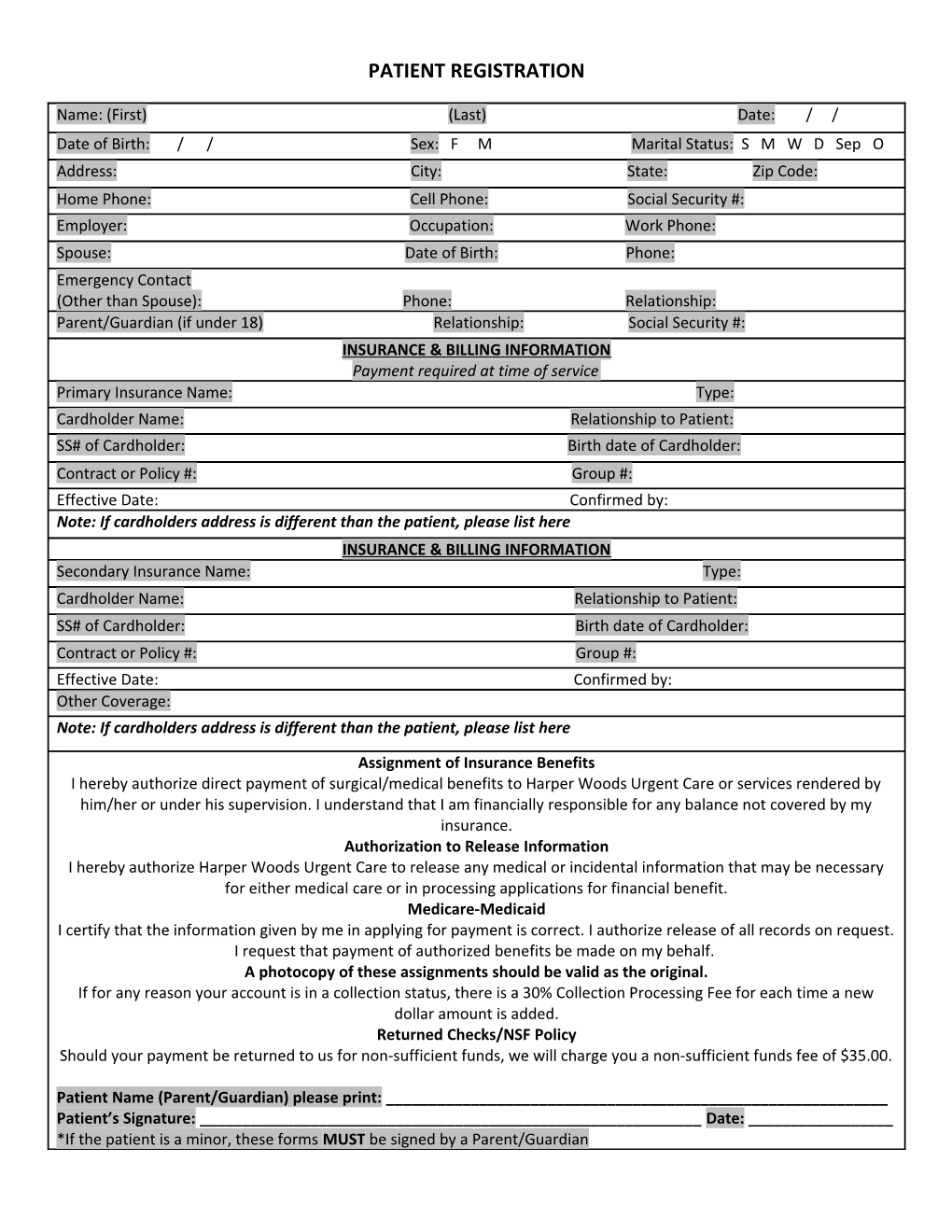
PATIENT REGISTRATION
Name: (First) (Last) Date: / / Date of Birth: / / Sex: F M Marital Status: S M W D Sep O Address: City: State: Zip Code: Home Phone: Cell Phone: Social Security #: Employer: Occupation: Work Phone: Spouse: Date of Birth: Phone: Emergency Contact (Other than Spouse): Phone: Relationship: Parent/Guardian (if under 18) Relationship: Social Security #: INSURANCE & BILLING INFORMATION Payment required at time of service Primary Insurance Name: Type: Cardholder Name: Relationship to Patient: SS# of Cardholder: Birth date of Cardholder: Contract or Policy #: Group #: Effective Date: Confirmed by: Note: If cardholders address is different than the patient, please list here INSURANCE & BILLING INFORMATION Secondary Insurance Name: Type: Cardholder Name: Relationship to Patient: SS# of Cardholder: Birth date of Cardholder: Contract or Policy #: Group #: Effective Date: Confirmed by: Other Coverage: Note: If cardholders address is different than the patient, please list here
Assignment of Insurance Benefits I hereby authorize direct payment of surgical/medical benefits to Harper Woods Urgent Care or services rendered by him/her or under his supervision. I understand that I am financially responsible for any balance not covered by my insurance. Authorization to Release Information I hereby authorize Harper Woods Urgent Care to release any medical or incidental information that may be necessary for either medical care or in processing applications for financial benefit. Medicare-Medicaid I certify that the information given by me in applying for payment is correct. I authorize release of all records on request. I request that payment of authorized benefits be made on my behalf. A photocopy of these assignments should be valid as the original. If for any reason your account is in a collection status, there is a 30% Collection Processing Fee for each time a new dollar amount is added. Returned Checks/NSF Policy Should your payment be returned to us for non-sufficient funds, we will charge you a non-sufficient funds fee of $35.00.
Patient Name (Parent/Guardian) please print: ______Patient’s Signature: ______Date: ______*If the patient is a minor, these forms MUST be signed by a Parent/Guardian