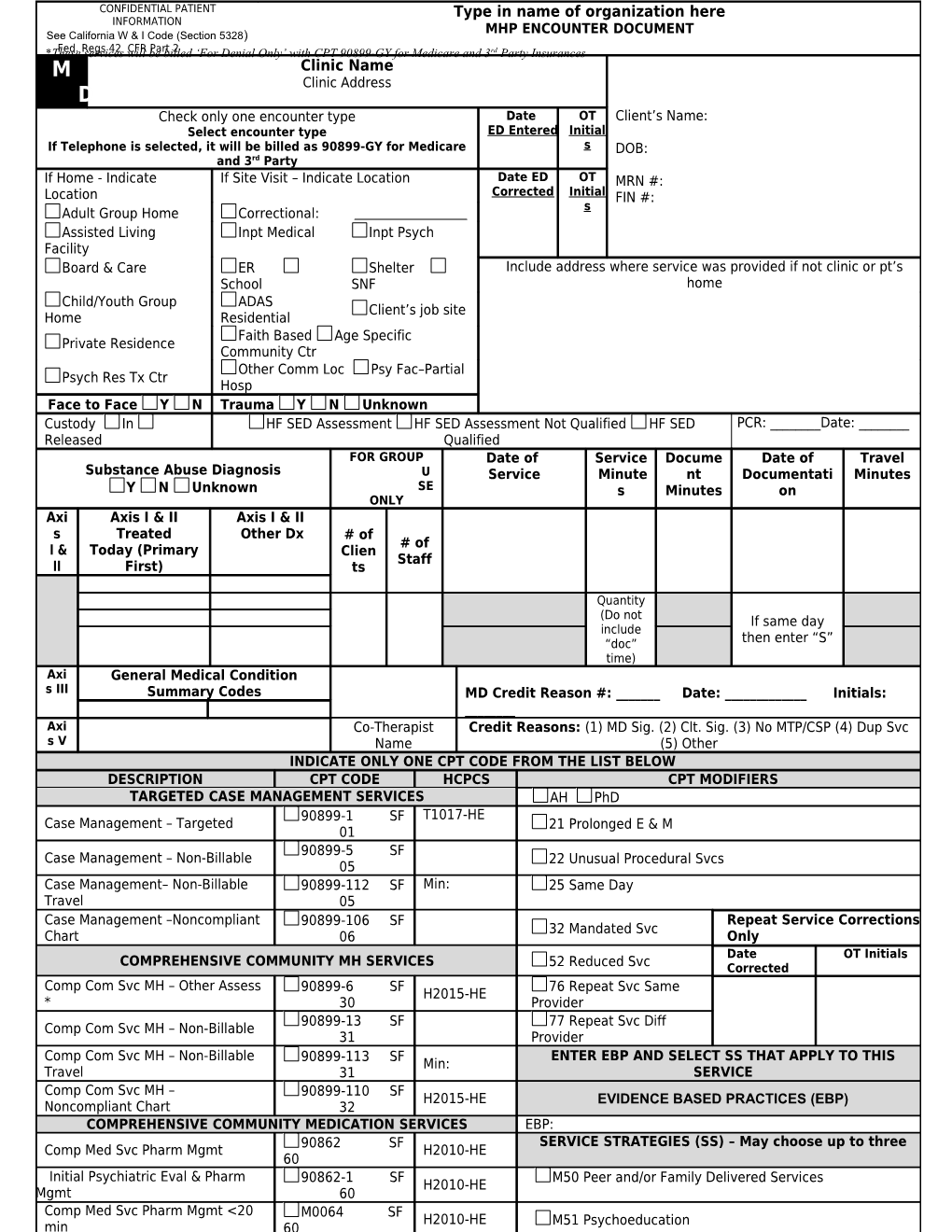
CONFIDENTIAL PATIENT Type in name of organization here INFORMATION See California W & I Code (Section 5328) MHP ENCOUNTER DOCUMENT *These Fed. Regsservices 42 willCFR bePart billed 2 ‘For Denial Only’ with CPT 90899-GY for Medicare and 3rd Party Insurances M Clinic Name Clinic Address D Check only one encounter type Date OT Client’s Name: Select encounter type ED Entered Initial If Telephone is selected, it will be billed as 90899-GY for Medicare s DOB: and 3rd Party If Home - Indicate If Site Visit – Indicate Location Date ED OT MRN #: Location Corrected Initial FIN #: s Adult Group Home Correctional:
Assisted Living Inpt Medical Inpt Psych Facility Board & Care ER Shelter Include address where service was provided if not clinic or pt’s School SNF home Child/Youth Group ADAS Client’s job site Home Residential Faith Based Age Specific Private Residence Community Ctr Other Comm Loc Psy Fac–Partial Psych Res Tx Ctr Hosp Face to Face Y N Trauma Y N Unknown Custody In HF SED Assessment HF SED Assessment Not Qualified HF SED PCR: ______Date: ______Released Qualified FOR GROUP Date of Service Docume Date of Travel Substance Abuse Diagnosis U Service Minute nt Documentati Minutes Y N Unknown SE s Minutes on ONLY Axi Axis I & II Axis I & II s Treated Other Dx # of # of I & Today (Primary Clien Staff II First) ts
Quantity (Do not If same day include then enter “S” “doc” time) Axi General Medical Condition s III Summary Codes MD Credit Reason #: ______Date: ______Initials: ______Axi Co-Therapist Credit Reasons: (1) MD Sig. (2) Clt. Sig. (3) No MTP/CSP (4) Dup Svc
s V Name (5) Other INDICATE ONLY ONE CPT CODE FROM THE LIST BELOW DESCRIPTION CPT CODE HCPCS CPT MODIFIERS TARGETED CASE MANAGEMENT SERVICES AH PhD 90899-1 SF T1017-HE Case Management – Targeted 21 Prolonged E & M 01 90899-5 SF Case Management – Non-Billable 22 Unusual Procedural Svcs 05 Case Management– Non-Billable 90899-112 SF Min: 25 Same Day Travel 05 Case Management –Noncompliant 90899-106 SF Repeat Service Corrections 32 Mandated Svc Chart 06 Only Date OT Initials COMPREHENSIVE COMMUNITY MH SERVICES 52 Reduced Svc Corrected Comp Com Svc MH – Other Assess 90899-6 SF 76 Repeat Svc Same H2015-HE * 30 Provider 90899-13 SF 77 Repeat Svc Diff Comp Com Svc MH – Non-Billable 31 Provider Comp Com Svc MH – Non-Billable 90899-113 SF ENTER EBP AND SELECT SS THAT APPLY TO THIS Min: Travel 31 SERVICE Comp Com Svc MH – 90899-110 SF H2015-HE EVIDENCE BASED PRACTICES (EBP) Noncompliant Chart 32 COMPREHENSIVE COMMUNITY MEDICATION SERVICES EBP: 90862 SF SERVICE STRATEGIES (SS) – May choose up to three Comp Med Svc Pharm Mgmt H2010-HE 60 Initial Psychiatric Eval & Pharm 90862-1 SF M50 Peer and/or Family Delivered Services H2010-HE Mgmt 60 Comp Med Svc Pharm Mgmt <20 M0064 SF H2010-HE M51 Psychoeducation min 60 MD Encounter Document (ED 5.0) (rev. 12/1/10) CONFIDENTIAL PATIENT INFORMATION Name: Error: Reference source not found See: Cal W & I Code (Section 5328) Clinic Name DOB: Clinic Address MRN#:
PSYCHIATRIC MEDICATION MONITORING RECORD – Page 1 of 2 MD/DO Name (Print) Date of Service Date Written (if late Error: Reference source not found entry) Service Documentation Travel time: Encounterminutes Type: Select encounter typetime Type of Service: Medication Language in which client received services, if other than English: Spanish Vietnamese Other (Specify)
Interpreter utilized? (Describe in Progress Note) 1. SUBJECTIVE & COLLATERAL DATA (Information from client and/or other sources (family, school, staff, caretakers, etc.)
See Next Page: 2. CURRENT MEDICATION & OBJECTIVE DATA Name of Medication / Dosage and Frequency Name of Medication / Dosage and Frequency
HR BP HT WT _ AIMS Completed N/A or Y N* (*Explain) Compliance: Y N* (*Explain) Adverse/Side Effects: Y* (*Explain) N Any New Physical Conditions/Concerns: Y* (*Explain) N Lab Tests Completed/Ordered: N/A or Y N* (*Explain) Satisfactory Response to Medication(s): Results of Lab Tests: Comments/Explanations: Initial ______See Next Page: ED 5.0 med mon 2pg. rev 9-28-10 Name: CONFIDENTIAL PATIENT INFORMATION See: Cal W & I Code (Section 5328) Clinic Name DOB: Clinic Address MRN#:
Psychiatric Medication Monitoring Record – Page 2 of 2 MD/DO Name (Print) Date of Service Date Written (if late entry) Clinician Name, License, Job Type Service Documentation Travel time: Encounterminutes Type: Select encounter typetime Type of Service: Medication
3. ASSESSMENT/DIAGNOSIS Initial/Update* Unchanged (see initial or last update) Axis I:
4. TREATMENT PLAN Lab Tests ordered and/or other evaluations recommended: See Next Page: Change(s) in Medication(s): Y N Specify ANY change(s) and reason Comments/Explanations:
Follow up visits: Y N
Next follow up date: Signature and Title:
ED 5.0 med mon 2pg. rev 9-28-10