When Doing TRIAGE, You MUST Protect Yourself and Your Buddy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Paramedic National EMS Education Standard
NORTHWEST COMMUNITY EMERGENCY MEDICAL SERVICES SYSTEM CCCooonnntttiiinnnuuuiiinnnggg EEEddduuucccaaatttiiiooonnn SSSeeepppttteeemmmbbbeeerrr 222000111222 EEyyee && EEaarr DDiissoorrddeerrss && TTrraauummaa Questions/comments are welcome. Please direct to Jen Dyer, RN, EMT-P EMS Educator NWC EMSS Con-Ed Eye and Ear Disorders and Trauma September 2012 – page 1 Paramedic National EMS Education Standard Integrates assessment findings with principles of pathophysiology to formulate a field impression and implement a treatment/disposition plan for patients with eye and ear disorders/trauma. Objectives: Upon completion of the class and review of the independent study materials and post-test question bank, each participant will do the following with a degree of accuracy that meets or exceeds the standards established for their scope of practice: 1. Identify the anatomical structures of the eye and describe the corresponding physiologic function of each. (C) 2. Explain the physiology of normal vision. (C) 3. Identify the anatomic structures of the ear and describe the corresponding physiologic function of each. (C) 4. Explain the physiology of normal hearing. (C) 5. Explain the physiology of equilibrium. (C) 6. Select and discuss maneuvers for assessing eye structures and functions (C) and demonstrate a thorough EMS assessment of ocular structures, visual acuity, pupils and ocular movements. (P) 7. Distinguish abnormal assessment findings/conditions of the eye: blurred vision, diplopia, photophobia, changes in vision, flashing, pupil exam, Adie’s pupil, oculomotor nerve paralysis, Horner’s Syndrome, blindness, deviation/paralytic strabismus, orbit fracture, cataracts, conjunctivitis, color blindness, near sightedness, farsightedness, astigmatism, amblyopia, burns of the eye, corneal abrasions, foreign body, inflammation of the eyelid, glaucoma, hyphema, iritis, orbital cellulitis, macular degeneration and trauma. -

ABCDE Approach
The ABCDE and SAMPLE History Approach Basic Emergency Care Course Objectives • List the hazards that must be considered when approaching an ill or injured person • List the elements to approaching an ill or injured person safely • List the components of the systematic ABCDE approach to emergency patients • Assess an airway • Explain when to use airway devices • Explain when advanced airway management is needed • Assess breathing • Explain when to assist breathing • Assess fluid status (circulation) • Provide appropriate fluid resuscitation • Describe the critical ABCDE actions • List the elements of a SAMPLE history • Perform a relevant SAMPLE history. Essential skills • Assessing ABCDE • Needle-decompression for tension • Cervical spine immobilization pneumothorax • • Full spine immobilization Three-sided dressing for chest wound • • Head-tilt and chin-life/jaw thrust Intravenous (IV) line placement • • Airway suctioning IV fluid resuscitation • • Management of choking Direct pressure/ deep wound packing for haemorrhage control • Recovery position • Tourniquet for haemorrhage control • Nasopharyngeal (NPA) and oropharyngeal • airway (OPA) placement Pelvic binding • • Bag-valve-mask ventilation Wound management • • Skin pinch test Fracture immobilization • • AVPU (alert, voice, pain, unresponsive) Snake bite management assessment • Glucose administration Why the ABCDE approach? • Approach every patient in a systematic way • Recognize life-threatening conditions early • DO most critical interventions first - fix problems before moving on -
TCCC CLS Skill Instructions Mod 7 25 JAN 20
MODULE 07: AIRWAY MANAGEMENT IN TFC SKILL INSTRUCTIONS 25 JAN 2020 COMBAT LIFESAVER (CLS) TACTICAL COMBAT CASUALTY CARE SKILL INSTRUCTIONS HEAD-TILT/CHIN-LIFT INSTRUCTION TASK: Open an airway using the head-tilt/chin-lift maneuver CONDITION: Given a simulated scenario where a casualty and responder are in combat gear and the casualty is unconscious without a patent airway STANDARD: EffeCtively open the airway by performing the head-tilt/chin-lift maneuver following all steps and measures correctly without Causing further harm to the Casualty EQUIPMENT: N/A PERFORMANCE MEASURES: step-by-step instructions NOTE: Do not use if a spinal or neck injury is suspected. 01 Roll the Casualty onto their back, if necessary, and place them on a hard, flat surface. 02 Kneel at the level of the Casualty’s shoulders. Position yourself at the side of the Casualty. 03 Open the mouth and looK for visible airway obstruCtions (e.g., laCerations, obstructions, broken teeth, burns, or swelling or other debris, such as vomit). NOTE: If foreign material or vomit is in the mouth, remove it as quiCKly as possible. NOTE: Do not perform a blind finger sweep. 04 PlaCe one hand on the Casualty's forehead and apply firm, backward pressure with the palm to tilt the head back. 05 PlaCe the fingertips of the other hand under the bony part of the lower jaw and lift, bringing the Chin forward. NOTE: Do not use the thumb to lift the chin. 06 While maintaining the open airway position, place an ear over the casualty's mouth and nose, looking toward the chest and stomaCh. -

Emergency Medical Responder Febuary Pre Work
EMERGENCY MEDICAL RESPONDER FEBUARY PRE WORK Name___________________________________ MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) When moving or lifting a patient, you should: 1) A) determine the patient's chief complaint. B) ask bystanders to help. C) use good body mechanics. D) provide emotional support. 2) You have an ethical responsibility to: 2) A) read professional publications. B) maintain your skills and knowledge. C) be ready to perform at all times. D) all of the above. 3) As an Emergency Medical Responder you may be at risk of exposure to an infectious disease when 3) you: A) are talking on the phone. B) handle equipment that has blood on it. C) wear gloves when you care for a patient. D) respond to an emergency. 4) In the anatomical position, the respiratory system would be ________ to the digestive system. 4) A) superior B) anterior C) posterior D) inferior 5) You have a patient with a suspected spinal injury. The best method for movement to the backboard 5) device would be: A) direct carry. B) log roll. C) shoulder drag. D) extremity lift. 6) For patients who have a suspected spinal injury, you should use: 6) A) head-tilt. B) jaw thrust. C) head-tilt, chin-lift. D) chin-lift. 7) You have a patient who experienced an approximately 16-foot fall from the roof while working on 7) the gutters. He is found supine on the driveway and does not respond to verbal or painful stimuli. After assessing the scene and taking spinal restriction, you should proceed to the: A) initial assessment. -
5 Minute EMS Clinic-The First Five Minutes V2
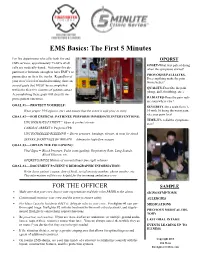
EMS Basics: The First 5 Minutes For fire departments who offer both fire and OPQRST EMS services, approximately 75-80% of all ONSET-What was patient doing calls are medically-based. Not every fire de- when the symptoms started? partment is fortunate enough to have EMT’s or PROVOKES/PALLIATES- paramedics on their fire trucks. Regardless of Does anything make the pain your crew’s level of medical training, there are worse/better? several goals that MUST be accomplished QUALITY-Describe the pain within the first five minutes of patient contact. (sharp, dull, throbbing, etc.). Accomplishing these goals will directly im- prove patient outcomes. RADIATES-Does the pain radi- ate somewhere else? GOAL #1—-PROTECT YOURSELF: SEVERITY-On a scale from 1- Wear proper PPE (gloves, etc.) and ensure that the scene is safe prior to entry. 10 with 10 being the worst pain, rate your pain level. GOAL #2—-FOR CRITICAL PATIENTS, PERFORM IMMEDIATE INTERVENTIONS: TIME-When did the symptoms UNCONSCIOUS PATIENT = Open & protect airway start? CARDIAC ARREST = Perform CPR UNCONTROLLED BLEEDING = Direct pressure, bandage, elevate, & treat for shock SEVERE SHORTNESS OF BREATH = Administer high-flow oxygen GOAL #3—-OBTAIN THE FOLLOWING: Vital Signs = Blood Pressure, Pulse (rate/quality), Respiratory Rate, Lung Sounds, Blood Glucose, etc. OPQRST/SAMPLE History of current illness (see right column) GOAL #4—-DOCUMENT PATIENT’S DEMOGRAPHIC INFORMATION: Write down patient’s name, date of birth, social security number, phone number, etc. This information will be very helpful for the incoming ambulance crew. FOR THE OFFICER SAMPLE Make sure that your crew knows your expectations and their roles PRIOR to the alarm. -

New Spinal Recovery Position June 2019
New Spinal Recovery Position June 2019 Background Since first publication, the Qualsafe First Aid Made Easy A4 sized First Aid Book has included methods for turning an unconscious casualty with a suspected spinal injury in order to protect the airway – a “spinal recovery position”. Originally a log-roll was included, which requires the first aider to recruit the help of three other people, and more recently a spinal recovery position that required the help of one additional person was included. Injury to the lumbar or thoracic region present in 71.4% of spinal injury patients,8 so the guidance for placing someone into the spinal recovery position has always differed from the ‘traditional’ recovery position, in order to minimise torsion (twisting) of the spine, which is impossible to avoid when pulling a casualty onto their side using only the knee. This topic is only taught to first aiders who attend a course that specifically covers spinal injury on the syllabus (e.g. First Aid at Work, but not Emergency First Aid at Work). The problem with the previous spinal recovery position It is important to note that turning an unconscious casualty onto their side to protect the airway is an emergency procedure that a first aider will have to perform in stressful circumstances. The optimum treatment for a supine spinal injury patient is to keep the casualty on their back and provide manual in-line stabilisation (MILS) with the head and neck in a neutral alignment, whilst continually monitoring breathing. 1,2 Ideally the first aider who can stay with the casualty should only turn the them if they become concerned about the airway. -

2012 2013 First Aid Contest Rules
2016 FIRST AID CONTEST RULES INDEX Section II Title Page Rules Governing the 2016 First Aid Contest ........................................................................ 1 Scorecard A Discounts ............................................................................................................ 8 Interpretations of Scorecard B (Artificial Ventilation/Cardiopulmonary Resuscitation). ........................................................................................................................ 12 Skill Sheets Initial Assessment .................................................................................................................. 15 Patient Assessment ................................................................................................................ 16 Automated External Defibrillator ........................................................................................ 19 One-Person CPR (Manikin Only) ........................................................................................ 18 Two-Rescuer CPR (Manikin Only) ...................................................................................... 20 Mouth-to-Mask Resuscitation .............................................................................................. 24 Airway Obstruction ............................................................................................................... 25 Sucking Chest Wound .......................................................................................................... -
Speaker Notes Module 07 – Airway Management In
COMBAT LIFESAVER TACTICAL COMBAT CASUALTY CARE (TCCC) SPEAKER NOTES MODULE 07 – AIRWAY MANAGEMENT IN TFC SLIDE 1 – TITLE SLIDE SLIDE 2 – TCCC ROLES Tactical Combat Casualty Care is broken up into 4 roles of care. The most basic is taught to All Service Members (ASM), which is the absolute basics of hemorrhage control and to recognize more serious problems. You are in the Combat Lifesaver (CLS) role. This teaches you more advanced care to treat the most common causes of death on the battlefield, and to recognize, prevent, and communicate with medical personnel the life-threatening complications of these injuries. The Combat Medic/Corpsman role has much more advanced and invasive care requiring significantly more medical knowledge and skills. Finally, the last role is for combat paramedics and advanced providers, to provide the most sophisticated care to keep our wounded warriors alive and get them to definitive care. Your role as a combat lifesaver is to treat the most common causes of death on the battlefield, which are massive hemorrhage and airway/respiratory problems. In addition, you are given the skills to prevent complications and treat other associated but not immediately life-threatening injuries. TCCC CLS SPEAKER NOTES #TCCC-CLS-14-01 25 JAN 20 COMBAT LIFESAVER TACTICAL COMBAT CASUALTY CARE (TCCC) SPEAKER NOTES SLIDE 3 – TLO/ELO The TCCC-CLS course is built on a foundation of learning objectives. These objectives lay out the basic structure of the course and describe the knowledge and skills you are expected to acquire by the end of the course. The module has one Terminal Learning Objective, or TLO. -
Medical Standard Operating Guidelines (Released May 2016)
CENTURY AMBULANCE SERVICE, INC. Medical Standard Operating Guidelines (Released May 2016) Authorization These guidelines and treatment guidelines were developed and reviewed under the authorization of the below-signed Medical Director in accordance with Florida Statute 401 and Chapter 64J-1 of the Florida Administrative Code. Changes to these guidelines can only be made with the authorization of the Medical Director and Century Ambulance Service, Inc. Signature on File David Murray, M.D. Medical Director These Medical Standard Operating Guidelines (MSOG) as reviewed and signed above by Century Ambulance Service, Inc.’s Medical Director supersede all previous memos, Emergency Medical Services Standard Operating Guidelines, Medical Standard Operating Guidelines, and Drug Listings. Century Ambulance Service, Inc. Medical Standard Operating Guidelines 1 Table of Contents (200.00) Authorization...................................................................................................................................... 1 Table of Contents (200.00) ................................................................................................................ 2 Introduction (200.02) ......................................................................................................................... 8 Reporting and Treating Patient Abuse / Neglect (205.00) ................................................................. 9 Clinical Quality Assurance Program Purpose and Overview (205.02)........................................... -

Emergency Drill Triage Kit Instruction Guide
Emergency Drill Triage Kit Instruction Guide During major emergencies schools must be prepared to be self-reliant This kit does not require because it is universally understood that local first responders will advanced training or be overwhelmed. Schools will need to be ready to rescue and treat equipment. The skills injured victims using only the skills and training of the school staff. This that this kit will review Emergency Drill Triage Kit was created in collaboration with the Pediatric are the same skills Disaster Resource and Training Center at Childrens Hospital Los Angeles. taught in Basic First Aid It is intended to support school personnel as they practice identifying, and CPR classes. reporting, transporting and treating injured victims. This kit is designed to help school personnel review their Basic First Aid training and practice those skills. m num ti b ic e v r Objects fell onto patient. 9 VISUAL CUES A key component of this kit is the 40 mock victim tags. These victim Cut on Non-bleeding scalp laceration; head and right foot swollen tags were created based on historical data of earthquake-related VICTIM INFORMATION and tender. rightEmergency Triage Drillfoot injuries. Experts from Childrens Hospital Los Angeles and Los Angeles pain. City Fire reviewed the mock victim scenarios and outlined first aid and medical responses. These victim tags represent the kinds of Mock Victim Tags injuries sustained by school aged children during an earthquake and 40 cards in clip pouches they are designed to review the First Aid procedures that could be Victim Checklist used during any traumatic emergency. -

View/Download
Backcountry First Aid: Prevention,Triage and Treatment Peter Heidmann DVM MPH Specialist: Equine Internal Medicine Montana Equine Equine Medicine and Surgery Board-certified Experts 406-388-8323 Dedicated to the highest quality care of horses Preparation = Prevention • Paperwork – Health Certificate, Coggins – Contact Information – Maps • Know your country • Tack – Well-fitted, well-suited • Fitness – Fatigue promotes injury – Lameness and myopathy – Colic and lacerations Triage: Lameness • Heat? Swelling? • Flexion Tests – Arthritis – Ligament Sprain • (Connects bone to bone) – Tendon Strain • (Connects muscle to bone) • 85% of lameness originates at/below fetlock – Digital Pulses • Stone Bruises • Sole Abscess • Fractured Coffin Bone (P3) Treatment: Lameness • Thermal Therapy – Ice Early -- Heat Late • Anti-inflammatory Medications – Phenylbutazone – Surpass • Limb Wraps – Minimize Swelling – Supports Soft Tissues – Extensive Padding is CRITICAL • Other Salves? Poultices? Sweats? Triage: Wounds • Location location location • Which wound is more serious? Triage: Wounds • Infection Control – Each round removes contamination: • Dirty water is better than mud • Clean water is better than dirty water • Sterile water is better than clean water – A clean wound is considered infected after 6 hours • 2 - 4 - 16 - 256 - 65,536 - 4,294,967,296!! – Antiseptic Solutions – Vaccinations – Antibiotics • Oral, Injectable, Topical • Ask your veterinarian… Triage: Eye Trauma • Use caution with “hi-line” • Eyelid Trauma • Corneal Trauma – Signs: • Squinting • Severe Tearing • Head-shyness Treatment: - Clean any wounds w/ Saline - Opthalmic Antibiotics - NO STEROID OINTMENTS! Triage: Hemorrhage Blood Loss: How Much is TOO Much?? Blood Volume is 8 - 10 % of Body Weight Eg 1000# horse = 450 Kg = 36-45 L Total Total loss of 1/10 is typically well-tolerated = 3.6 - 4.5 Liters = More than 1GALLON! Triage: Hemorrhage Treatment • Most Wounds stop bleeding spontaneously • Arterial vs. -

Principles and Practice of First Aid
CHAPTER 1: PRINCIPLES AND PRACTICE OF FIRST AID Definition of first aid 1. First aid refers to the actions taken in response to someone who is injured or suddenly taken ill 2. A first aider is a person who takes this action Aims of first aid ● Preserve life ● Prevent the condition from becoming worse ● Promote recovery Responsibilities and duties of first aider ● Give first aid to the casualty ● Keep a record of all treatment given ● Maintain the first aid box o Replenish contents regularly o ensure only first aid items are kept in the box Responding to emergency ● Be calm in your approach ● Be aware of risks to yourself and others ● Build and maintain trust ● Give early treatment ● Call appropriate help ● Remember your own needs 1 First Aid Priorities ● Assess a situation quickly and calmly ● Protect yourself and casualty from danger ● Prevent cross contamination ● Provide comfort and reassure the casualties ● Give early treatment, most serious (life-threatening) first ● Arrange appropriate help:- o Call 995 o Transfer to the care of a healthcare professional; or home Calling for ambulance ● Dial 995 ● State o Your telephone number o The exact location of incident o Type and gravity if the emergency o Number, gender and age of casualties o Details of any hazards Universal Precautions ● Wash your hands and wear disposable gloves ● Cover cuts and grazes with waterproof dressings ● Wear plastic apron and plastic glasses for eye protection ● Use a resuscitation mask (face shield or pocket mask) when giving rescue breaths ● Dispose all waste safely ● Do not touch a wound or the part of dressing that will touch a wound ● Do not breathe, cough or sneeze over the wound ● If you accidentally prick or cut your skin, or splash your eye, wash the area thoroughly and seek medical help immediately 2 CHAPTER 2: WOUNDS, BLEEDING AND SHOCK Basic Anatomy and Physiology of the circulatory system The heart and blood vessels ● The heart and blood vessels make up the circulatory system.