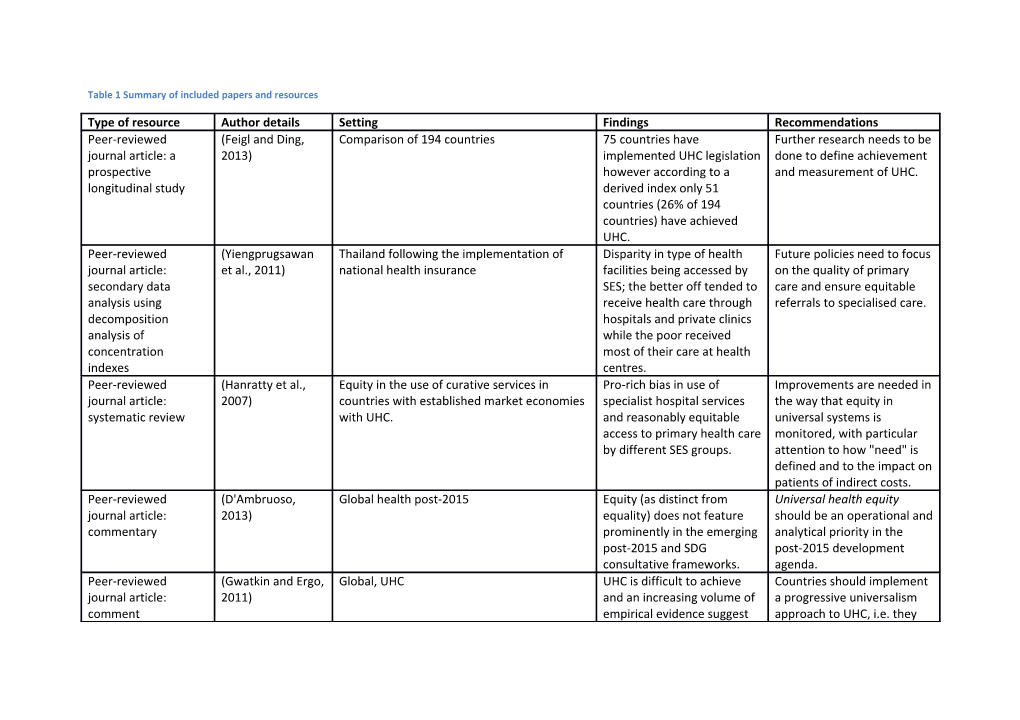
Table 1 Summary of included papers and resources
Type of resource Author details Setting Findings Recommendations Peer-reviewed (Feigl and Ding, Comparison of 194 countries 75 countries have Further research needs to be journal article: a 2013) implemented UHC legislation done to define achievement prospective however according to a and measurement of UHC. longitudinal study derived index only 51 countries (26% of 194 countries) have achieved UHC. Peer-reviewed (Yiengprugsawan Thailand following the implementation of Disparity in type of health Future policies need to focus journal article: et al., 2011) national health insurance facilities being accessed by on the quality of primary secondary data SES; the better off tended to care and ensure equitable analysis using receive health care through referrals to specialised care. decomposition hospitals and private clinics analysis of while the poor received concentration most of their care at health indexes centres. Peer-reviewed (Hanratty et al., Equity in the use of curative services in Pro-rich bias in use of Improvements are needed in journal article: 2007) countries with established market economies specialist hospital services the way that equity in systematic review with UHC. and reasonably equitable universal systems is access to primary health care monitored, with particular by different SES groups. attention to how "need" is defined and to the impact on patients of indirect costs. Peer-reviewed (D'Ambruoso, Global health post-2015 Equity (as distinct from Universal health equity journal article: 2013) equality) does not feature should be an operational and commentary prominently in the emerging analytical priority in the post-2015 and SDG post-2015 development consultative frameworks. agenda. Peer-reviewed (Gwatkin and Ergo, Global, UHC UHC is difficult to achieve Countries should implement journal article: 2011) and an increasing volume of a progressive universalism comment empirical evidence suggest approach to UHC, i.e. they that the ‘trickle-down effect’ should aim to first increase is pervasive and may coverage among constitute the norm. disadvantaged groups, rather than taking the traditional approach of serving initially those who are easiest to reach. Peer-reviewed (Knaul et al., 2012) Mexico Mexico has made significant Further reform including journal article: progress with social systematic measures to commentary protection of health based reorganise the health system on access to effective health by functions is needed to care being viewed as a continue progress towards universal right. Research UHC. shows that the program is improving access to health services, improving effective coverage and reducing catastrophic and impoverishing health expenditure particularly for the poor. Peer-reviewed (Jacobs et al., Low to middle income Asian countries Presents an analytical A combination of journal article: an 2011) framework for selecting interventions concurrently analytical framework appropriate interventions to addressing demand-side and address barriers supply-side barriers are (geographical access, required to tackle specific availability, affordability and access barriers but their acceptability) to health effectiveness can be services. The framework can influenced by contextual be used both to identify factors. interventions and to analyse why certain interventions fail to tackle specific barriers. Peer-reviewed (Kisely et al., 2007) Nova-scotia province of Canada Despite the UHC system, Further research into how journal article: psychiatric status affects disparities arise and how to secondary analysis of survival with and access to reduce them is a key priority cohort records some procedures for for future research. circulatory disease. Despite increased risk of death, psychiatric patients, and in particular, inpatients were less likely to undergo specialised or revascularization procedures. Peer-reviewed (Blais et al., 2003) Canada – Quebec province While no significant regional More evidence-based journal article: differences were found for planning is required, primary and need indicators, mental specifically using secondary analysis health services for children epidemiologic survey data, are not distributed across to match resources to needs regions according to need. and to monitor changes over time. Peer-reviewed (Cunningham et Canada: British Columbia Province Inequities were observed in Identifying potential journal article: cross- al., 2011) end-of-life health care with systemic reasons for the sectional analysis of populations with higher observed patterns of secondary data income receiving more care inequity is important in and need-adjusted equity designing policies to address results suggesting that males such patterns. received less care than females. Peer-reviewed (Korda et al., 2009) Australia – 12,940 patients hospitalised for Using the SEIFA index of Further research is needed journal article: acute myocardial infarction or angina in the socioeconomic to determine whether the retrospective cohort state of Western Australia. disadvantage, the results higher rates of procedures analysis of secondary showed Australia’s health for discretionary care are data care system does not due to overuse in guarantee equity in the advantaged individuals or receipt of high technology underuse in disadvantaged health care for patients with groups – with different IHD. There was more equity implications for policy. in the receipt of procedures for AMI, where the guidelines for treatment are well established, but less equity for angina patients, with more advantaged populations receiving more procedures for angina, perhaps because health care is less urgent and more discretionary. Peer-reviewed (Kreng and Yang, Taiwan under the national health insurance There was found to be Under the NHI scheme journal article: cross- 2011) system and the 23 decision making units. horizontal inequity of payments for health care sectional study using resource allocation between suppliers could be adopted a multi-criteria geographic areas with the as an efficient strategy to decision making North receiving more reduce the disparity of approach with grey resources with limited access resource allocation and incidence analysis to health care services in ensure more equitable rural areas. distribution. Further emphasis should be put on vertical equity taking into account demographics (i.e. the elderly need more care) as well as the social environment (i.e. issues with transport in rural areas). Peer-reviewed (Shortt and Shaw, Review of 39,000 surgeries performed A review was conducted of Further research needs to be journal article: 2003) between 1992 and 1999 at two Canadian the waiting times for elective done to include the secondary analysis of hospitals. surgery by SES however no population who did not medical records relationship was receive elective surgery and determined. to adjust for severity of illness. Organisational report: (Giedion et al., The developing world UHC interventions in LMICs 1. Affordability is important The World Bank 2013) improve access to health but may not be enough. systematic review care. The evidence also 2. Target the poor, but keep and synthesis of shows, though less an eye on the non-poor. existing evidence convincingly, that UHC often 3. Benefits should be closely has a positive effect on linked to target populations’ financial protection, and needs. that, in some cases it seems 4. Highly focused to have a positive impact on interventions can be a useful health status. initial step toward UHC. 5. Incorporate evaluation in the early stages of the program and, ideally, simultaneously design the intervention and evaluation. Organizational report: (World Health Global, UHC Proposes that countries Further research is needed WHO World Health Organization, measure UHC across a into how quality and equity report 2013 2013) spectrum which of access are monitored encompasses the social within UHC programmes. determinants of health across a subset of services that represent overall quantity, quality, equity and financing of services, disaggregated by locally- appropriate dimensions. Background paper for (Frenz and Vega, Literature review and recommendations Equity of utilisation is being Equitable access should be Global Symposium on 2010) commonly used as a proxy viewed as the experiences Health Systems indicator for equity of access and interactions of different Research but fails to adequately groups with the health capture unmet need of those system, within the broader who do not use the formal social determinants of health sector. Presents an health. analytical framework for assessing equity of access within UHC policies. Organisational (USAID, 2012) Country-level There are lingering There is a need for a meeting report conceptual challenges with conceptual framework to measuring UHC and varying measure UHC utilising equity objectives and audiences for catalysing indicators which indicators: global advocacy encompass financial risk purposes require a small protection and coverage of number of simple, intuitive, good quality health services easy-to-communicate for all. A meeting of country- indicators whilst country- level stakeholders should be level health planners and convened to facilitate policymakers, need more common understanding and comprehensive, detailed, identify country-level needs and actionable country- for indicators. Concurrently, specific indicators for policy key stakeholders should and management. come to consensus on criteria for selecting high- level indicators. Organization report: (UHC Forward, Global monitoring of health intervention Presents a draft framework The progress of the most Rockefeller 2012) coverage, with a focus on equity within UHC and criteria for the disadvantaged/least Foundation development of an index and performing groups should tracer indicators for global receive as much, if not more monitoring of UHC with attention than the whole regular measurement of population. equity. Organization report: (World Health Global and country-level UHC Discusses appropriate Countries must select their WHO technical Organization et al., indicators for equity analyses own indicators and global meeting report 2013) at global and country levels. stakeholders should determine internationally comparable, tracer indicators for UHC. Organization report: (World Health Global and country-level UHC Presents a framework and Feedback is sought on the County and Global Organization and timelines for monitoring of draft framework and its monitoring World Bank, 2013) UHC covering a set of potential as an umbrella goal frameworks for UHC interventions related to the for the SDGs. MDGs, as well as related to chronic conditions and injuries, as well as financial risk protection. Organisational report: (Sengupta, 2013) Global Secure finances for health The only to build truly Occasional Paper care are a necessary but universal health outcomes is insufficient condition for for finances to be equitable and high quality administered by well- care. Equity and efficiency designed public health care tend to be compromised by systems rather than the ideological pressures which private sell-out of health prevent an entirely public systems via UHC. system of care provision. Organisational report: (Brearley et al., Global The report estimates the 1.) The level and structured review of 2013) number of maternal and progressivity of funding for country experiences child health lives that would the health sector must and literature, key be saved if within-country increase. informant interviews, health inequities in the 2.) Health sector resources econometric coverage of essential MCH must be pooled across the analyses, a Lives interventions were population Saved Tool analysis eliminated. 3.) The package of benefits and case studies. should be tailored to meet the needs of poor and vulnerable people, including a minimum of free primary healthcare, and aligning the incentives of healthcare providers through payment mechanisms, will help to ensure more equitable coverage. 4.) Quality concerns in service delivery must be addressed. 5.) Coordinated reforms across the whole system, and beyond the health sector, are needed to address other barriers to demand and supply. 6.) The quantity, quality and use of disaggregated data is critical to inform planning process, monitoring, evaluation and accountability. 7.) Effective government stewardship is essential for regulation, strategic planning and effective collaboration with other actors.
1. BLAIS, R., BRETON, J. J., FOURNIER, M., ST-GEORGES, M. & BERTHIAUME, C. 2003. Are mental health services for children distributed according to needs? Can J Psychiatry, 48, 176-86. 2. BREARLEY, L., MARTEN, R. & O'CONNELL, T. 2013. Universal Health Coverage: A Commitment to Close the Gap. 3. CUNNINGHAM, C. M., HANLEY, G. E. & MORGAN, S. G. 2011. Income inequities in end-of-life health care spending in British Columbia, Canada: A cross-sectional analysis, 2004-2006. Int J Equity Health, 10, 12. 4. D'AMBRUOSO, L. 2013. Global health post-2015: the case for universal health equity. Glob Health Action, 6, 19661. 5. FEIGL, A. B. & DING, E. L. 2013. Evidenced Formal Coverage Index and universal healthcare enactment: A prospective longitudinal study of economic, social, and political predictors of 194 countries. Health Policy, 113, 50-60. 6. FRENZ, P. & VEGA, J. 2010. Universal health coverage with equity: what we know, don't know and need to know. Background paper for the global symposium on health systems research, 16-19 November 2010 - Montreux, Switzerland. HSR Symposium. 7. GIEDION, U., ALFONSO, E. & DIAZ Y 2013. The impact of universal coverage schemes in the developing world: a review of the existing evidence. Washington DC,: The World Bank. 8. GWATKIN, D. R. & ERGO, A. 2011. Universal health coverage: friend or foe of health equity? The Lancet, 377, 2160-2161. 9. HANRATTY, B., ZHANG, T. & WHITEHEAD, M. 2007. How close have universal health systems come to achieving equity in use of curative services? A systematic review. International Journal of Health Services, 37, 89–109. 10. JACOBS, B., IR, P., BIGDELI, M., ANNEAR, P. L. & VAN DAMME, W. 2011. Addressing access barriers to health services: an analytical framework for selecting appropriate interventions in low-income Asian countries. Health Policy and Planning, 2011, 1-13. 11. KISELY, S., SMITH, M., LAWRENCE, D., COX, M., CAMPBELL, L. A. & MAATEN, S. 2007. Inequitable access for mentally ill patients to some medically necessary procedures. CMAJ, 176, 779-84. 12. KNAUL, F. M., GONZÁLEZ-PIER, E., GÓMEZ-DANTÉS, O., GARCÍA-JUNCO, D., ARREOLA-ORNELAS, H., BARRAZA-LLORÉNS, M., SANDOVAL, R., CABALLERO, F., HERNÁNDEZ-AVILA, M., JUAN, M., KERSHENOBICH, D., NIGENDA, G., RUELAS, E., SEPÚLVEDA, J., TAPIA, R., SOBERÓN, G., CHERTORIVSKI, S. & FRENK, J. 2012. The quest for universal health coverage: achieving social protection for all in Mexico. The Lancet, 380, 1259-79. 13. KORDA, R. J., CLEMENTS, M. S. & KELMAN, C. W. 2009. Universal health care no guarantee of equity: comparison of socioeconomic inequalities in the receipt of coronary procedures in patients with acute myocardial infarction and angina. BMC Public Health, 9, 460. 14. KRENG, V. B. & YANG, C. T. 2011. The equality of resource allocation in health care under the National Health Insurance System in Taiwan. Health Policy, 100, 203-10. 15. SENGUPTA, A. 2013. Universal Health Coverage: Beyond rhetoric. In: MCDONALD, D. A. & RUITERS, G. (eds.) Municipal Services Project, Occasional Paper No. 20 - November 2013. 16. SHORTT, S. E. & SHAW, R. A. 2003. Equity in Canadian health care: does socioeconomic status affect waiting times for elective surgery? CMAJ, 168, 413-6. 17. UHC FORWARD 2012. Measurement of trends and equity in coverage of health interventions in the context of universal health coverage. Rockefeller Foundation Center, Bellagio, September 17-21, 2012. 18. USAID 2012. Measuring and monitoring country progress towards universal health coverage: concepts, indicators, and experiences. Meeting summary - July 20, 2012, Washington, DC. Washington DC: United States Agency for International Development, Health Systems 20/20. 19. WORLD HEALTH ORGANIZATION 2013. The World Health Report 2013: research for universal health coverage. Geneva: WHO. 20. WORLD HEALTH ORGANIZATION & WORLD BANK 2013. Monitoring Progress towards Universal Health Coverage at Country and Global Levels: A Framework. Joint WHO/World Bank Group Discussion Paper, December 2013 21. WORLD HEALTH ORGANIZATION, WORLD BANK & MINISTRY OF HEALTH SINGAPORE 2013. Measurement and monitoring of universal health coverage. Techinical meeting; Singapore, 17-18 September 2013 summary report. 22. YIENGPRUGSAWAN, V., CARMICHAEL, G., LIM, L.-Y., SEUBSMAN, S. & SLEIGH, A. 2011. Explanation of inequity in utilization of ambulatory care before and after universal health insurance in Thailand. Health Policy and Planning,, 26, 105-114.