Practical No : 02
Hb, ESR, PCV ASSESSMENT AND OSMOTIC FRAGILITY TEST
Haemoglobin (Hb) Measurement
Objectives :- The student should be able to, 1. Define normal Hb levels 2. List the conditions that a. Decrease Hb levels b. Increase Hb levels 3. Identify the instruments that are used to measure Hb levels 4. Describe the steps involved in performing the test 5. Read and interpret the results 6. Describe the advantages and disadvantages of the test
Can be done using the Sahli's method or the Talliquest method, which both employ the method of estimating haemoglobin by measurement of its colour. The Talliquest method is not used routinely as errors may occur.
Sahli's Method
Principle : The blood is diluted in an acid solution, converting Hb to acid haematin. The test solution is matched against a coloured glass reference.
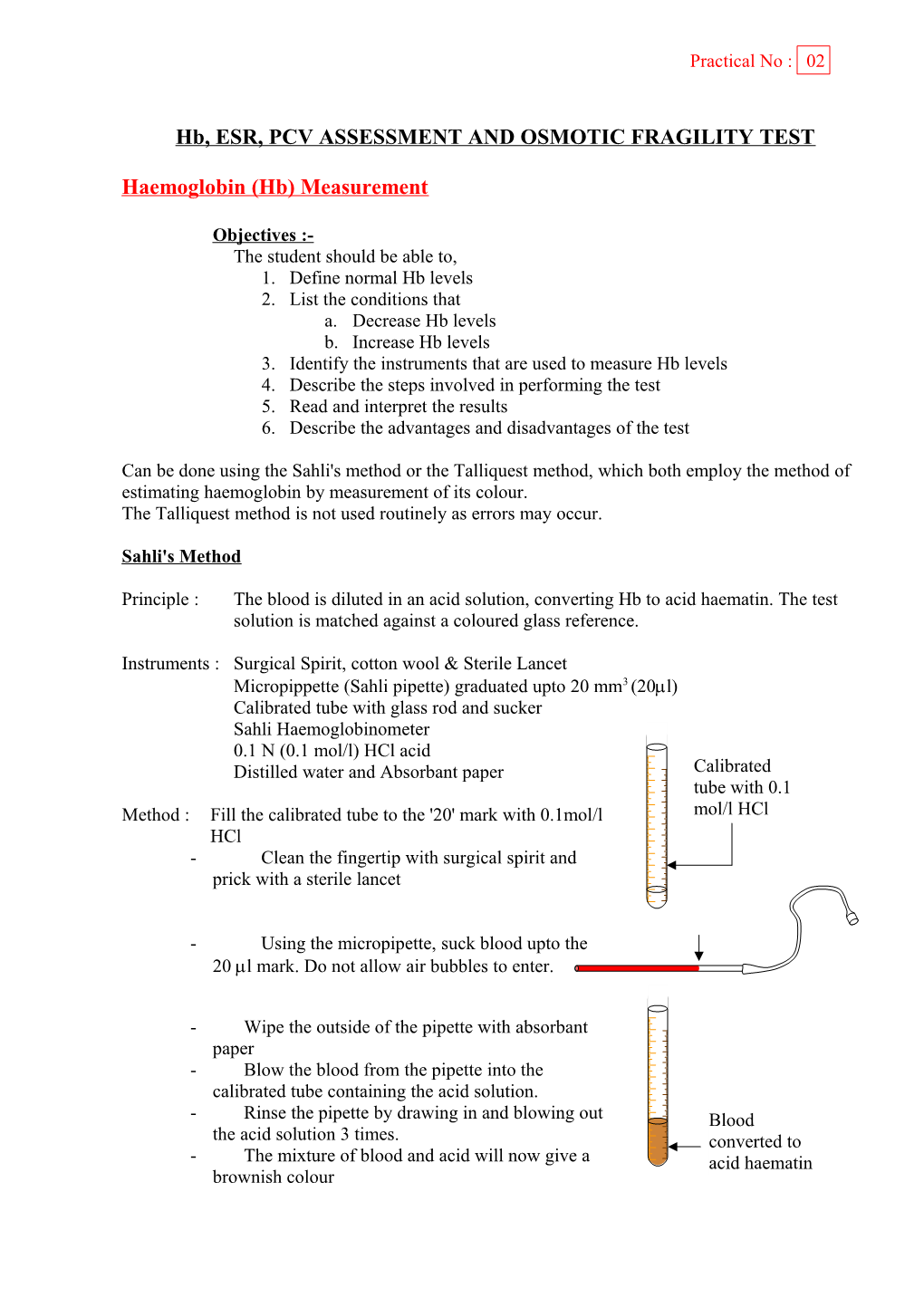
Instruments : Surgical Spirit, cotton wool & Sterile Lancet Micropippette (Sahli pipette) graduated upto 20 mm3 (20l) Calibrated tube with glass rod and sucker Sahli Haemoglobinometer 0.1 N (0.1 mol/l) HCl acid Distilled water and Absorbant paper Calibrated tube with 0.1 Method : Fill the calibrated tube to the '20' mark with 0.1mol/l mol/l HCl HCl - Clean the fingertip with surgical spirit and prick with a sterile lancet
- Using the micropipette, suck blood upto the 20 l mark. Do not allow air bubbles to enter.
- Wipe the outside of the pipette with absorbant paper - Blow the blood from the pipette into the calibrated tube containing the acid solution. - Rinse the pipette by drawing in and blowing out Blood the acid solution 3 times. converted to - The mixture of blood and acid will now give a acid haematin brownish colour - Allow to stand for five minutes - Now place the calibrated tube in the comparator and stand facing a window
- Compare the colour of the calibrated tube with the reference tubes If lighter, the Hb value is 4g/l or less If darker, continue to dilute the blood acid mixture with distilled water drop by drop, all the while stirring with the glass rod.
- Stop when the colours match - Now, note the mark that is reached.
Results : Depending on the type of tube, the result can be read as g/dl or g%
Interpretation : The normal Haemoglobin values for males and females are as follows, Male - 14 - 15 g/dl Female - 13 - 14 g/dl
A value less than the above will indicate Anaemia and a value much higher than the above will indicate polycythaemia.
Further tests have to be performed, however, to identify the nature / cause of the anaemia.
Advantages and Disadvantages :
Advantages Disadvantages A very simple method Colour comparison may vary from Easy to perform, with minimum technical observer to observer. expertise Obstruction of micropipette by air Can transport apparatus easily bubbles Addition of extra distilled water to tube Due to tight sucking, ECF may enter the micropipette Incomplete transformation of haem to acid haematin Packed Cell Volume (PCV) - (Haematocrit / Erythrocyte volume fraction)
Objectives :- The student should be able to, 1. Describe what is Packed Cell Volume (PCV) 2. Define normal levels 3. List the conditions that a. Increase the PCV and b. Decrease the PCV 4. Identify the instruments used to measure PCV 5. Describe the steps involved in performing the procedures 6. Read and Interpret the results
Packed cell volume estimation can be done by two methods 1. Wintrobe method (Macro) 2. Microhaematocrit method (Micro)
Wintrobe Method
Instruments : Ordinary electric centrifuge Special graduated tubes (Wintrobe tube) (Bore - 0.6 mm / Length - 9.5 cm / Calibrations - 0 - 100) Long fine capillary Pasteur pipette with rubber teat Sterile syringe and needle, cotton wool and surgical spirit Anticoagulant (EDTA)
Method : Draw venous blood, add it to a tube of anticoagulant (EDTA) and mix well - Using the capillary pipette, fill the wintrobe tube with blood upto the '100' mark. - Make sure that there are no air bubbles. - Centrifuge for 30 minutes at 3600 rpm - Read the level at which the red cells meet the level of leukocytes
Result : The graduation should be read from down upwards (towards the 100 mark)
Microhaematocrit method
Instruments : Microhaematocrit centrifuge (special, high speed) Capillary tubes containing a dried deposit of Heparin (anticoagulant) (length - 75 mm / bore - 1.5 mm) Plastic modeling clay Sterile blood lancet, surgical spirit and cotton wool. Method : Clean fingertip with surgical spirit and prick with a sterile lancet. - Wipe away the first drop with filter paper - Apply the tip of the heparinized capillary tube to the drop of blood. - The blood will flow into the tube by capillary action
- Fill about 3/4ths of the tube. - Plug the other end of the tube with plastic modeling clay
- Place the capillary tubes in the centrifuge slots. (the sealed end of the tube should point outwards) - Centrifuge at 15000 rpm for 3 minutes.
- The blood will have separated into layers. (Plasma / white cell coat / red cell layer)
Results : The reading is made at the junction between red cells and white cells using the haematocrit meter (reader).
100
50
0
Interpretation : The normal values for PCV are, Males - 40 - 54 Females - 37 - 47
PCV is increased in - Polycythaemia Spherocytosis Severe dehydration
PCV is decreased in - Anaemia Erythrocyte Sedimentation Rate (ESR)
Objectives :- The student should be able to, 1. Describe what is Erythrocyte Sedimentation Rate (ESR) 2. Describe the physiological basis of ESR 3. Define normal ranges 4. List the conditions that a. Increase the ESR b. Decrease the ESR 5. Identify the instruments that are used to measure ESR 6. Read and interpret the results.
Erythrocyte Sedimentation Rate (ESR) measures the rate at which red blood cells in anticoagulated blood settles to the bottom of a calibrated tube.
Instruments : Westegren ESR tube (internal diameter - 2.5 mm / graduated from 0 -200 mm) Westegren stand Anticoagulant : 38g/l (3.8%) trisodium citrate solution 5 ml graduated syringe Timer Small tube or bottle
Method : - Place 0.4 ml of 3.8% tri sodium citrate in a small tube or bottle
Tri Sodium - Collect venous blood applying the Citrate tourniquet as loosely as possible - Collect 2 ml of blood. - Remove the needle from the syringe and add 1.6 ml blood to the bottle containing anticoagulant Anticoagulated - Mix well by shaking the bottle gently. blood
- Measurement of ESR should begin within 2 hours of collecting blood !
- Draw the citrated blood into the westegren tube using a rubber bulb upto the '0' mark 3-way pipette filler
Westegren tube - Place the tube in the Westegren stand making sure that the tube is completely upright. - Check that there are no air bubbles in the tube - Check that the stand is level and is away from the windows
- Start the timer after setting it to one hour. ESR
1 hr Results : Are read one hour later Note the height of the column of plasma in mm graduations starting from the '0' mark at the top
The results are expressed as ESR - ………….mm/ 1st hour
Interpretation : The normal values for ESR are, Males - 1 - 10 mm/ 1st hour Females - 3 - 14 mm/ 1st hour
ESR depends on The ratio of specific gravity of RBC : Plasma
F F g
Rouleaux formation
ESR is also known as a test of the Acute Phase Response. Here, a deviation from the normal values will be seen when there are increased amounts of acute phase proteins (Caeruloplasmin, Haptoglobin) in the blood.
ESR increased in, ESR decreased in Chronic inflammations & infections Polycythaemia Eg. TB Sickle cell disease Acute inflammations & infections Cryoglobinaemia Normal Pregnancy (Physiological) Malignancies Severe anaemias
Q: Why do females have a slightly higher ESR than males ? Osmotic Fragility Test
Objectives :- The student should be able to, 1. Describe what is 'Osmotic Fragility Test' 2. Define the normal osmotic fragility range 3. Describe how to perform the test 4. Describe the conditions that a. Increase osmotic fragility b. Decrease osmotic fragility 5. Read and interpret the results
This measures the fragility of red blood cells when put into solutions of hypotonic saline of varied tonicity.
Principle : When red cells are placed in buffered saline solutions of varying tonicity, there is a variation in the net amount of fluid entering or leaving the cells.
In an Isotonic solution In a Hypotonic solution In a Hypertonic solution (0.9% saline)
Net fluid shift out of No net fluid shift Net fluid shift into the red cell the red cell
No change in the RBC volume The red cell swells The red cell shrinks Thus, at very low tonicity, the red cell will absorb water to such an extent that it will lyse (haemolysis). The osmotic fragility of freshly taken red cells reflects their ability to take up a certain amount of water before lysing. This is determined by their volume to surface area ratio.
Instruments / materials : Test tube stand 10 conical test tubes NaCl solutions of varied concentration ranging from 0.9% saline to 0.1% Sample of anticoagulated venous blood (using heparin as EDTA contains osmotically active particles) Pipette filler
Method : Obtain a sample of venous blood and mix it with anticoagulant. - Take 10 conical test tubes and place in the stand - Put 5ml each of the solutions of varied tonicity into these tubes and label them - Using a pipette filler put 1 drop of blood each into the tubes. - Mix the blood and saline in each tube - Allow the tubes to stand for one hour or centrifuge them - Now, observe for changes.
Results : The following changes will be seen in the test tubes
Clear solution Slight reddish Reddish solution with red button solution with red no red button button
0.90 0.75 0.65 0.60 0.55 0.50 0.40 0.35 0.30 0.20 % solutions - Observe the concentration of the saline where red colour first appears in the solution - Observe the concentration of the saline where the red button completely disappears from the bottom of the tube. - This will be the normal osmotic fragility range. - Plot these results on a graph.
Interpretation:
The graph shows the normal range 100 of osmotic fragility. ( ) 80 This ranges from 0.45 - 0.55 with initial lysis at 0.55 and completion of 60 lysis at 0.45 40 Osmotic fragility is
Increased in, (curve shifted to right) 20 Hereditary Spherocytosis Autoimmune Haemolytic anaemia 0 0.2 0.3 0.35 0.4 0.45 0.5 0.55 0.6 0.65 0.75 0.9 Decreased in, (curve shifted to left) Iron deficiency anaemia - Thalassaemia minor Sickle cell anaemia
Q. : Explain why the osmotic fragilty differs from the normal range in the above conditions.