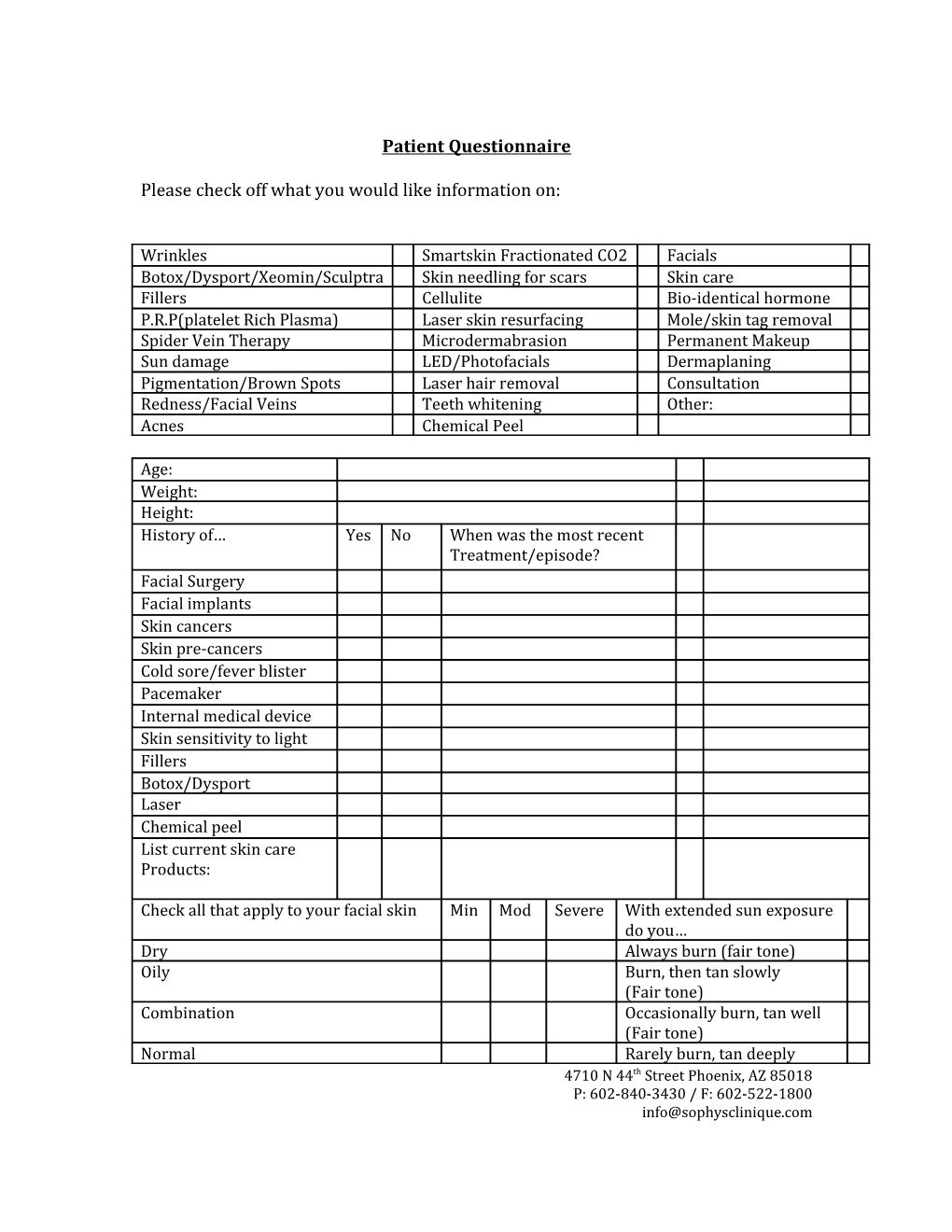
Patient Questionnaire
Please check off what you would like information on:
Wrinkles Smartskin Fractionated CO2 Facials Botox/Dysport/Xeomin/Sculptra Skin needling for scars Skin care Fillers Cellulite Bio-identical hormone P.R.P(platelet Rich Plasma) Laser skin resurfacing Mole/skin tag removal Spider Vein Therapy Microdermabrasion Permanent Makeup Sun damage LED/Photofacials Dermaplaning Pigmentation/Brown Spots Laser hair removal Consultation Redness/Facial Veins Teeth whitening Other: Acnes Chemical Peel
Age: Weight: Height: History of… Yes No When was the most recent Treatment/episode? Facial Surgery Facial implants Skin cancers Skin pre-cancers Cold sore/fever blister Pacemaker Internal medical device Skin sensitivity to light Fillers Botox/Dysport Laser Chemical peel List current skin care Products:
Check all that apply to your facial skin Min Mod Severe With extended sun exposure do you… Dry Always burn (fair tone) Oily Burn, then tan slowly (Fair tone) Combination Occasionally burn, tan well (Fair tone) Normal Rarely burn, tan deeply 4710 N 44th Street Phoenix, AZ 85018 P: 602-840-3430 / F: 602-522-1800 [email protected] (Olive tone) Break Outs Never burn (dark tone) Blackheads/clogged pores Never burn (very dark tone) Rosacea, redness or broken capillaries Sensitivity to products
(Print) Name:______Date______
4710 N 44th Street Phoenix, AZ 85018 P: 602-840-3430 / F: 602-522-1800 [email protected]