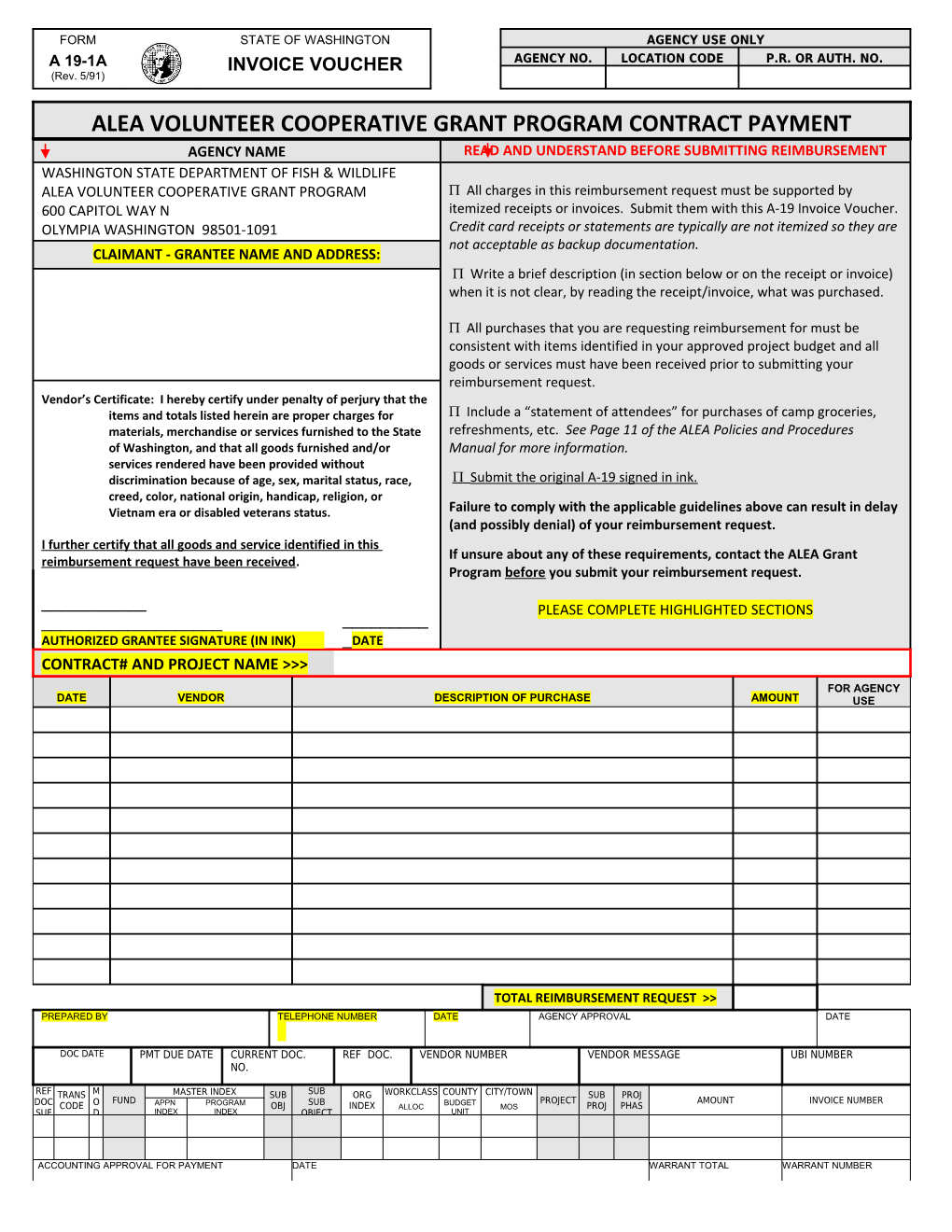
FORM STATE OF WASHINGTON AGENCY USE ONLY A 19-1A INVOICE VOUCHER AGENCY NO. LOCATION CODE P.R. OR AUTH. NO. (Rev. 5/91)
ALEA VOLUNTEER COOPERATIVE GRANT PROGRAM CONTRACT PAYMENT AGENCY NAME READ AND UNDERSTAND BEFORE SUBMITTING REIMBURSEMENT WASHINGTON STATE DEPARTMENT OF FISH & WILDLIFE ALEA VOLUNTEER COOPERATIVE GRANT PROGRAM All charges in this reimbursement request must be supported by 600 CAPITOL WAY N itemized receipts or invoices. Submit them with this A-19 Invoice Voucher. OLYMPIA WASHINGTON 98501-1091 Credit card receipts or statements are typically are not itemized so they are not acceptable as backup documentation. CLAIMANT - GRANTEE NAME AND ADDRESS: Write a brief description (in section below or on the receipt or invoice) when it is not clear, by reading the receipt/invoice, what was purchased.
All purchases that you are requesting reimbursement for must be consistent with items identified in your approved project budget and all goods or services must have been received prior to submitting your reimbursement request. Vendor’s Certificate: I hereby certify under penalty of perjury that the items and totals listed herein are proper charges for Include a “statement of attendees” for purchases of camp groceries, materials, merchandise or services furnished to the State refreshments, etc. See Page 11 of the ALEA Policies and Procedures of Washington, and that all goods furnished and/or Manual for more information. services rendered have been provided without discrimination because of age, sex, marital status, race, Submit the original A-19 signed in ink. creed, color, national origin, handicap, religion, or Vietnam era or disabled veterans status. Failure to comply with the applicable guidelines above can result in delay (and possibly denial) of your reimbursement request. I further certify that all goods and service identified in this If unsure about any of these requirements, contact the ALEA Grant reimbursement request have been received. Program before you submit your reimbursement request.
______PLEASE COMPLETE HIGHLIGHTED SECTIONS ______AUTHORIZED GRANTEE SIGNATURE (IN INK) _DATE CONTRACT# AND PROJECT NAME >>> FOR AGENCY DATE VENDOR DESCRIPTION OF PURCHASE AMOUNT USE
TOTAL REIMBURSEMENT REQUEST >> PREPARED BY TELEPHONE NUMBER DATE AGENCY APPROVAL DATE
DOC DATE PMT DUE DATE CURRENT DOC. REF DOC. VENDOR NUMBER VENDOR MESSAGE UBI NUMBER NO.
REF TRANS M MASTER INDEX SUB SUB ORG WORKCLASS COUNTY CITY/TOWN SUB PROJ FUND APPN PROGRAM BUDGET PROJECT AMOUNT INVOICE NUMBER DOC CODE O OBJ SUB INDEX ALLOC MOS PROJ PHAS SUF D INDEX INDEX OBJECT UNIT
ACCOUNTING APPROVAL FOR PAYMENT DATE WARRANT TOTAL WARRANT NUMBER