Fatal Balamuthia Mandrillaris Encephalitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Revised Classification of Naked Lobose Amoebae (Amoebozoa
Protist, Vol. 162, 545–570, October 2011 http://www.elsevier.de/protis Published online date 28 July 2011 PROTIST NEWS A Revised Classification of Naked Lobose Amoebae (Amoebozoa: Lobosa) Introduction together constitute the amoebozoan subphy- lum Lobosa, which never have cilia or flagella, Molecular evidence and an associated reevaluation whereas Variosea (as here revised) together with of morphology have recently considerably revised Mycetozoa and Archamoebea are now grouped our views on relationships among the higher-level as the subphylum Conosa, whose constituent groups of amoebae. First of all, establishing the lineages either have cilia or flagella or have lost phylum Amoebozoa grouped all lobose amoe- them secondarily (Cavalier-Smith 1998, 2009). boid protists, whether naked or testate, aerobic Figure 1 is a schematic tree showing amoebozoan or anaerobic, with the Mycetozoa and Archamoe- relationships deduced from both morphology and bea (Cavalier-Smith 1998), and separated them DNA sequences. from both the heterolobosean amoebae (Page and The first attempt to construct a congruent molec- Blanton 1985), now belonging in the phylum Per- ular and morphological system of Amoebozoa by colozoa - Cavalier-Smith and Nikolaev (2008), and Cavalier-Smith et al. (2004) was limited by the the filose amoebae that belong in other phyla lack of molecular data for many amoeboid taxa, (notably Cercozoa: Bass et al. 2009a; Howe et al. which were therefore classified solely on morpho- 2011). logical evidence. Smirnov et al. (2005) suggested The phylum Amoebozoa consists of naked and another system for naked lobose amoebae only; testate lobose amoebae (e.g. Amoeba, Vannella, this left taxa with no molecular data incertae sedis, Hartmannella, Acanthamoeba, Arcella, Difflugia), which limited its utility. -

Multiple Roots of Fruiting Body Formation in Amoebozoa
GBE Multiple Roots of Fruiting Body Formation in Amoebozoa Falk Hillmann1,*, Gillian Forbes2, Silvia Novohradska1, Iuliia Ferling1,KonstantinRiege3,MarcoGroth4, Martin Westermann5,ManjaMarz3, Thomas Spaller6, Thomas Winckler6, Pauline Schaap2,and Gernot Glo¨ ckner7,* 1Junior Research Group Evolution of Microbial Interaction, Leibniz Institute for Natural Product Research and Infection Biology – Hans Kno¨ ll Institute (HKI), Jena, Germany 2Division of Cell and Developmental Biology, School of Life Sciences, University of Dundee, United Kingdom 3Bioinformatics/High Throughput Analysis, Friedrich Schiller University Jena, Germany 4CF DNA-Sequencing, Leibniz Institute on Aging Research, Jena, Germany 5Electron Microscopy Center, Jena University Hospital, Germany 6Pharmaceutical Biology, Institute of Pharmacy, Friedrich Schiller University Jena, Germany 7Institute of Biochemistry I, Medical Faculty, University of Cologne, Germany *Corresponding authors: E-mails: [email protected]; [email protected]. Accepted: January 11, 2018 Data deposition: The genome sequence and gene predictions of Protostelium aurantium and Protostelium mycophagum were deposited in GenBank under the Accession Numbers MDYQ00000000 and MZNV00000000, respectively. The mitochondrial genome of P. mycophagum was deposited under the Accession number KY75056 and that of P. aurantium under the Accession number KY75057. The RNAseq reads can be found in Bioproject Accession PRJNA338377. All sequence and annotation data are also available directly from the authors. The P. aurantium strain is deposited in the Jena Microbial Resource Collection (JMRC) under accession number SF0012540. Abstract Establishment of multicellularity represents a major transition in eukaryote evolution. A subgroup of Amoebozoa, the dictyos- teliids, has evolved a relatively simple aggregative multicellular stage resulting in a fruiting body supported by a stalk. Protosteloid amoeba, which are scattered throughout the amoebozoan tree, differ by producing only one or few single stalked spores. -

Diagnosis of Infections Caused by Pathogenic Free-Living Amoebae
Virginia Commonwealth University VCU Scholars Compass Microbiology and Immunology Publications Dept. of Microbiology and Immunology 2009 Diagnosis of Infections Caused by Pathogenic Free- Living Amoebae Bruno da Rocha-Azevedo Virginia Commonwealth University Herbert B. Tanowitz Albert Einstein College of Medicine Francine Marciano-Cabral Virginia Commonwealth University Follow this and additional works at: http://scholarscompass.vcu.edu/micr_pubs Part of the Medicine and Health Sciences Commons Copyright © 2009 Bruno da Rocha-Azevedo et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Downloaded from http://scholarscompass.vcu.edu/micr_pubs/9 This Article is brought to you for free and open access by the Dept. of Microbiology and Immunology at VCU Scholars Compass. It has been accepted for inclusion in Microbiology and Immunology Publications by an authorized administrator of VCU Scholars Compass. For more information, please contact [email protected]. Hindawi Publishing Corporation Interdisciplinary Perspectives on Infectious Diseases Volume 2009, Article ID 251406, 14 pages doi:10.1155/2009/251406 Review Article Diagnosis of Infections Caused by Pathogenic Free-Living Amoebae Bruno da Rocha-Azevedo,1 Herbert B. Tanowitz,2 and Francine Marciano-Cabral1 1 Department of Microbiology and Immunology, Virginia Commonwealth University School of Medicine, Richmond, VA 23298, USA 2 Department of Pathology, Albert Einstein College of Medicine, Bronx, NY 10461, USA Correspondence should be addressed to Francine Marciano-Cabral, [email protected] Received 25 March 2009; Accepted 5 June 2009 Recommended by Louis M. Weiss Naegleria fowleri, Acanthamoeba spp., Balamuthia mandrillaris,andSappinia sp. -

Bacterial Brain Abscess in a Patient with Granulomatous Amebic Encephalitis
SVOA Neurology ISSN: 2753-9180 Case Report Bacterial Brain Abscess in a Patient with Granulomatous Amebic Encephalitis. A Misdiagnosis or Free-Living Amoeba Acting as Trojan Horse? Rolando Lovaton1* and Wesley Alaba1 1 Hospital Nacional Cayetano Heredia (Lima-Peru) *Corresponding Author: Dr. Rolando Lovaton, Neurosurgery Service-Hospital Nacional Cayetano Heredia, Avenida Honorio Delgado 262 San Martin de Porres, Lima-Peru Received: July 13, 2021 Published: July 24, 2021 Abstract Amebic encephalitis is a rare and devastating disease. Mortality rate is almost 90% of cases. Here is described a very rare case of bacterial brain abscess in a patient with recent diagnosis of granulomatous amebic encephalitis. Case De- scription: A 29-year-old woman presented with headache, right hemiparesis and tonic-clonic seizure. Patient was diag- nosed with granulomatous amebic encephalitis due to Acanthamoeba spp.; although, there was no improvement of symptoms in spite of stablished treatment. Three months after initial diagnosis, a brain MRI showed a ring-enhancing lesion in the left frontal lobe compatible with brain abscess. Patient was scheduled for surgical evacuation and brain abscess was confirmed intraoperatively. However, Gram staining of the purulent content showed gram-positive cocci. Patient improved headache and focal deficit after surgery. Conclusion: It is the first reported case of a patient with cen- tral nervous system infection secondary to Acanthamoeba spp. who presented a bacterial brain abscess in a short time. Keywords: amebic encephalitis; Acanthamoeba spp; bacterial brain abscess Introduction Free–living amoebae cause potentially fatal infection of central nervous system. Two clinical entities have been de- scribed for amebic encephalitis: primary amebic meningoencephalitis (PAM), and granulomatous amebic encephalitis (GAE). -

Developing Novel Therapeutic Agents for Acanthamoeba Infection and Investigating the Process of Encystment
Developing novel therapeutic agents for Acanthamoeba infection and investigating the process of encystment Anas Abdullah Hamad (BSc, MSc) A thesis submitted in partial fulfilment of the requirements of the University of Wolverhampton for the degree of Doctor of Philosophy June 2020 Declaration This work or any part thereof has not previously been presented in any form to the University or to any other body whether for the purposes of assessment, publication or for any other purpose (unless otherwise indicated in page 3). Save for any express acknowledgements, references and/or bibliographies cited in the work, I confirm that the intellectual content of the work is the result of my own efforts and of no other person. The right of Anas Abdullah Hamad to be identified as author of this work is asserted in accordance with ss.77 and 78 of the Copyright, Designs and Patents Act 1988. At this date copyright is owned by the author. Signature………………………………………. Date……………………………………………. 15/10/2020 2 List of posters and publication related to the work presented in this thesis: Heaselgrave, W., Hamad, A., Coles, S. and Hau, S., 2019. In Vitro Evaluation of the Inhibitory Effect of Topical Ophthalmic Agents on Acanthamoeba Viability. Translational vision science & technology, 8(5), pp.17-17. Manuscript published. Hamad, A. and Heaselgrave, W., 2017. Developing novel treatments for the blinding protozoan eye infection Acanthamoeba keratitis. Proceedings of the Internal Annual Research Symposium, Poster no. 23, University of Wolverhampton, UK. Hamad, A. and Heaselgrave, W., 2018. Developing new treatments and optimising existing treatment strategies for the corneal infection Acanthamoeba keratitis. -

This Thesis Has Been Submitted in Fulfilment of the Requirements for a Postgraduate Degree (E.G
This thesis has been submitted in fulfilment of the requirements for a postgraduate degree (e.g. PhD, MPhil, DClinPsychol) at the University of Edinburgh. Please note the following terms and conditions of use: This work is protected by copyright and other intellectual property rights, which are retained by the thesis author, unless otherwise stated. A copy can be downloaded for personal non-commercial research or study, without prior permission or charge. This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author. The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author. When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given. Protein secretion and encystation in Acanthamoeba Alvaro de Obeso Fernández del Valle Doctor of Philosophy The University of Edinburgh 2018 Abstract Free-living amoebae (FLA) are protists of ubiquitous distribution characterised by their changing morphology and their crawling movements. They have no common phylogenetic origin but can be found in most protist evolutionary branches. Acanthamoeba is a common FLA that can be found worldwide and is capable of infecting humans. The main disease is a life altering infection of the cornea named Acanthamoeba keratitis. Additionally, Acanthamoeba has a close relationship to bacteria. Acanthamoeba feeds on bacteria. At the same time, some bacteria have adapted to survive inside Acanthamoeba and use it as transport or protection to increase survival. When conditions are adverse, Acanthamoeba is capable of differentiating into a protective cyst. -

Granulomatous Meningoencephalitis Balamuthia Mandrillaris in Peru: Infection of the Skin and Central Nervous System
SMGr up Granulomatous Meningoencephalitis Balamuthia mandrillaris in Peru: Infection of the Skin and Central Nervous System A. Martín Cabello-Vílchez MSc, PhD* Universidad Peruana Cayetano Heredia, Instituto de Medicina Tropical “Alexander von Humboldt” *Corresponding author: Instituto de Medicina Tropical “Alexander von Humboldt”, Av. Honorio Delgado Nº430, San A. Martín Cabello-Vílchez, Universidad Peruana Cayetano Heredia, MartínPublished de Porras, Date: Lima-Perú, Tel: +511 989767619, Email: [email protected] February 16, 2017 ABSTRACT Balamuthia mandrillaris is an emerging cause of sub acute granulomatous amebic encephalitis (GAE) or Balamuthia mandrillaris amoebic infection (BMAI). It is an emerging pathogen causing skin lesions as well as CNS involvement with a fatal outcome if untreated. The infection has been described more commonly in inmunocompetent individuals, mostly males, many children. All continents have reported the disease, although a majority of cases are seen in North and South America, especially Peru. Balamuthia mandrillaris is a free living amoeba that can be isolated from soil. In published reported cases from North America, most patients will debut with neurological symptoms, where as in countries like Peru, a skin lesion will precede neurological symptoms. The classical cutaneous lesionis a plaque, mostly located on face, knee or other body parts. Diagnosis requires a specialized laboratory and clinical experience. This Amoebic encephalitis may be erroneously interpreted as a cerebral neoplasm, causing delay in the management of the infection. Thediagnosis of this infection has proven to be difficult and is usually made post-mortem but in Peru many cases were pre-morten. Despite case fatality rates as high as > 98%, some experimental therapies have shown protozoal therapy with macrolides and phenothiazines. -

Pathogenic Free Living Amoeba
Middle Black Sea Journal of Health Science August 2015; 1(2): 13-20 REVIEW Risks and Threats Comes with Global Warming: Pathogenic Free Living Amoeba Nihal Doğan1 1Osmangazi University Medical Faculty Microbiology Department. Eskişehir, Turkey Received: 28 July 2015 accepted: 12 August 2015/ published online: 30 August 2015 © Ordu University Institute of Health Science, Turkey, 2015 Abstract Free living amoebae like Naegleria, Acanthamoeba, Balamuthia and Sappinia are known appearing opportunistic and also fatal protozoa in humans and other animals. They are widely distributed in soil and water in the world. They cause “Primer Amoebic Meningoencephalitis” the host immune response to these protist pathogens differs from each other to evidence by the postmortem laboratory findings from the affected patients. This review was performed with a search in Medline, PubMed, Science Direct, Ovid, and Scopus literatures by the search terms of “pathogenic free-living amoeba infections”. Analysis of a detailed review and literature shown that Naegleria fowleri, Acanthamoeba and Balamuthia and also Sappinia sp. infections are causing extensive brain damage to the host immune response. In human infection due to related to brain, skin, lung and eyes have increased significantly during the last years. They have different effects on epidemiology, immunology, pathology, and clinical features of the infections produced. This particular review planned to raise awareness about free-living amoeba, which found in a patient who applied to ESOGU Hospital Neurology Clinic because of suddenly unconsciousness and coma and diagnosed with Naegleria fowleri. Clinicians should be aware of PAM infections and include in differential diagnosis of meningoencephalitis. PAM should be suspected in young adults and children with acute neurological symptoms as described below and recent exposure to fresh water. -

Acta Protozool
Acta Protozool. (2015) 54: 45–51 www.ejournals.eu/Acta-Protozoologica ACTA doi:10.4467/16890027AP.15.004.2191 PROTOZOOLOGICA Electron Microscopical Investigations of a New Species of the Genus Sappinia (Thecamoebidae, Amoebozoa), Sappinia platani sp. nov., Reveal a Dictyosome in this Genus Claudia WYLEZICH1, Julia WALOCHNIK2, Daniele CORSARO3, Rolf MICHEL4, Alexander KUDRYAVTSEV5 1Department of General Ecology, Zoological Institute, University of Cologne, Germany; present address: Leibniz-Institute for Baltic Sea Research Warnemünde, Rostock, Germany; 2Molecular Parasitology, Institute of Specific Prophylaxis and Tropical Medicine, Medical University of Vienna, Austria; 3CHLAREAS – Chlamydia Research Association, Vandoeuvre-lès-Nancy, France; 4Central Institute of the Federal Armed Forces Medical Services, Department of Microbiology (Parasitology) Koblenz, Germany; 5Department of Invertebrate Zoology, Faculty of Biology, St. Petersburg State University, Russia Abstract. The genus Sappinia belongs to the family Thecamoebidae within the Discosea (Amoebozoa). For long time the genus comprised only two species, S. pedata and S. diploidea, based on morphological investigations. However, recent molecular studies on gene sequences of the small subunit ribosomal RNA (SSU rRNA) gene revealed a high genetic diversity within the genus Sappinia. This indicated a larger species richness than previously assumed and the establishment of new species was predicted. Here, Sappinia platani sp. nov. (strain PL- 247) is described and ultrastructurally investigated. This strain was isolated from the bark of a sycamore tree (Koblenz, Germany) like the re-described neotype of S. diploidea. The new species shows the typical characteristics of the genus such as flattened and binucleate tro- phozoites with a differentiation of anterior hyaloplasm and without discrete pseudopodia as well as bicellular cysts. -
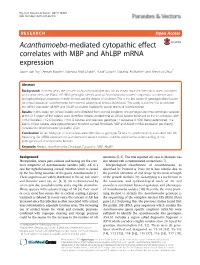
Acanthamoeba-Mediated Cytopathic Effect Correlates with MBP And
Ng et al. Parasites & Vectors (2017) 10:625 DOI 10.1186/s13071-017-2547-0 RESEARCH Open Access Acanthamoeba-mediated cytopathic effect correlates with MBP and AhLBP mRNA expression Sook-Luan Ng1, Anisah Nordin2, Norzana Abd Ghafar3, Yusof Suboh2, Noraina Ab Rahim2 and Kien-Hui Chua1* Abstract Background: In recent years, the concern of Acanthamoeba keratitis has increased since the infection is often associated with contact lens use. Partial 18S rRNA genotypic identification of Acanthamoeba isolates is important to correlate with pathophysiological properties in order to evaluate the degree of virulence. This is the first report of genotypic identification for clinical isolates of Acanthamoeba from corneal scrapings of keratitis in Malaysia. This study is also the first to correlate the mRNA expression of MBP and AhLBP as virulent markers for axenic strains of Acanthamoeba. Results: In this study, ten clinical isolates were obtained from corneal scrapings. Rns genotype and intra-genotypic variation at the DF3 region of the isolates were identified. Results revealed that all clinical isolates belonged to the T4 genotype, with T4/6 (4 isolates), T4/2 (3 isolates), T4/16 (2 isolates) and one new genotype T4 sequence (T4/36), being determined. The axenic clinical isolates were cytopathogenic to rabbit corneal fibroblasts. MBP and AhLBP mRNA expression are directly correlated to Acanthamoeba cytopathic effect. Conclusions: All ten Malaysian clinical isolates were identified as genotype T4 which is predominantly associated with AK. Measuring the mRNA expression of Acanthamoeba virulent markers could be useful in the understanding of the pathogenesis of Acanthamoeba keratitis. Keywords: Keratitis, Acanthamoeba, Genotype, Cytopathic, MBP, AhLBP Background infections [5, 6]. -

Free-Living Amoebae and Central Nervous System Infection: Report of Seven Cases
American Journal of Infectious Diseases Case Reports Free-Living Amoebae and Central Nervous System Infection: Report of Seven Cases Alcalá Martínez Enrique, Gaona Flores Verónica A., Paz Ayar Nibardo and González Guerra Eduardo Hospital de Infectología, Centro Médico Nacional La Raza, Mexico Article history Abstract: The Free-Living Amoeba (FLA) is an opportunistic Received: 27-09-2019 protozoan with a cosmopolitan distribution that can cause Central Revised: 07-12-2019 Nervous System (CNS) infection. It develops in relatively stagnant Accepted: 12-12-2019 waters such as swimming pools, lagoons and ponds but only species belonging to the genera Hartmannella, Naegleria, Acanthamoeba and Corresponding Author: Alcalá Martínez Enrique Balamuthia have been found in humans. The resulting pathology is Hospital de Infectología, highly lethal due to the lack of effective treatment. The aim of this Centro Médico Nacional La study is to describe a series of neuroinfection cases treated at the Raza, Mexico Hospital de Infectología in Mexico City. This is a descriptive study Email: [email protected] conducted between July 2008 and June 2016. It includes all patients admitted with signs and symptoms of meningoencephalitis and a laboratory work-up confirming the presence of FLA trophozoites in Cerebrospinal Fluid (CSF). Statistical Analysis. Nominal variables are reported as relative frequencies and quantitative variables, as medians, maximum and minimum. Seven cases were identified, 43% of which were male. The median number of days between exposure and symptom development was nine days. The most frequent symptoms were: Headache 57%, vomiting 29%, fever 57%, meningeal irritation 43% and altered consciousness 86%. Three of the seven analyzed cases died and one case was also HIV positive. -
Comprehensive Phylogenetic Reconstruction of Amoebozoa Based on Concatenated Analyses of SSU-Rdna and Actin Genes
Smith ScholarWorks Biological Sciences: Faculty Publications Biological Sciences 8-2-2011 Comprehensive Phylogenetic Reconstruction of Amoebozoa Based on Concatenated Analyses of SSU-rDNA and Actin Genes Daniel J.G. Lahr University of Massachusetts Amherst Jessica Grant Smith College Truc Nguyen Smith College Jian Hua Lin Smith College Laura A. Katz Smith College, [email protected] Follow this and additional works at: https://scholarworks.smith.edu/bio_facpubs Part of the Biology Commons Recommended Citation Lahr, Daniel J.G.; Grant, Jessica; Nguyen, Truc; Lin, Jian Hua; and Katz, Laura A., "Comprehensive Phylogenetic Reconstruction of Amoebozoa Based on Concatenated Analyses of SSU-rDNA and Actin Genes" (2011). Biological Sciences: Faculty Publications, Smith College, Northampton, MA. https://scholarworks.smith.edu/bio_facpubs/121 This Article has been accepted for inclusion in Biological Sciences: Faculty Publications by an authorized administrator of Smith ScholarWorks. For more information, please contact [email protected] Comprehensive Phylogenetic Reconstruction of Amoebozoa Based on Concatenated Analyses of SSU- rDNA and Actin Genes Daniel J. G. Lahr1,2, Jessica Grant2, Truc Nguyen2, Jian Hua Lin2, Laura A. Katz1,2* 1 Graduate Program in Organismic and Evolutionary Biology, University of Massachusetts, Amherst, Massachusetts, United States of America, 2 Department of Biological Sciences, Smith College, Northampton, Massachusetts, United States of America Abstract Evolutionary relationships within Amoebozoa have been the subject