer and support them, are equally strong. None of this would be possible without the Adult Volunteers, whose commitment, leadership and example underpin the development and success of the Cadet Movement. Their reward Air Chief Marshal Sir Jock Stirrup, is to see the cadets change for the better as they are given a Chief of the Defence Staff head-start in life, and as they develop links with the community in which they live. -
Terminology & Rank Structure
Somerset Cadet Bn (The Rifles) ACF Jellalabad HouseS 14 Mount Street Taunton Somerset TA1 3QE t: 01823 284486 armycadets.com/somersetacf/ facebook.com/SomersetArmyCadetForce Terminology & Rank Structure The Army Cadets and the armed forces can be a minefield of abbreviations that can confound even the most experienced person, never mind a new cadet or adult instructor. To address that this document has been prepared that will hopefully go some way towards explanation. If you train with the regular or reserve armed forces you will come across many of the more obscure acronyms. Naturally this document is in a state of continuous update as new and mysterious acronyms are created. ACRONYMS/TERMINOLOGY AAC Army Air Corp accn Accommodation ACFA Army Cadet Force Association Adjt Adjutant Admin Administration, or as in Personal Admin - “sort your kit out” AFD Armed Forces Day AFV Armoured Fighting Vehicle, tracked fighting vehicle, see MBT AI Adult Instructor (NCO) (initials Ay Eye) Ammo Ammunition AOSB Army Officer Selection Board AR Army Reserve (formerly Territorial Army) Armd Armoured AROSC Army Reserve Operational Shooting Competition (formerly TASSAM) Arty Artillery, as in Arty Sp - artillery support ATC Air Training Corps Att Attached, as in Attached Personnel - regular soldiers helping Basha Personal Shelter BATSIM Battlefield Simulation, eg Pyro (see below) Bde Brigade BFA Blank Firing Adaptor/Attachment Blag To acquire something BM Bugle Major/Band Master 20170304U - armycadets.com/somersetacf Bn Battalion Bootneck A Royal Marines Commando -

Royal Air Force Air Cadets Consent Certificate
OFFICIAL-SENSITIVE (PERSONAL) (When Completed) TG Form 3822A Royal Air Force Air Cadets Consent Certificate Section 1a – Cadet Details We will add your child’s contact details to the Cadet Forces Management Information System (MIS) which is used to manage their membership in the RAF Air Cadets and act as their central record. Full Name of Child Date of Birth / / Religion Gender ☐Male ☐Female☐Prefer not to say ☐Other_________________ Pronoun ☐He/Him ☐She/Her ☐They/Them White: ☐English / Welsh / Scottish / Northern Irish / British ☐Irish ☐Gypsy or Irish Traveller ☐Any other White background Asian / Asian British: ☐Indian ☐ Pakistani ☐ Bangladeshi ☐Chinese ☐Any other Asian background Ethnicity ☐White and Black Caribbean ☐White and Black African ☐White and Asian (Choose Mixed / Multiple Ethnic Groups: ☐Any other Mixed / Multiple ethnic background ONE) Black/ African / Caribbean / Black British: ☐African ☐Caribbean ☐Any other Black / African / Caribbean background Other Ethnic Group: ☐Arab ☐Any other ethnic group Prefer Not to Say ☐Prefer not to say Section 1b – External Agency Involvement Is there a Local Authority representative working with your family including Social Worker, Early Help Worker, Family ☐ ☐ Support Worker or Family Intervention Worker? Yes No Section 1c – Cadet Contact Details Please Note: At least one telephone number and an email address is required. These will be used to set up your child’s central record and Cadet Portal account. Property Name/Number Street Area Town County Country Post Code Mobile Phone Home Phone Primary Email Secondary Email Note: The primary email address will be used for Cadet Portal including notifications about events and activities as well as Cadet Portal password resets. -

Front Cover & Security.Qxd
RESTRICTED Chapter 3 MILITARY KNOWLEDGE CCF AND ACF SECTION 1. — RANKS AND BADGES OF RANK 0301. The aim of this Section is to teach cadets the names and ranks of the offi- cers, SSIs and AIs in their own contingents/detachments, and where appropriate, those in their superior headquarters. The opportunity is taken to explain military ranks and badges of rank at the same time. 0302. The ranks and badges of rank shown below should be known by all cadets: Officers Second Lieutenant Captain Major Lieutenant Colonel Lieutenant Colonel Non Commissioned Officers and Warrant Officers Lance Corporal Sergeant Staff Warrant Warrant Corporal Sergeant Officer Officer Class 2 Class 1 (WO2) (WO1) Fig 56. — Ranks and Badges of Rank RESTRICTED 3-1 RESTRICTED SECTION 2. — ARMY STRUCTURE — ARMS AND SERVICES 0303. As cadets gain a knowledge of basic military training by working their way through the APC syllabus, it is desirable that they gain a more general knowledge of how the Army is organized into Regiments and Corps. Any cadet who requires fur- ther information about the Army can obtain it from his own contingent or detachment officer, from the schools liaison officer or from the nearest Job Centre. 0304. The people of Britain live in freedom, but only because we have always fought to keep that freedom whenever it was attacked. Our Armed Forces stand in constant readiness to defend the United Kingdom in time of war or world tension. The Cold War has ended but the world today is still unstable. The rise of nationalism, eth- nic strife, religious fundamentalism, terrorism and threat to the world environment are all increasing. -

The Cadet Corps Originated from a Letter Sent by the War Office on 12Th May 1859 to Lord Lieutenants Asking Them to Raise Rifle Volunteer Battalions for Home Defence
HISTORY OF THE CCF The Cadet Corps originated from a letter sent by the War Office on 12th May 1859 to Lord Lieutenants asking them to raise Rifle Volunteer Battalions for Home Defence. As a result, a number of schools formed units in 1859 which were attached to these battalions. In 1908, the Minister for War, Lord Haldane, invited universities and schools to form units of new Corps to provide officers for the then newly formed Territorial Force and a reservoir of officer material in the event of war. As a result, 87 schools accepted and formed the Junior Officers’ Training Corps. This was administered directly from the War Offices which drew up schemes for training, introduced proficiency certificates and arranged for annual camps and Inspections. HM King Edward VII consented to become the Colonel-in-Chief of the OTC. Some other schools besides those forming the OTC had formed Volunteer cadet units soon after 1900 and subsequently received full official recognition and a small grant from public funds. These units were usually affiliated to TA Regiments and administered through County TA Associations. In 1915, 92 such School Units were attached to various TA Regiments. Official recognition and financial support were withdrawn in 1930 from cadet units not in the OTC. The Public Secondary Schools Cadet Association under the guidance of its President, Field Marshal Lord Allenby, supported and played a significant part in the forming of the British National Cadet Association which subsequently organised County Cadet Committees to administer local cadet units and it is a matter of justifiable pride that so many of the schools affected carried on. -
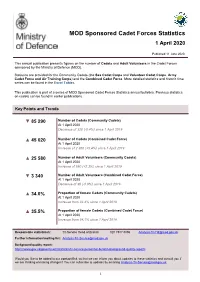
MOD Sponsored Cadet Forces Statistics April 2020
MOD Sponsored Cadet Forces Statistics 1 April 2020 Published 11 June 2020 This annual publication presents figures on the number of Cadets and Adult Volunteers in the Cadet Forces sponsored by the Ministry of Defence (MOD). Statistics are provided for the Community Cadets (the Sea Cadet Corps and Volunteer Cadet Corps, Army Cadet Force and Air Training Corps) and the Combined Cadet Force. More detailed statistics and historic time series can be found in the Excel Tables. This publication is part of a series of MOD Sponsored Cadet Forces Statistics annual bulletins. Previous statistics on cadets can be found in earlier publications. Key Points and Trends ▼ 85 290 Number of Cadets (Community Cadets) At 1 April 2020 Decrease of 320 (-0.4%) since 1 April 2019 ▲ 45 020 Number of Cadets (Combined Cadet Force) At 1 April 2020 Increase of 2 300 (+5.4%) since 1 April 2019 ▲ 25 580 Number of Adult Volunteers (Community Cadets) At 1 April 2020 Increase of 580 (+2.3%) since 1 April 2019 ▼ 3 340 Number of Adult Volunteers (Combined Cadet Force) At 1 April 2020 Decrease of 30 (-0.9%) since 1 April 2019 ▲ 34.0% Proportion of female Cadets (Community Cadets) At 1 April 2020 Increase from 33.4% since 1 April 2019 ▲ 35.5% Proportion of female Cadets (Combined Cadet Force) At 1 April 2020 Increase from 34.1% since 1 April 2019 Responsible statistician: Tri-Service Head of Branch 020 7807 8896 [email protected] Further information/mailing list: [email protected] Background quality report: https://www.gov.uk/government/statistics/tri-service-personnel-bulletin-background-quality-reports -

Army Dress Regulations (All Ranks)
ARMY DRESS REGULATIONS (ALL RANKS) Part 8 Dress Regulations for Combined Cadet Force (Army Sections) and the Army Cadet Force Ministry of Defence PS12(A) August 2014 SECTION 1 GENERAL INSTRUCTIONS SCOPE 08.101. This Part of Army Dress Regulations deals with the scales of clothing and dress regulations for Cadet Forces Adult Volunteers (CFAV) and cadets in Army Sections of the Combined Cadet Force (CCF) and detachments of the Army Cadet Force (ACF). The scales of clothing are set out in Section 4 of this pamphlet. APPLICATION 08.102. The Regulations contained in Part 8 apply only to CCF (Army Sections) and ACF. LAYOUT 08.103. Part 8 is divided into the following sections and a series of related clothing scales: a. Section 1 - General Instructions. b. Section 2 - Provision and Maintenance of Clothing. c. Section 3 - Dress. d. Section 4 - Personal Clothing Scales. e. Section 5 – CCF and ACF Banners. f. Section 6 – Detailed Instructions for the Wearing Of Uniform in Public. g. Section 7 – Special Instructions for Wearing Uniform – Religious and Cultural Considerations. ARMY DRESS COMMITTEE 08.104. The Army Dress Committee considers all proposals affecting authorised orders of dress and embellishments and approves the wearing of new pattern clothing; no deviation from any authorised pattern of clothing is permitted. 08.105. Dress Proposals. Proposals are to be forwarded, through Cadet Branch HQ Support Command, to the Secretary Army Dress Committee, PS12(A), MOD Main Building. 08.106. Proposal Guidelines. To assist the Committee Secretariat in any research, and to avoid unnecessary delay or correspondence, originators are to observe the following guidelines in the preparation of proposals which should include: a. -
Information on Serving and Reserve Personnel Enrolled As Cadet Force
Ministry of Defence Main Building Whitehall London SW1A 2HB United Kingdom Our Reference: XXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXX XXXXXXXXXX Dear XXXXXXXXXXX, Thank you for your e-mail to the Ministry of Defence (MOD) dated XXXXXXX in which you requested the following information: 1/ How many members of the Regular Army are also paid CFAV’s in the Army Cadet Force or Combined Cadet Force Army Section either as Officers or Other Ranks 2/ How Many Members of the Army Reserve who are presently serving on Full Time Reserve Service contracts are paid CFAVs of the Army Cadet Force or Combined Cadet Force Army Section either as Officers or Other Ranks 3/ How many members of the Regular Royal Navy are also paid CFAV’s in the Sea Cadet Corps or Combined Cadet Force Navy Section either as Officers or Other Ranks 4/ How Many Members of the Royal Naval Reserve who are presently serving on Full Time Reserve Service contracts are paid CFAVs of the Sea Cadet Corps or Combined Cadet Force Navy Section either as Officers or Other Ranks 5/ How many members of the Regular Royal Air Force are also paid CFAV’s in the Air Training Corp Royal Air Force Volunteer Reserve Training Branch or Combined Cadet Force RAF Section either as Officers or Other Ranks 6/ How Many Members of the Army Reserve who are presently serving on Full Time Reserve Service contracts are paid CFAVs of the Air Training Corp Royal Air Force Volunteer Reserve Training Branch or Combined Cadet Force RAF Section either as Officers or Other Ranks 7/ Is it acceptable to the MOD & Government that members of the three services either Regular or Reserve on FTRS contracts and members of the cadet Forces who are in receipt of a salary from the public purse are double hatting and more importantly double waging when the monies to pay the salary and Voluntary Allowance come from the same fund. -

MOD Sponsored Cadet Forces Statistics 1 April 2021
MOD Sponsored Cadet Forces Statistics 1 April 2021 Published 03 Jun 2021 This annual publication presents figures on the number of Cadets and Adult Volunteers in the Cadet Forces sponsored by the Ministry of Defence (MOD). Statistics are provided for the Community Cadets (the Sea Cadet Corps and Volunteer Cadet Corps, Army Cadet Force and Air Training Corps) and the Combined Cadet Force. More detailed statistics and historic time series can be found in the Excel Tables. This publication is part of a series of MOD Sponsored Cadet Forces Statistics annual bulletins. Previous statistics on cadets can be found in earlier publications. Key Points and Trends ▼ 74 040 Number of Cadets (Community Cadets) At 1 April 2021 Decrease of 11 260 (-13%) since 1 April 2020 ▲ 46 070 Number of Cadets (Combined Cadet Force) At 1 April 2021 Increase of 1 050 (+2%) since 1 April 2020 ▼ 24 200 Number of Adult Volunteers (Community Cadets) At 1 April 2021 Decrease of 1 380 (-5%) since 1 April 2020 ▼ 3 270 Number of Adult Volunteers (Combined Cadet Force) At 1 April 2021 Decrease of 70 (-2%) since 1 April 2020 ▼ 33% Proportion of female Cadets (Community Cadets) At 1 April 2021 Decrease from 34% since 1 April 2020 ◄► 36% Proportion of female Cadets (Combined Cadet Force) At 1 April 2021 Remained at 36% since 1 April 2020 Responsible statistician: Tri-Service Head of Branch 020 7807 8896 [email protected] Further information/mailing list: [email protected] Background quality report: https://www.gov.uk/government/statistics/tri-service-personnel-bulletin-background-quality-reports -

Vacancy for Deputy Commandant 1 (Adults) - Merseyside Army Cadet Force
VACANCY FOR DEPUTY COMMANDANT 1 (ADULTS) - MERSEYSIDE ARMY CADET FORCE Introduction 1. There will be a vacancy for the Deputy Commandant (1) within Merseyside Army Cadet Force from 1 September 2020. The normal place of duty for this post will be the Headquarters of Merseyside ACF which is situated in Altcar Training Camp, L38 7JD. The HQ staff parade on a Saturday, with occasional weekday evening work as directed by the Commandant. County Organisation 2. Merseyside ACF comprises 32 detachments which are divided into four Companies. The County has over 750 Cadets with 185 Cadet Force Adult Volunteers (Officers and Adult Instructors) on strength. Role 3. The post of Deputy Commandant is a voluntary appointment. However, the successful applicant will receive remuneration appropriate to the rank of Lieutenant Colonel as per the current Volunteer Allowance scheme for weekends, courses and camps (currently up to 28 days). In addition, payment for residence to place of duty and motor mileage allowances may be claimed when on official ACF duty. 4. The successful candidate for this appointment will work in close liaison with the Commandant, CTO and Company Commanders, the CEO and QM. He or she will be primarily concerned with the management and welfare of Cadets and Adults under Command. To facilitate this, direct support to the command staff in the production of the staff work and administration surrounding the G1 and G4 staff functions will be necessary. 5. Candidates need to be equally conversant and comfortable with staff work and, in the absence of the Commandant, liaison with military headquarters and other high profile outside agencies. -
The Cadet Training Manual Volume I
PROTECT D/HQDT/18/35/38 Army Code No. 71462 THE CADET TRAINING MANUAL VOLUME I Reprinted incorporating Amendments 1 – 6 June 2001 Note: For details of the following subjects refer to WESTMINSTER for the subject matter: Fieldcraft Training First Aid Training Skill at Arms Training (less old style cadet air rifle) Shooting Training 1990 PROTECT PROTECT SECURITY WARNING NOTICE THIS DOCUMENT IS THE PROPERTY OF HER BRITANNIC MAJESTY’S GOVERNMENT, and is issued for the information of such persons only as need to know its contents in the course of their official duties. Any person finding this document should hand it into a British Forces unit or to a police station for its safe return to the MINISTRY OF DEFENCE, D MOD SY, LONDON SW1 2HB, with particulars of how and where found. THE UNAUTHORIZED RETENTION OR DESTRUCTION OF THE DOCUMENT IS AN OFFENCE UNDER THE OFFICIAL SECRETS ACTS OF 1911 – 1989. (When released to persons outside Government service, this document is issued on a personal basis and the recipient to whom it is entrusted, in confidence, within the provisions of the Official Secrets Acts 1911 – 1989, is personally responsible for its safe custody and for seeing that its contents are disclosed only to authorized persons.) CONDITIONS OF RELEASE (Applicable to copies supplied with Ministry of Defence approval to Commonwealth and Foreign Governments) 1. This information is released by the United Kingdom Government to the recipient Government for Defence purposes only. 2. This information must be accorded the same degree of security protection as that accorded thereto by the United Kingdom Government.