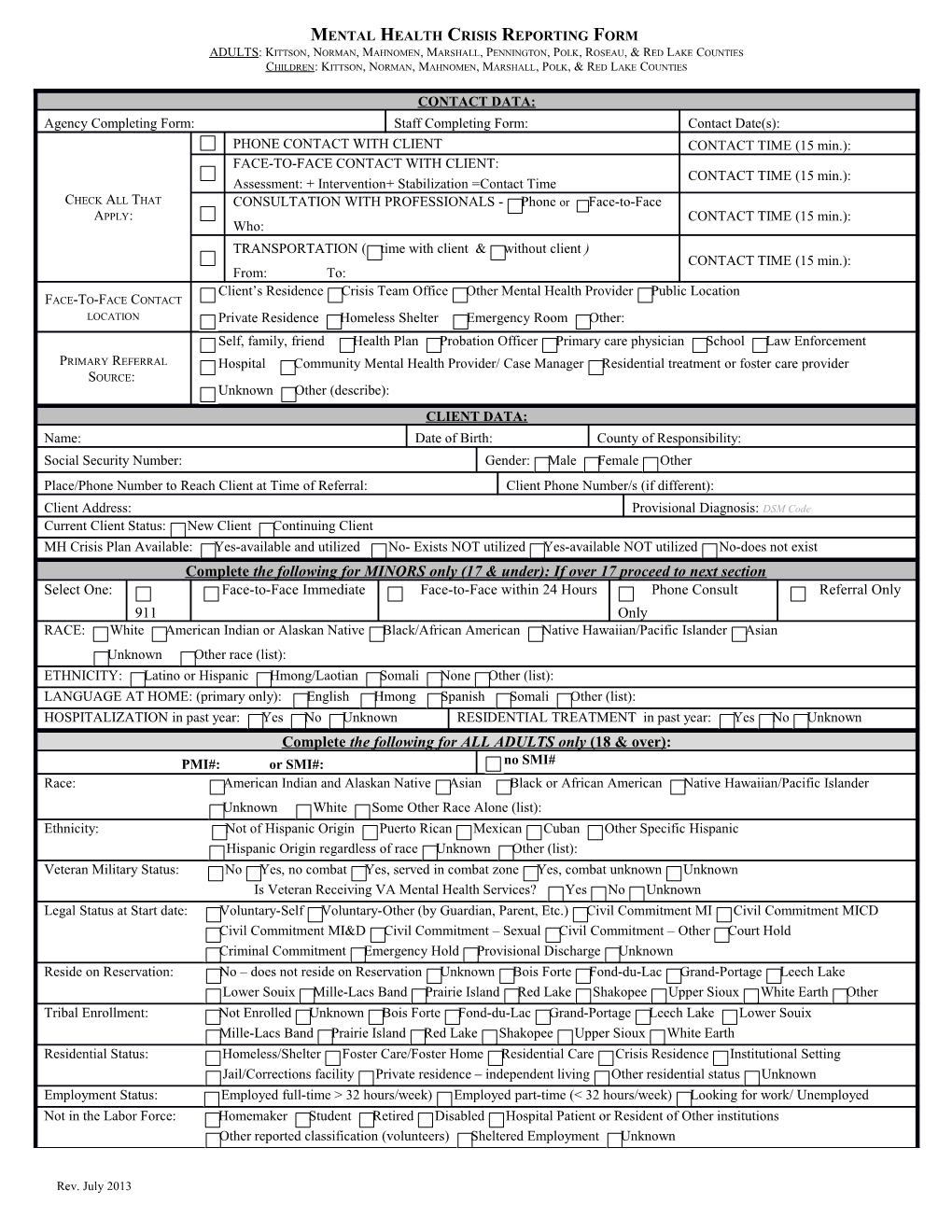
MENTAL HEALTH CRISIS REPORTING FORM ADULTS : KITTSON, NORMAN, MAHNOMEN, MARSHALL, PENNINGTON, POLK, ROSEAU, & RED LAKE COUNTIES CHILDREN : KITTSON, NORMAN, MAHNOMEN, MARSHALL, POLK, & RED LAKE COUNTIES
CONTACT DATA: Agency Completing Form: Staff Completing Form: Contact Date(s): PHONE CONTACT WITH CLIENT CONTACT TIME (15 min.): FACE-TO-FACE CONTACT WITH CLIENT: CONTACT TIME (15 min.): Assessment: + Intervention+ Stabilization =Contact Time CHECK ALL THAT CONSULTATION WITH PROFESSIONALS - Phone or Face-to-Face APPLY: CONTACT TIME (15 min.): Who: TRANSPORTATION ( time with client & without client ) CONTACT TIME (15 min.): From: To: Client’s Residence Crisis Team Office Other Mental Health Provider Public Location FACE-TO-FACE CONTACT LOCATION Private Residence Homeless Shelter Emergency Room Other: Self, family, friend Health Plan Probation Officer Primary care physician School Law Enforcement PRIMARY REFERRAL Hospital Community Mental Health Provider/ Case Manager Residential treatment or foster care provider SOURCE: Unknown Other (describe): CLIENT DATA: Name: Date of Birth: County of Responsibility: Social Security Number: Gender: Male Female Other Place/Phone Number to Reach Client at Time of Referral: Client Phone Number/s (if different): Client Address: Provisional Diagnosis: DSM Code Current Client Status: New Client Continuing Client MH Crisis Plan Available: Yes-available and utilized No- Exists NOT utilized Yes-available NOT utilized No-does not exist Complete the following for MINORS only (17 & under): If over 17 proceed to next section Select One: Face-to-Face Immediate Face-to-Face within 24 Hours Phone Consult Referral Only 911 Only RACE: White American Indian or Alaskan Native Black/African American Native Hawaiian/Pacific Islander Asian Unknown Other race (list): ETHNICITY: Latino or Hispanic Hmong/Laotian Somali None Other (list): LANGUAGE AT HOME: (primary only): English Hmong Spanish Somali Other (list): HOSPITALIZATION in past year: Yes No Unknown RESIDENTIAL TREATMENT in past year: Yes No Unknown Complete the following for ALL ADULTS only (18 & over): PMI#: or SMI#: no SMI# Race: American Indian and Alaskan Native Asian Black or African American Native Hawaiian/Pacific Islander Unknown White Some Other Race Alone (list): Ethnicity: Not of Hispanic Origin Puerto Rican Mexican Cuban Other Specific Hispanic Hispanic Origin regardless of race Unknown Other (list): Veteran Military Status: No Yes, no combat Yes, served in combat zone Yes, combat unknown Unknown Is Veteran Receiving VA Mental Health Services? Yes No Unknown Legal Status at Start date: Voluntary-Self Voluntary-Other (by Guardian, Parent, Etc.) Civil Commitment MI Civil Commitment MICD Civil Commitment MI&D Civil Commitment – Sexual Civil Commitment – Other Court Hold Criminal Commitment Emergency Hold Provisional Discharge Unknown Reside on Reservation: No – does not reside on Reservation Unknown Bois Forte Fond-du-Lac Grand-Portage Leech Lake Lower Souix Mille-Lacs Band Prairie Island Red Lake Shakopee Upper Sioux White Earth Other Tribal Enrollment: Not Enrolled Unknown Bois Forte Fond-du-Lac Grand-Portage Leech Lake Lower Souix Mille-Lacs Band Prairie Island Red Lake Shakopee Upper Sioux White Earth Residential Status: Homeless/Shelter Foster Care/Foster Home Residential Care Crisis Residence Institutional Setting Jail/Corrections facility Private residence – independent living Other residential status Unknown Employment Status: Employed full-time > 32 hours/week) Employed part-time (< 32 hours/week) Looking for work/ Unemployed Not in the Labor Force: Homemaker Student Retired Disabled Hospital Patient or Resident of Other institutions Other reported classification (volunteers) Sheltered Employment Unknown
Rev. July 2013
2 Highest Education: Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 Grade 6 Grade 7 Grade 8 Grade 9 Grade 10 Grade 11 Grade 12/GED Voc/Tech School College Freshman College Sophomore College Junior College Senior Graduate/Professional School Unknown
Education Enrollment Status: Enrolled Not Enrolled Unknown Number of Arrests in the past 30 days: 00-30 Unknown
Children under 18 years of age: Children Age Range(s): Children Reside with the Client: Children have Special Needs: Yes No 0-5 6-11 12-17 Full-time Part-time Not at all Yes No Unknown Unknown Unknown Unknown
Axis II: Axis III: Diagnostic Assessment Axis I: Axis V- GAF (301; 317-319; 999.9996- (001-289; 320-759; 780-999; Date:// (209-316; 999.9996-999.9997) (0-100 ) 997 Unknown 999.9997) V01-V 86; 999.9996-999.9998)
Substance Abuse Screening: Screened – Negative Screened – Positive Not Screened INCIDENT DATA: Suicidal (ideation) Suicidal (attempt) Self-Injurious Behaviors (non-suicidal) Anxiety/Panic Trauma (assault, loss, abuse) Aggressive, threatening, or homicidal behaviors Depression Situational Crisis Challenging, disruptive, out of control behavior Mania Psychotic or delusional (no threatening behaviors, non-assaultive) Other (MUST describe, e.g., grief, parenting concern, substance abuse) : Current Stressors/Nature of Problem/Current Symptoms/Risk Behaviors/Problems:
Is alcohol or drug use influencing the current mental health crisis? Yes No Prescription Medication(s) Known: OUTCOME: Brief Description of Outcome:
Client Whereabouts Known at Episode Closing? Yes No
Complete the following for MINORS only (17 & under) Complete the following for ADULTS only (18 & older) Immediate Disposition: Coordination Referrals Made (new services you Case Management Hospitalization (All that Apply) arranged, not services in place): Shelter Placement With Case Manager E.D./Psychiatric Hospital Not Receiving, Appoint.Arranged With CTSS Provider Already Receives, Sharing Info Emergency Foster Care Residential Treatment Not Receiving, Referral Declined Temporary residence with Other (list): Physician/Psychiatrist/CNS Already Receives, NOT Sharing Info relatives/friends Additional Mental Health Not Receiving, Not Referred Remained in current home Services Chemical Health Services Other (MUST specify): Other (Must Specify):
______Staff Signature Date Supervisor Signature Date
______Client Signature ( Refusal/List Reason above) Date County Director Signature/Approval Date
COMPLETE THE FOLLOWING SECTION ONLY FOR CHILDREN (17 & UNDER) RECEIVING STABILIZATION SERVICES:
Name (if given): Date of Birth: County of Responsibility: Contact Date:
*IF STABILIZATION SERVICES WERE PROVIDED FOR AN INDIVIDUAL AGED 0-17, PLEASE COMPLETE THE FOLLOWING:
Rev. July 2013
MENTAL HEALTH CRISIS REPORTING FORM ADULTS : KITTSON, NORMAN, MAHNOMEN, MARSHALL, PENNINGTON, POLK, ROSEAU, & RED LAKE COUNTIES CHILDREN : KITTSON, NORMAN, MAHNOMEN, MARSHALL, POLK, & RED LAKE COUNTIES CASII Score: SDQ Scores: Parent Self Teacher/Case Manager Other Services (all that apply) Curren Referrals Other Services (cont) Current Referrals t Individual Psychotherapy Residential Treatment Group Therapy Case Management (Children’s Mental Health) Family Psychotherapy Medication management – Psychiatrist Individual Skills Training Medication management – Primary care provider Group Skills Training Partial hospitalization Family Skills Training Inpatient hospital services Mental Health Behavioral Aide Support groups Day Treatment None/unknown
______Staff Signature Date
*PLEASE SEND FORM TO THE CRISIS COORDINATOR AT NWMHC 603 BRUCE ST. CROOKSTON, MN 56716 FOR PROCESSING
Rev. July 2013