Parent/Guardian Date: School Principal Dental Checkup Result
The school dentist carried out a dental check up and the condition of your child's teeth is as indicated below.
Once examination has been given, please give the "Dental Exam Result Form" (bottom of this page) to your child's classroom teacher. It may be needed for reference at a later date.
Grade: Class: Name:
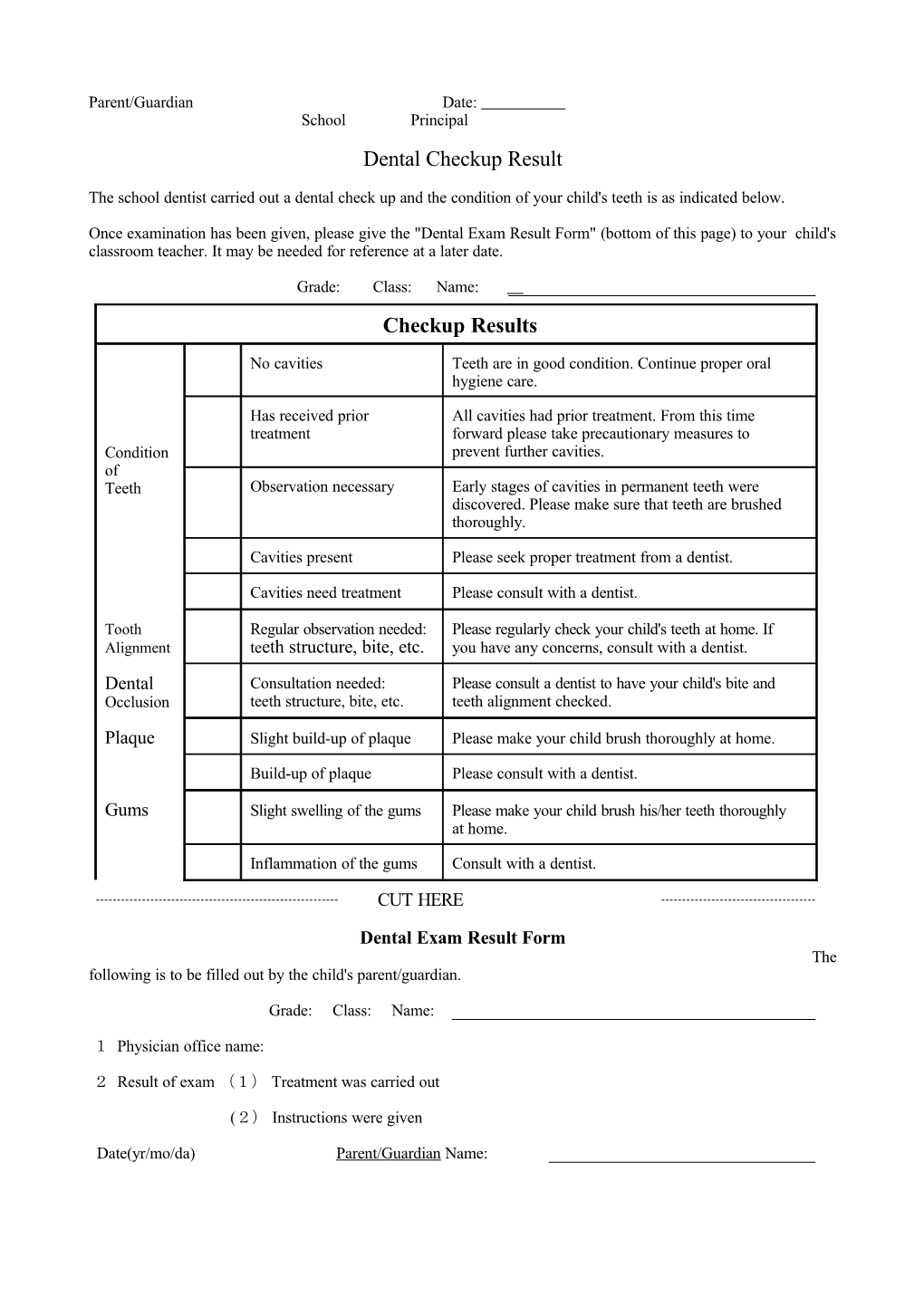
Checkup Results
No cavities Teeth are in good condition. Continue proper oral hygiene care.
Has received prior All cavities had prior treatment. From this time treatment forward please take precautionary measures to Condition prevent further cavities. of Teeth Observation necessary Early stages of cavities in permanent teeth were discovered. Please make sure that teeth are brushed thoroughly.
Cavities present Please seek proper treatment from a dentist.
Cavities need treatment Please consult with a dentist.
Tooth Regular observation needed: Please regularly check your child's teeth at home. If Alignment teeth structure, bite, etc. you have any concerns, consult with a dentist.
Dental Consultation needed: Please consult a dentist to have your child's bite and Occlusion teeth structure, bite, etc. teeth alignment checked.
Plaque Slight build-up of plaque Please make your child brush thoroughly at home.
Build-up of plaque Please consult with a dentist.
Gums Slight swelling of the gums Please make your child brush his/her teeth thoroughly at home.
Inflammation of the gums Consult with a dentist.
CUT HERE
Dental Exam Result Form The following is to be filled out by the child's parent/guardian.
Grade: Class: Name:
1 Physician office name:
2 Result of exam (1) Treatment was carried out
(2) Instructions were given
Date(yr/mo/da) Parent/Guardian Name: