2.5 BLOOD and BODY FLUID EXPOSURE Completed in liaison with Brigid Quaid, Occupational Health Nurse Manager
SHARPS INJURY A PERCUTANEOUS injury is one where there has been skin penetration by a sharp, which has been used on a patient or has been in contact with a patient’s body fluids.
Other EXPOSURES include bites, blood and body fluid exposure and splashes on to the skin or mucous membranes
PROCEDURE AFTER SHARPS INJURY
BLEED IT Þ WASH IT Þ REPORT IT
1. Encourage the area to bleed freely by washing under running water 2. Do not suck the puncture site 3. Wash the site thoroughly under running water 4. Report the incident to the ward/unit/department Manager and Supervisor, if applicable 5. Exposure Report Form to be completed, 6. Attend the Accident and Emergency Department with the completed form
Procedure for BLOOD or BODY FLUID EXPOSURE
1. Wash the site well under running water. 2. Complete Near Miss Incident Report Form 3. Contact the Occupational Health Department or Accident and Emergency Department for advice
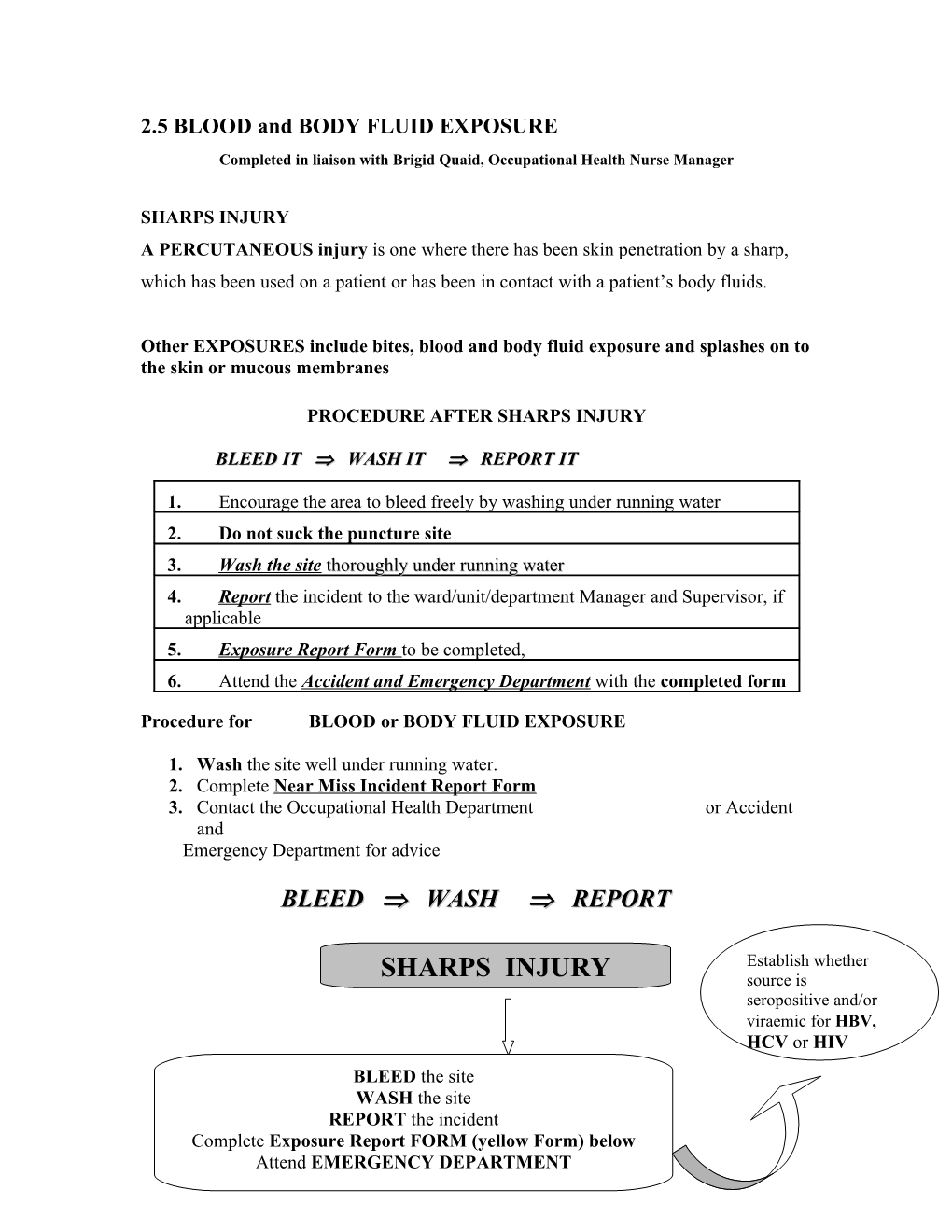
BLEED Þ WASH Þ REPORT
Establish whether SHARPS INJURY source is seropositive and/or viraemic for HBV, HCV or HIV BLEED the site WASH the site REPORT the incident Complete Exposure Report FORM (yellow Form) below Attend EMERGENCY DEPARTMENT SOURCE of sharp If known ward/department manager will contact the patients medical team to arrange for consented blood testing of source HEPATITIS immunity status Consent should be documented in If not fully immune or immunity the patients notes and consent unknown/uncertain, the staff obtained for Hepatitis B & C and member may require; HIV testing Hepatitis B immunoglobulin, administered intravenously, by the A&E department
TETANUS immunity status If not immune/uncertain, tetanus toxoid may be administered
Occupational Health Department will follow up and arrange for counselling as required
BLOOD/BODY FLUID EXPOSURE REPORT FORM WHEN COMPLETED PLEASE RETURN TO:
Occupational Health Department Telephone ext: 22019
Part 1 To be completed at location/ward where the incident occurred. A. PERSON EXPOSED B. SOURCE PATIENT DETAILS
To be completed in full by ward sister or This must be completed in full by appropriate medical personnel department head/supervisor as appropriate Source: Known Unknown Name: ______Medical Record Number: ______Address: ______Hospital: ______Ward/Department: ______Name: ______Date of Birth: ______Home Telephone No: ______ WITH INFORMED CONSENT (please note Date of Birth: ______in source patient chart) blood test to be requested from patient for hepatitis B surface Occupation: ______antigen & hepatitis C antibody & HIV antibody. Department: ______(Send the sample to the microbiology laboratory for urgent testing) Date & Time of exposure: ______ Does the medical history suggest that the Date & Time incident reported: ______source patient may be in a HIV risk group? YES/NO Description of incident: ______Signed: ______Date: ______
PERSON EXPOSED:
Treat the injury, give tetanus toxoid if necessary. Has a hepatitis B Vaccine course been completed? YES/NO Date of last dose: If YES: blood sample to be sent to Microbiology Department for hepatitis B surface antibody titre (urgent) and storage Result: Hep B surface antibody titre: ______ If NO: blood sample to be sent to Microbiology Department for storage Ring the laboratory for the result of the blood test on the source patient (if known) Result: HepBsAg Hep C HIV Is the injury significant? YES/NO Is hepatitis B hyperimmuneglobulin needed? YES/NO Is HIV prophylaxis required? YES/NO (If YES contact the Medical Registrar) Is hepatitis B vaccine needed? YES/NO If needed vaccine will be given in the Occupational Health Dept. ext: 22019 (Non urgent)
Signed: ______Date: ______
PLEASE RETURN THIS FORM TO THE OCCUPATIONAL HEALTH DEPARTMENT Page1 Part 3 To be completed by the Occupational Health Department
SOURCE PATIENT Blood test for Hepatitis B Antigen: Result: Date: Blood test for Hepatitis C Antibody Result: Date: Blood test for HIV: Result: Date:
PERSON EXPOSED Has a blood sample been sent to the laboratory for storing? Yes
Hepatitis B vaccination: Present Status: Details of interview, counselling and follow up of exposed person: Hepatitis B Status Hepatitis C Status HIV Status
PLEASE NOTE ù Sharps must not be passed directly from hand to hand and handling should be kept to a minimum
ù Needles must not be bent or broken prior to use or disposal
ù Needles and syringes must not be disassembled by hand prior to disposal
ù Needles should never be recapped
ù Used sharps must be discarded into an approved sharps box/container (Epic 2001)
For further advice see SHB document Prevention and Protection Protocols for Blood and Body Fluid Exposures – A Focus on Sharps January 2003
Pratt R.J., Pellowe C., Loveday H.P., Robinson N and Smith G.W.(2001) The Epic Project : Developing National Evidence-based Guidelines for Preventing Healthcare Associated Infections. Journal of Hospital Infection : January, Vol.47, Supplement, 1-82