Radiology Case Report: Katharine Moore - 4339665
Patient ID: OH# 09296674 Date of Study: June 11, 2008 Type of Study: Chest Xray (AP Portable Erect)
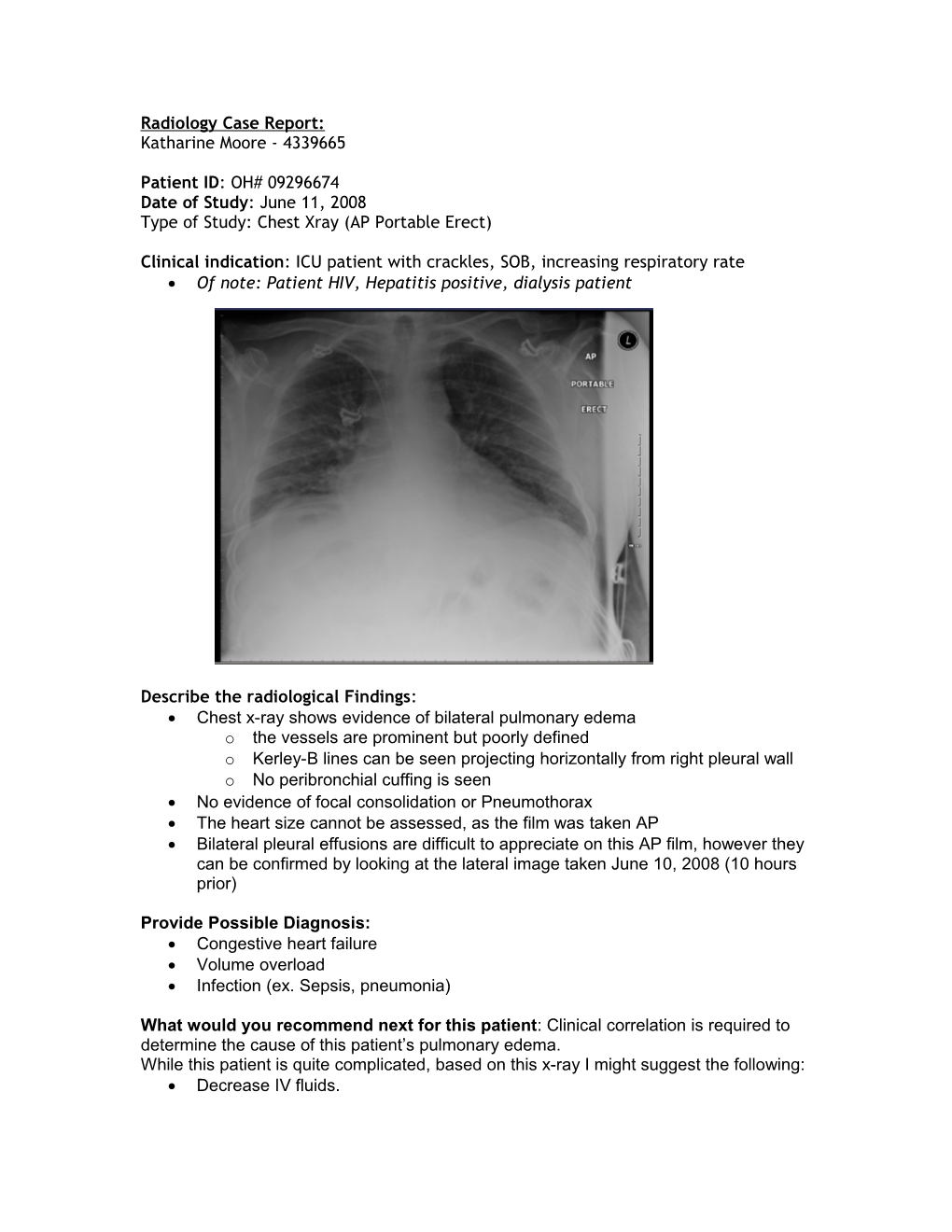
Clinical indication: ICU patient with crackles, SOB, increasing respiratory rate Of note: Patient HIV, Hepatitis positive, dialysis patient
Describe the radiological Findings: Chest x-ray shows evidence of bilateral pulmonary edema o the vessels are prominent but poorly defined o Kerley-B lines can be seen projecting horizontally from right pleural wall o No peribronchial cuffing is seen No evidence of focal consolidation or Pneumothorax The heart size cannot be assessed, as the film was taken AP Bilateral pleural effusions are difficult to appreciate on this AP film, however they can be confirmed by looking at the lateral image taken June 10, 2008 (10 hours prior)
Provide Possible Diagnosis: Congestive heart failure Volume overload Infection (ex. Sepsis, pneumonia)
What would you recommend next for this patient: Clinical correlation is required to determine the cause of this patient’s pulmonary edema. While this patient is quite complicated, based on this x-ray I might suggest the following: Decrease IV fluids. Evaluate for signs of infection, though consolidation/pneumonia is not seen on this AP film it is possible that the patient’s HIV status has prevented him from mounting the immune response required to generate focal patches of consolidation. Diuretics will not be helpful given the patient is dependent on dialysis… consider dialysis to remove extra fluid if volume overload is suspected. No other imaging is required. May repeat chest x-ray if clinical status changes, or in 1-2d to ensure resolution.
Is the use of this test appropriate: Yes
Is there any alternative test(s): No. While the above changes could be identified via CT scan, the CXR was a much more cost-effective choice for this patient. Also, the clinical information provided suggested that the patient was experiencing increased distress, thus a portable AP film at the bedside was the only practical choice.
How would you explain to the patient about the possible risks & benefits of this test?
Benefits Imaging the lungs allows us to find/confirm possible reasons for your recent SOB (pneumonia, pulmonary edema, pulmonary nodules, lung ca etc.) Comparing these films to previous ones allows us to assess whether things have improved, worsened or changed Catching lung pathology early gives us the best chance for successful intervention
Risks: Risks are minor compared to benefits Low dose of radiation (compared to other forms of imaging) o Dose equivalent to what someone would receive in background radiation every 10 days (~ 0.1mSV) May be inconclusive, and require further imaging
How much does the test cost: A single chest x-ray costs approximately $30-40.