YOUR VIEWS ABOUT LIVING WITH HIV
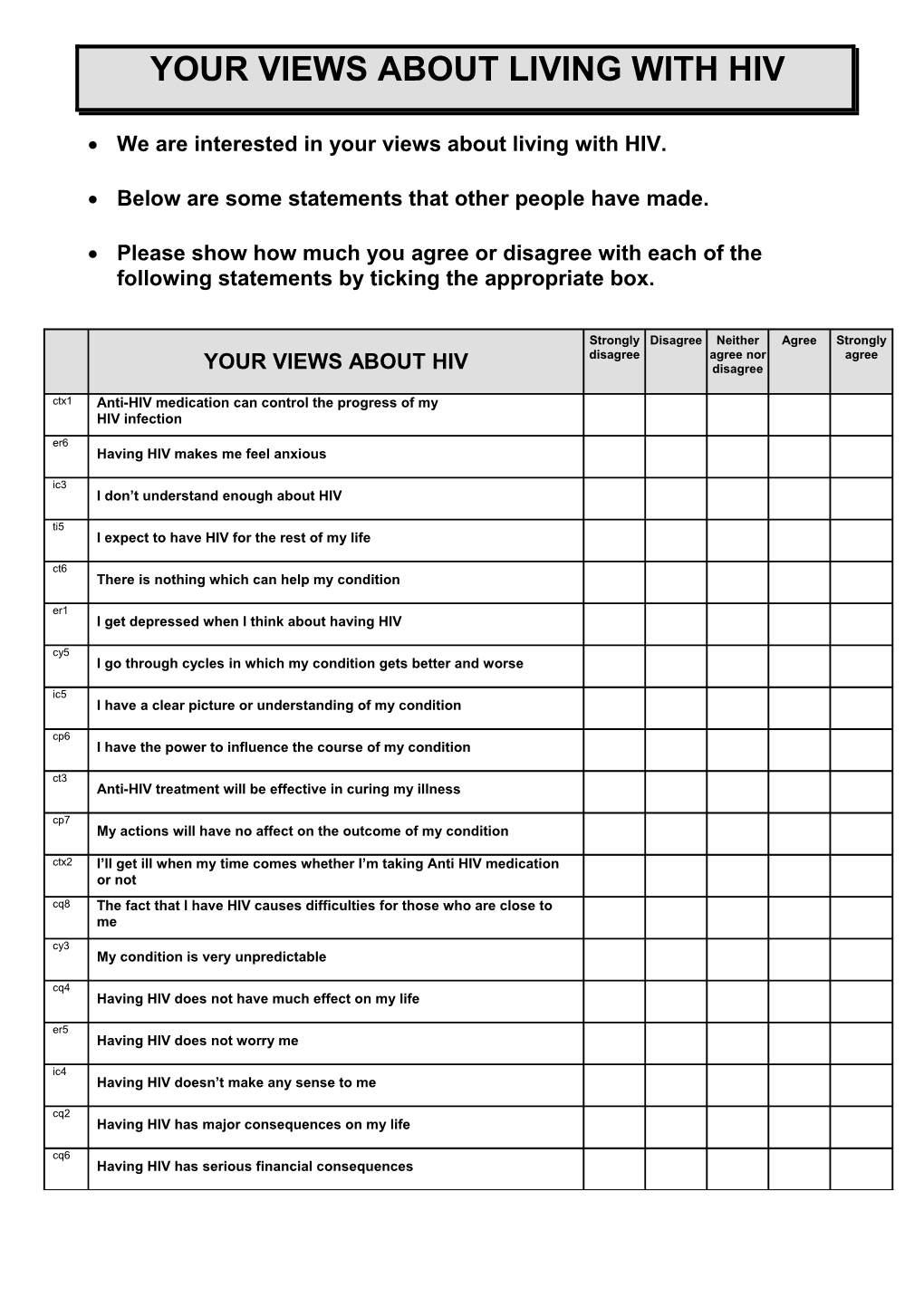
We are interested in your views about living with HIV.
Below are some statements that other people have made.
Please show how much you agree or disagree with each of the following statements by ticking the appropriate box.
Strongly Disagree Neither Agree Strongly disagree agree nor agree YOUR VIEWS ABOUT HIV disagree ctx1 Anti-HIV medication can control the progress of my HIV infection er6 Having HIV makes me feel anxious ic3 I don’t understand enough about HIV ti5 I expect to have HIV for the rest of my life ct6 There is nothing which can help my condition er1 I get depressed when I think about having HIV cy5 I go through cycles in which my condition gets better and worse ic5 I have a clear picture or understanding of my condition cp6 I have the power to influence the course of my condition ct3 Anti-HIV treatment will be effective in curing my illness cp7 My actions will have no affect on the outcome of my condition ctx2 I’ll get ill when my time comes whether I’m taking Anti HIV medication or not cq8 The fact that I have HIV causes difficulties for those who are close to me cy3 My condition is very unpredictable cq4 Having HIV does not have much effect on my life er5 Having HIV does not worry me ic4 Having HIV doesn’t make any sense to me cq2 Having HIV has major consequences on my life cq6 Having HIV has serious financial consequences YOUR VIEWS ABOUT LIVING WITH HIV
Strongly Disagree Neither Agree Strongly disagree agree nor agree YOUR VIEWS ABOUT HIV disagree
ic2 The HIV virus is a mystery to me
cq1 My illness is a serious condition
ti2 My condition is likely to be permanent rather than temporary
er8 Having HIV makes me feel afraid
er4 Having HIV makes me feel angry
cq5 Having HIV strongly affects the way others see me
ti1 My condition will improve in time
cy2 My symptoms come and go in cycles
cp5 Nothing I do will affect my illness
cp4 The course of my condition depends on me
ct4 The negative effects of my illness can be prevented by Anti HIV therapy
ic1 The symptoms of my condition are puzzling to me
cy1 The symptoms of my condition change a great deal from day to day
cp1 There is a lot which I can do to control my condition
ct2 There is very little that can be done to improve my condition
cp2 What I do can determine whether my condition gets better or worse
er3 When I think about having HIV I get upset
ct5 Anti HIV medication can control my condition
NB. The items below were added as extra timeline items following our cross-sectional study. They are not yet validated.
tlx1 I expect my condition to get better quickly
tlx2 I expect my condition to get better slowly
tlx3 I expect my state of health to remain how it is for the foreseeable future
tlx4 I expect my condition to get worse slowly
tlx5 I expect my condition to get worse quickly YOUR EXPERIENCE OF SYMPTOMS ASSOCIATED WITH HIV
Listed below are a number of symptoms that you may or may not have experienced since being diagnosed with HIV.
We are interested in how you are feeling AT PRESENT.
Please rate the severity of any symptoms you are currently experiencing by circling the appropriate number on the scale, where 1 indicates very mild and 5 indicates very severe.
Please only rate the symptoms that you believe are a result of HIV and NOT those that you believe are due to your medication.
Are you currently experiencing this symptom If yes, please rate the symptom severity very as a result of having HIV? very mild mild moderate severe severe ie1 Pain Yes No 1 2 3 4 5 ie2 Sore throat Yes No 1 2 3 4 5 ie3 Nausea Yes No 1 2 3 4 5 ie4 Breathlessness Yes No 1 2 3 4 5 ie5 Weight loss Yes No 1 2 3 4 5 ie6 Fatigue Yes No 1 2 3 4 5 ie7 Stiff Joints Yes No 1 2 3 4 5 ie8 Sore eyes Yes No 1 2 3 4 5 ie9 Wheezing Yes No 1 2 3 4 5 ie10 Headaches Yes No 1 2 3 4 5 ie11 Upset stomach Yes No 1 2 3 4 5 ie12 Sleep difficulties Yes No 1 2 3 4 5 ie13 Dizziness Yes No 1 2 3 4 5 ie14 Loss of strength Yes No 1 2 3 4 5 ie15 Night sweats Yes No 1 2 3 4 5 ie16 Diarrhoea Yes No 1 2 3 4 5 ie17 Feeling faint Yes No 1 2 3 4 5 YOUR EXPERIENCE OF SYMPTOMS ASSOCIATED WITH HIV
Are you currently experiencing this symptom If yes, please rate the symptom severity very as a result of having HIV? very mild mild moderate severe severe ie18 Fever Yes No 1 2 3 4 5 ie19 Sexual problems Yes No 1 2 3 4 5 ie20 Loss of appetite Yes No 1 2 3 4 5 ie21 Skin problems Yes No 1 2 3 4 5 ie22 Altered sensation in hands or feet Yes No 1 2 3 4 5 ie23 Stomach pain Yes No 1 2 3 4 5
If you have experienced any other symptoms recently that you believe may have been associated with HIV, please write them in the table below
As before, please rate the severity of any symptoms by circling the appropriate number on the scale, where 1 indicates ‘very mild’ and 5 indicates ‘very severe’.
Please rate the severity of each Symptom symptom severity very very mild mild moderate severe severe
Ie24 Yes No 1 2 3 4 5
Ie25 Yes No 1 2 3 4 5
Ie26 Yes No 1 2 3 4 5
Ie27 Yes No 1 2 3 4 5
Ie28 Yes No 1 2 3 4 5
Ie29 Yes No 1 2 3 4 5 YOUR EXPERIENCE OF SYMPTOMS ASSOCIATED WITH COMBINATION THERAPY
Listed below are a number of symptoms that you may or may not have experienced since you started taking combination therapy.
We are interested in how you are feeling AT PRESENT.
Please rate the severity of any symptoms you are currently experiencing by circling the appropriate number on the scale, where 1 indicates very mild and 5 indicates very severe.
Please only rate the symptoms that you believe are a result of taking combination therapy.
Are you currently experiencing this symptom If yes, please rate the symptom severity very as a result of taking combination therapy? very mild moderat severe severe mil e t-ie1 Pain Yes No 1 2 3 4 5 t-ie2 Sore throat Yes No 1 2 3 4 5 t-ie3 Nausea Yes No 1 2 3 4 5 t-ie4 Breathlessness Yes No 1 2 3 4 5 t-ie5 Weight loss Yes No 1 2 3 4 5 t-ie6 Fatigue Yes No 1 2 3 4 5 t-ie7 Stiff Joints Yes No 1 2 3 4 5 t-ie8 Sore eyes Yes No 1 2 3 4 5 t-ie9 Wheezing Yes No 1 2 3 4 5 t-ie10 Headaches Yes No 1 2 3 4 5 t-ie11 Upset stomach Yes No 1 2 3 4 5 t-ie12 Sleep difficulties Yes No 1 2 3 4 5 t-ie13 Dizziness Yes No 1 2 3 4 5 t-ie14 Loss of strength Yes No 1 2 3 4 5 t-ie15 Night sweats Yes No 1 2 3 4 5 t-ie16 Diarrhoea Yes No 1 2 3 4 5 t-ie17 Feeling faint Yes No 1 2 3 4 5 YOUR EXPERIENCE OF SYMPTOMS ASSOCIATED WITH COMBINATION THERAPY
Are you currently experiencing this symptom If yes, please rate the symptom severity very as a result of taking combination therapy? very mild moderat severe severe mil e t-Ie18 Fever Yes No 1 2 3 4 5 t-ie19 Sexual problems Yes No 1 2 3 4 5 t-ie20 Loss of appetite Yes No 1 2 3 4 5 t-ie21 Skin problems Yes No 1 2 3 4 5 t-ie22 Altered sensation in hands or feet Yes No 1 2 3 4 5 t-ie23 Stomach pain Yes No 1 2 3 4 5
If you have experienced any other symptoms recently that you believe may be a result of taking combination therapy, please write them in the table below
As before, please rate the severity of any symptoms by circling the appropriate number on the scale, where 1 indicates ‘very mild’ and 5 indicates ‘very severe’.
Please rate the severity of each Symptom symptom severity very very mild mild moderate severe severe t-ie24 Yes No 1 2 3 4 5 t-ie25 Yes No 1 2 3 4 5 t-ie26 Yes No 1 2 3 4 5 t-ie27 Yes No 1 2 3 4 5 t-ie28 Yes No 1 2 3 4 5 t-ie29 Yes No 1 2 3 4 5
V. Cooper, R. Horne, D. Buick, & J. Weinman. Centre for Health Care Research, University of Brighton, 1 Great Wilkins, Falmer, Brighton, BN1 9PH, UK.