Supplementary material
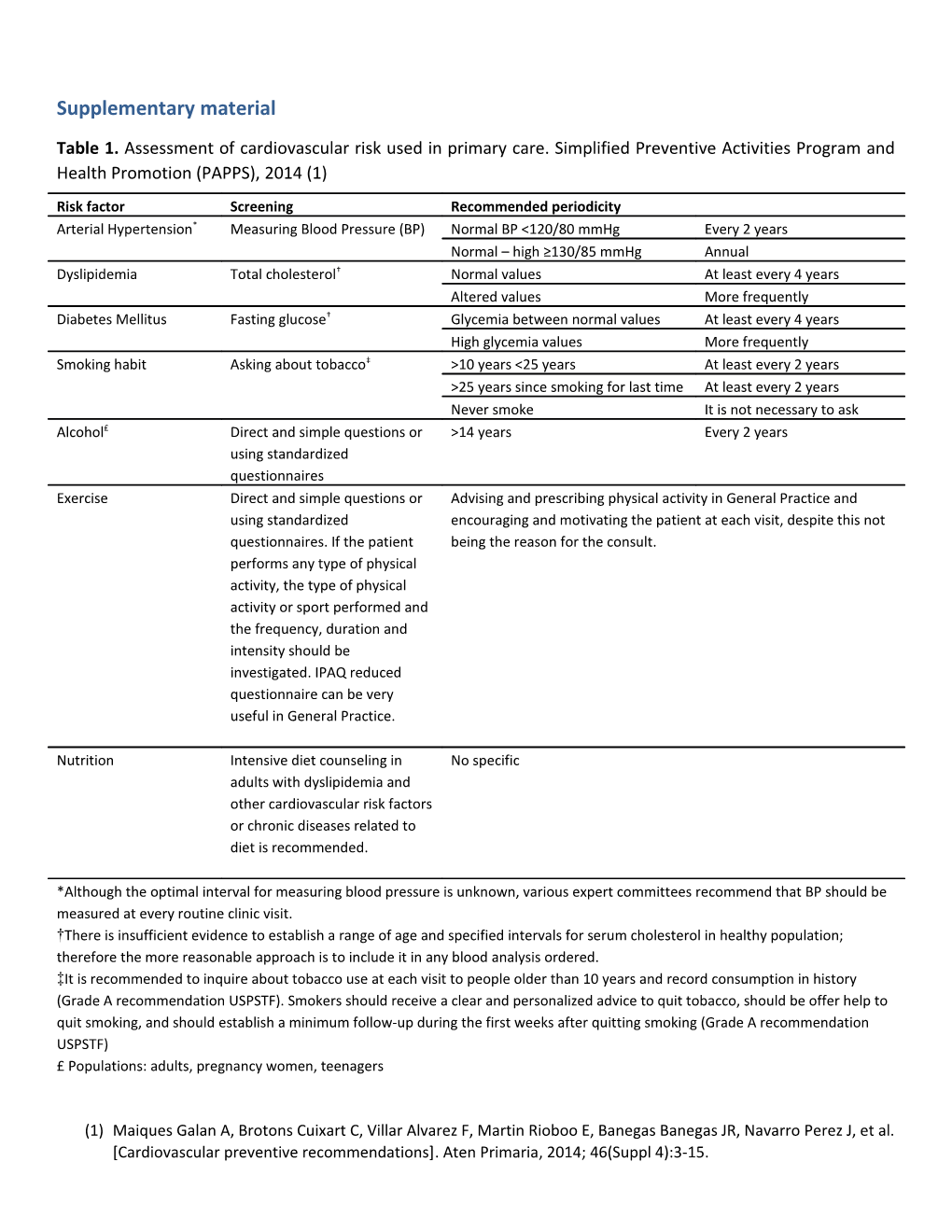
Table 1. Assessment of cardiovascular risk used in primary care. Simplified Preventive Activities Program and Health Promotion (PAPPS), 2014 (1)
Risk factor Screening Recommended periodicity Arterial Hypertension* Measuring Blood Pressure (BP) Normal BP <120/80 mmHg Every 2 years Normal – high ≥130/85 mmHg Annual Dyslipidemia Total cholesterol† Normal values At least every 4 years Altered values More frequently Diabetes Mellitus Fasting glucose† Glycemia between normal values At least every 4 years High glycemia values More frequently Smoking habit Asking about tobacco‡ >10 years <25 years At least every 2 years >25 years since smoking for last time At least every 2 years Never smoke It is not necessary to ask Alcohol£ Direct and simple questions or >14 years Every 2 years using standardized questionnaires Exercise Direct and simple questions or Advising and prescribing physical activity in General Practice and using standardized encouraging and motivating the patient at each visit, despite this not questionnaires. If the patient being the reason for the consult. performs any type of physical activity, the type of physical activity or sport performed and the frequency, duration and intensity should be investigated. IPAQ reduced questionnaire can be very useful in General Practice.
Nutrition Intensive diet counseling in No specific adults with dyslipidemia and other cardiovascular risk factors or chronic diseases related to diet is recommended.
*Although the optimal interval for measuring blood pressure is unknown, various expert committees recommend that BP should be measured at every routine clinic visit. †There is insufficient evidence to establish a range of age and specified intervals for serum cholesterol in healthy population; therefore the more reasonable approach is to include it in any blood analysis ordered. ‡It is recommended to inquire about tobacco use at each visit to people older than 10 years and record consumption in history (Grade A recommendation USPSTF). Smokers should receive a clear and personalized advice to quit tobacco, should be offer help to quit smoking, and should establish a minimum follow-up during the first weeks after quitting smoking (Grade A recommendation USPSTF) £ Populations: adults, pregnancy women, teenagers
(1) Maiques Galan A, Brotons Cuixart C, Villar Alvarez F, Martin Rioboo E, Banegas Banegas JR, Navarro Perez J, et al. [Cardiovascular preventive recommendations]. Aten Primaria, 2014; 46(Suppl 4):3-15. Validated 14-item Questionnaire of Mediterranean diet adherence. Martinez-Gonzalez, M. A., A. Garcia-Arellano, et al. (2012). "A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: the PREDIMED trial." PLoS One 7(8): e43134.
Criteria for 1 point
1. Do you use olive oil as main culinary fat? Yes
2. How much olive oil do you consume in a given day (including oil used for frying, salads, out- ≥4 tbsp of-house meals, etc.)?
3. How many vegetable servings do you consume per day? (1 serving : 200g [consider side ≥2 (≥1 portion raw or dishes as half a serving]) as a salad)
4. How many fruit units (including natural fruit juices) do you consume per day? ≥3
5. How many servings of red meat, hamburger, or meat products (ham, sausage, etc.) do you <1 consume per day? (1 serving: 100–150 g)
6. How many servings of butter, margarine, or cream do you consume per day? (1 serving: 12 <1 g)
7. How many sweet or carbonated beverages do you drink per day? <1
8. How much wine do you drink per week? ≥7 glasses
9. How many servings of legumes do you consume per week? (1 serving : 150 g) ≥3
10. How many servings of fish or shellfish do you consume per week? (1 serving 100–150 g of ≥3 fish or 4–5 units or 200 g of shellfish)
11. How many times per week do you consume commercial sweets or pastries (not <3 homemade), such as cakes, cookies, biscuits, or custard?
12. How many servings of nuts (including peanuts) do you consume per week? (1 serving 30 g) ≥3
13. Do you preferentially consume chicken, turkey, or rabbit meat instead of veal, pork, Yes hamburger, or sausage? 14. How many times per week do you consume vegetables, pasta, rice, or other dishes seasoned with sofrito (sauce made with tomato and onion, leek, or garlic and simmered with ≥2 olive oil)? Geriatric Depression Scale GDS-15 and GDS-4 Almeida OP, Almeida SA; Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry. 1999 Oct;14(10):858-65.
GDS-15 Yes No Are you basically satisfied with your life? 1 Have you dropped many of your activities and interests? 1 Do you feel that your life is empty? 1 Do you often get bored? 1 Are you in good spirits most of the time? 1 Are you afraid that something bad is going to happen to you? 1 Do you feel happy most of the time? 1 Do you often feel helpless? 1 Do you prefer to stay at home, rather than go out and do new things? 1 Do you feel you have more problems with memory than most? 1 Do you think it is wonderful to be alive? 1 Do you feel pretty worthless the way you are now? 1 Do you feel full of energy? 1 Do you feel that your situation is hopeless? 1 Do you think that most people are better off than you are? 1 15-item GDS score* A count >=5 suggests depression
GDS-4 Yes No Are you basically satisfied with your life? 1 Do you feel that your life is empty? 1 Are you afraid that something bad is going to happen to you? 1 Do you feel happy most of the time? 1
4-Item GDS score*
A count >=2 suggests depression Principles that guided these recommendations The principles that have guided the development of this document are:
Principle Explanation
All those involved in the care of PsD patients, not merely rheumatologists and dermatologists, were included. Internists, primary care physicians, nurses and patients were consulted. Participation It is not the intention of this paper to surpass the field of other specialists, but to respond to a need.
It should be adapted to a simpler and practical document for every day practice that can be Applicability easily handled by professionals at various levels.
All professionals involved must be informed of the problems these patients have. Dissemination This document and its recommendations should be adapted to the context or needs of different health professionals.
Utility The document and its materials should help manage comorbidity.
Flexibility It should be adaptable to different contexts, not a rigid document.
Validity The recommendations should be based on the best available evidence.
In front of different alternatives, we should always choose the one benefits the patient most, Patient centeredness and to facilitate their self-care.
Educational character The document should or can be used as a training material. Continuous feedback is welcome.