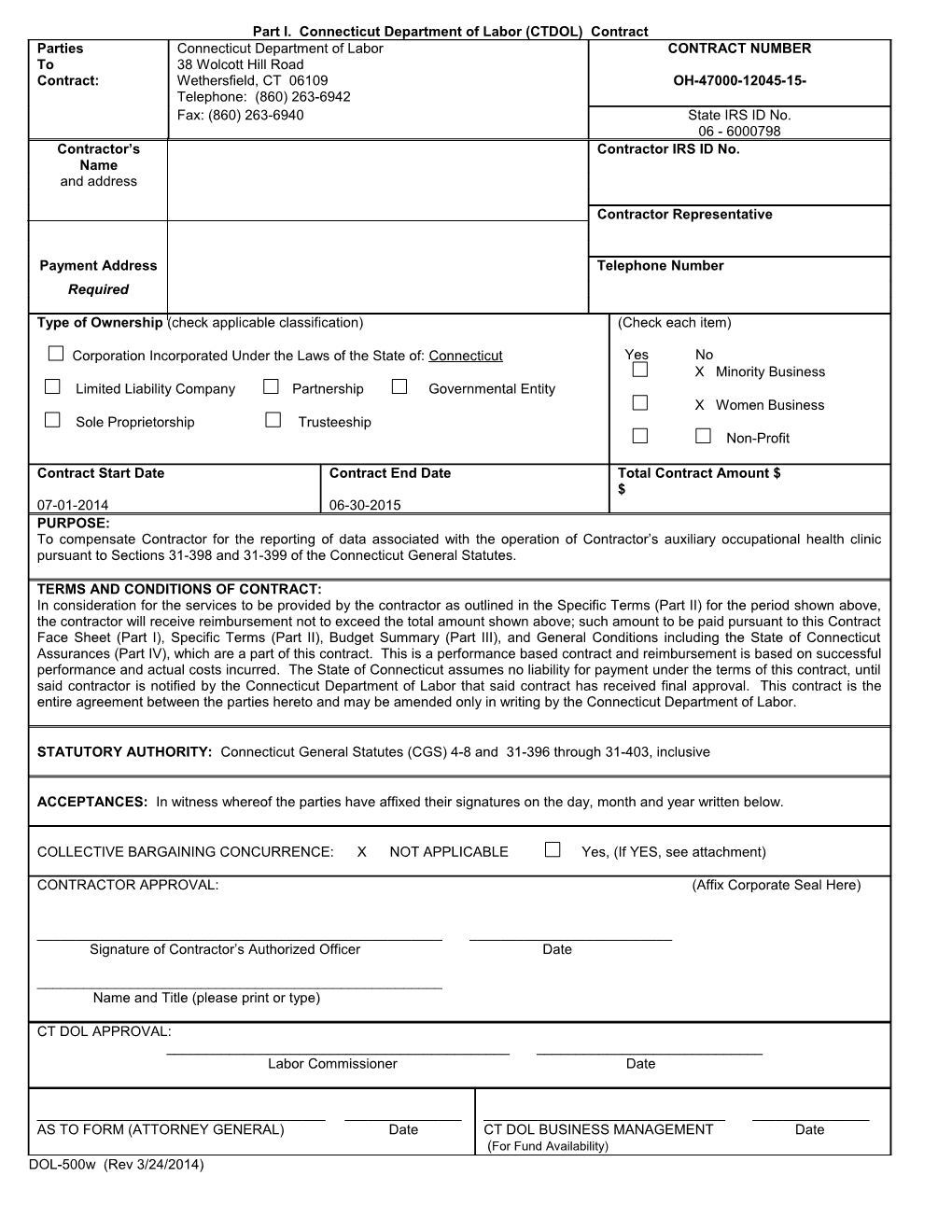
Part I. Connecticut Department of Labor (CTDOL) Contract Parties Connecticut Department of Labor CONTRACT NUMBER To 38 Wolcott Hill Road Contract: Wethersfield, CT 06109 OH-47000-12045-15- Telephone: (860) 263-6942 Fax: (860) 263-6940 State IRS ID No. 06 - 6000798 Contractor’s Contractor IRS ID No. Name and address
Contractor Representative
Payment Address Telephone Number Required
Type of Ownership (check applicable classification) (Check each item)
Corporation Incorporated Under the Laws of the State of: Connecticut Yes No X Minority Business Limited Liability Company Partnership Governmental Entity X Women Business Sole Proprietorship Trusteeship Non-Profit
Contract Start Date Contract End Date Total Contract Amount $ $ 07-01-2014 06-30-2015 PURPOSE: To compensate Contractor for the reporting of data associated with the operation of Contractor’s auxiliary occupational health clinic pursuant to Sections 31-398 and 31-399 of the Connecticut General Statutes.
TERMS AND CONDITIONS OF CONTRACT: In consideration for the services to be provided by the contractor as outlined in the Specific Terms (Part II) for the period shown above, the contractor will receive reimbursement not to exceed the total amount shown above; such amount to be paid pursuant to this Contract Face Sheet (Part I), Specific Terms (Part II), Budget Summary (Part III), and General Conditions including the State of Connecticut Assurances (Part IV), which are a part of this contract. This is a performance based contract and reimbursement is based on successful performance and actual costs incurred. The State of Connecticut assumes no liability for payment under the terms of this contract, until said contractor is notified by the Connecticut Department of Labor that said contract has received final approval. This contract is the entire agreement between the parties hereto and may be amended only in writing by the Connecticut Department of Labor.
STATUTORY AUTHORITY: Connecticut General Statutes (CGS) 4-8 and 31-396 through 31-403, inclusive
ACCEPTANCES: In witness whereof the parties have affixed their signatures on the day, month and year written below.
COLLECTIVE BARGAINING CONCURRENCE: X NOT APPLICABLE Yes, (If YES, see attachment)
CONTRACTOR APPROVAL: (Affix Corporate Seal Here)
______Signature of Contractor’s Authorized Officer Date
______Name and Title (please print or type)
CT DOL APPROVAL: ______Labor Commissioner Date
______AS TO FORM (ATTORNEY GENERAL) Date CT DOL BUSINESS MANAGEMENT Date (For Fund Availability) DOL-500w (Rev 3/24/2014) Part II. SPECIFIC TERMS CONNECTICUT DEPARTMENT OF LABOR AUXILIARY OCCUPATIONAL HEALTH CLINICS
Bristol Hospital, dba Medworks
Bristol Hospital, dba Medworks, (the contractor) in the operation of its Auxiliary Occupational Health Clinic, shall report of data associated with the operation of Contractor’s auxiliary occupational health clinic pursuant to Sections 31-398 and 31-399 of the Connecticut General Statutes. In addition, Bristol Hospital, dba Medworks, agrees to meet the following requirements:
1. LIMITATION OF COST: A. Funding for this agreement shall be accounted for separately and shall be used by the Contractor for activities described hereunder and for no other purpose.
B. The Contractor shall conform to the line item detail set forth in the budget. Actual expenditures for individual budget line items may vary by the lesser of ten percent (10%) or $10,000 without the prior written approval of DOL.
C. A maximum of fifteen (15) percent of the total contract is allowable for administrative costs. Approval to incur costs in excess of the fifteen (15) percent cap for administrative costs must be obtained from the Occupational Health Clinics Advisory Committee.
D. Equipment or property purchased at a cost of $1,000 or more per item must be specifically identified by a line item in the budget. Requests for the purchase of equipment or property after the approval of the Proposal will require the written consent of DOL or a modification to the contract before purchase. Requests to purchase equipment must contain a description of the item(s) to be purchased, its projected usage, projected costs and adhere to guidelines specified in General Conditions-Section 11.
2. SPECIAL PAYMENT AND REPORTING TERMS: A.. 1. Financial reports and invoices are to be completed by the Contractor quarterly and are due on or before the 15th day of the quarter for the prior quarter's reporting period. The Contractor shall submit a signed original and a copy of form DOL-14, Invoice/Status of Funds Report, each quarter. The mailing address is:
ATTN: Director, OSHA State of Connecticut Department of Labor 38 Wolcott Hill Road Wethersfield, CT. 06109
2. (a) Quarterly allotments of funds will be released to the Contractor, contingent upon the submission of data on occupational injuries and illnesses during the previous quarter. (b) Any physician data deemed incomplete by the contracting officer must be corrected and resubmitted to the DOL.
B. The Contractor may request an advance payment equal to its interim cash needs arising during any given quarterly reimbursement period. A written justification explaining the necessity for an advance must accompany the DOL-14, Invoice/Status of Funds Report. If the Contractor requests continuing authority to operate on a cash advance basis, this determination will be made by the DOL based on justification provided by the Contractor.
C. The Contractor will not be compensated for any activities which could be included in a corporate medicine program or an employee wellness program. These activities include, but are not limited to: routine workers’ compensation cases, mandated examinations, pre-employment examinations, medical evaluation involving establishment of product liability, employee physical programs, employee wellness programs, employee drug testing programs, and evaluations consigned to independent medical examiners.
D. In order to assure processing by the State of Connecticut, Office of the Comptroller within the current fiscal year (July 1 through June 30th), the Contractor shall submit a DOL-14, Invoice/Status of Funds Report by June 5, of the current fiscal year, for the estimated final quarter's expenditure for the agreement, including any uninvoiced prior quarter's expenditures or adjustments. Failure to do so by the required date could result in a loss of funding to the Contractor for amounts not processable.
3. FINAL RECONCILIATION: A. The Contractor agrees to submit a final reconciliation on form DOL-14, Invoice/Status of Funds Report to the DOL, reporting actual expenditures for this agreement no later than thirty (30) days after the ending date of this agreement.
B. Any funds paid to the Contractor and remaining unspent after the end date of the agreement will be refunded to the DOL with the final reconciliation described in 3..A. above. The refund check must be made payable to "Treasurer, State of Connecticut".
(Rev 3/24/2014) 4. PERFORMANCE AND MONITORING: A. The Contractor agrees to report all occupational illnesses and injuries which are diagnosed during the contract period to the DOL , utilizing the form entitled “Physician’s Report of Occupational Disease”.
B. The DOL may make informal visits of reasonable frequency and duration with advanced notice for the purpose of program monitoring and evaluation. Such visits may include the examination of a reasonable number of patient files and records.
C. The DOL shall monitor the Contractor's overall program performance, inform the Contractor of any specific program deficiencies, and make requests for corrective action when necessary.
D. (1) The Contractor will be responsible for submitting an annual program report that complies with the guidelines specified in Attachment A, Annual Program Report Guidelines Occupational Health Clinics. The report must be submitted to the DOL on or before August 1or thirty one (31) days following the termination of the contract, which ever comes first. (2) The Contractor agrees to cooperate with the DOL by providing any other performance reports or information requested by the DOL for the purpose of evaluating the activities funded by this contract. A time schedule for regular reporting will be determined by the DOL.
E. As detailed in Section 3 (A) of the General Conditions of this contract, if for any reason the Contractor shall fail to fulfill in a timely and proper manner its obligations under this contract, the DOL shall thereupon have the right to terminate this agreement in accordance with Section 3 of the General Conditions. “Timely and proper manner,” as referred to in this contract, includes the submission of all contract materials and other paperwork to the DOL on or before the established deadlines.
F. The Contractor further agrees to abide by all terms, conditions, and specifications detailed in the DOL-approved response to the Request for Proposal for an Auxiliary or Occupational Health Clinic.
5. WITHHOLDING:
A. The Contractor shall not be relieved of liability to the DOL for damages sustained by the DOL by virtue of any breach of the agreement by the Contractor, and the DOL may withhold any payments to the Contractor for the purpose of set-off until such time as the exact amount of damages to the DOL is determined.
6. PUBLICITY:
A. The Contractor agrees to use reasonable means to inform the public that the State of Connecticut, Department of Labor provides financial support for the operation of its occupational health clinics by including a statement to this effect in any news releases, reports, or promotional materials.
7. LIABILITY
A. The Contractor agrees that while performing services specified in this agreement that it shall carry sufficient insurance (liability and/or other) as applicable according to the nature of the service to be performed so as to save harmless the State of Connecticut from any insurable cause whatsoever. If requested, certificates of such insurance shall be filed with the contracting agency prior to the performance of service.
(Rev 3/24/2014)
Part III. BUDGET SUMMARY SHEET (Option 1) A. Administrative Costs
1. Staff Salaries
2. Staff Fringe
3. Travel Detail
4. Rent Detail
5. Equipment Detail
6. Other Direct Costs Detail
7. Insurance and Bonding
8. Contractual: (Outsourced)
TOTAL ADMINISTRATIVE COSTS $
B. Program
1. Staff Salaries
2. Staff Fringe
3. Other Costs
4. Equipment
5. Rental Detail
6. Travel Costs
7. Insurance and Bonding
8. Contractual (Outsourced)
TOTAL PROGRAM COSTS $
TOTAL CONTRACT AMOUNT $ A. Administrative Costs
1. Administrative Staff Salaries * Position Title Number % of Time Total Number Total in this Weekly of Weeks Amount Activity Salary
Total Administrative Staff Salaries
* Provide rationale and justification for allocation to project.
2. Administrative Staff Fringe Benefits Description of Fringe Rate Amount of Rate Total Amount Applied A. FICA
B. Workers' Compensation
C. Health and Welfare Insurance
D. Unemployment Compensation
E. Other (Specify)
F. Other (Specify)
G. Other (Specify)
Total Fringe Benefits of Administrative Staff A. Administrative Costs 3. Travel Detail ** Travel (Specify by position) Miles per Rate Number Total Amount Week per Mile of Weeks
Total Staff Travel
** Provide a describe need for travel and the rationale for such travel.
4. Rent Detail Location (Address) Cost Total Project Number of Total per Square % Months Amount Square Footage used Foot
Maintenance (if separate)
Utilities (if separate)
5. Equipment Detail (Unit acquisition cost $ 1,000.00 or >, useful life 1 year or more)*** Description Number Purchase Rental Maint. No. of Total (Cost) (Cost) (Cost) Months Amount
Total Equipment Cost
*** Provide explanation for the need of the above items. A. Administrative Costs
6. Other Direct Cost Detail Description Cost Per item Total Amount
A. Other (Specify)
B. Other (Specify)
C. Other (Specify)
Total Other Direct Cost
7. Insurance and Bonding Total Amount
Total insurance and Bonding
8. Contractual - (Outsourced to subrecipients/vendors for program services) List: Name Contractor/Vendor Total Amount
B. Program
1. Program Staff Salaries * Position Title Number % of Time Total Number Total in this Weekly of Weeks Amount Activity Salary
Total Program Staff Salaries
* Provide rationale and justification for allocation to project.
2. Program Staff Fringe Benefits Description of Fringe Rate Amount of Rate Total Amount Applied A. FICA
B. Workers' Compensation
C. Health and Welfare Insurance
D. Unemployment Compensation
E. Other (Specify)
F. Other (Specify)
G. Other (Specify)
Total Program Fringe Benefits B. Program
3. Other Program Cost Detail Description Cost Per item Total Amount
A. Other (Specify)
B. Other (Specify)
C. Other (Specify)
Total Other Program
4. Program Equipment Detail (Unit acquisition cost $ 1,000.00 or >, useful life 1 year or more)*** Description Number Purchase Rental Maint. No. of Total (Cost) (Cost) (Cost) Months Amount
Total Program Equipment Cost *** Provide explanation for the need of the above items.
5. Program Rent Detail Location (Address) Cost per Total PROJECT Number of Total Square Square % Months Amount Foot Footage used
Maintenance (if separate)
Utilities (if separate)
Total Program Rent Detail B. Program
6. Program Travel Detail ** Travel (Specify by position) Miles per Rate Number Total Amount Week per Mile of Weeks
Total Program Travel Detail
** Provide a describe need for travel and the rationale for such travel.
7. Program Insurance and Bonding Total Amount
Total insurance and Bonding
8. Contractual - (Outsourced to subrecipients/vendors for program services) List: Name Contractor/Vendor and attach description Amount of services.
Total Contractual