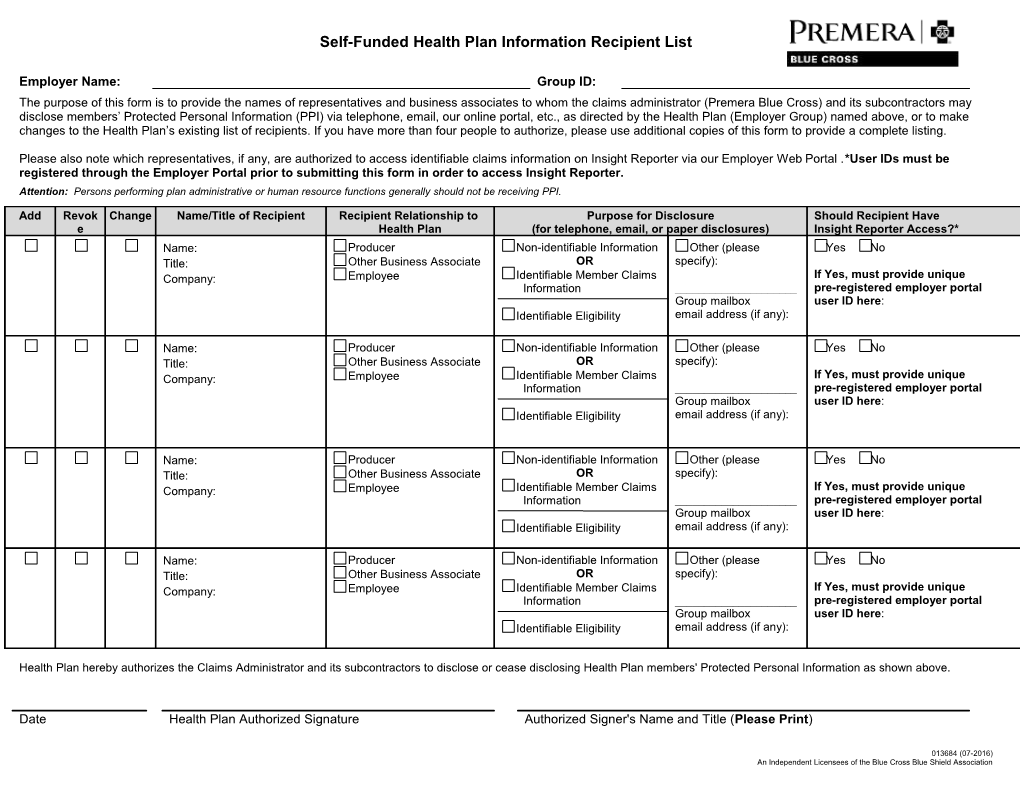
Self-Funded Health Plan Information Recipient List
Employer Name: Group ID: The purpose of this form is to provide the names of representatives and business associates to whom the claims administrator (Premera Blue Cross) and its subcontractors may disclose members’ Protected Personal Information (PPI) via telephone, email, our online portal, etc., as directed by the Health Plan (Employer Group) named above, or to make changes to the Health Plan’s existing list of recipients. If you have more than four people to authorize, please use additional copies of this form to provide a complete listing.
Please also note which representatives, if any, are authorized to access identifiable claims information on Insight Reporter via our Employer Web Portal .*User IDs must be registered through the Employer Portal prior to submitting this form in order to access Insight Reporter. Attention: Persons performing plan administrative or human resource functions generally should not be receiving PPI.
Add Revok Change Name/Title of Recipient Recipient Relationship to Purpose for Disclosure Should Recipient Have e Health Plan (for telephone, email, or paper disclosures) Insight Reporter Access?* Name: Producer Non-identifiable Information Other (please Yes No Title: Other Business Associate OR specify): Company: Employee Identifiable Member Claims If Yes, must provide unique Information ______pre-registered employer portal Group mailbox user ID here: Identifiable Eligibility email address (if any):
Name: Producer Non-identifiable Information Other (please Yes No Title: Other Business Associate OR specify): Company: Employee Identifiable Member Claims If Yes, must provide unique Information ______pre-registered employer portal Group mailbox user ID here: Identifiable Eligibility email address (if any):
Name: Producer Non-identifiable Information Other (please Yes No Title: Other Business Associate OR specify): Company: Employee Identifiable Member Claims If Yes, must provide unique Information ______pre-registered employer portal Group mailbox user ID here: Identifiable Eligibility email address (if any):
Name: Producer Non-identifiable Information Other (please Yes No Title: Other Business Associate OR specify): Company: Employee Identifiable Member Claims If Yes, must provide unique Information ______pre-registered employer portal Group mailbox user ID here: Identifiable Eligibility email address (if any):
Health Plan hereby authorizes the Claims Administrator and its subcontractors to disclose or cease disclosing Health Plan members' Protected Personal Information as shown above.
Date Health Plan Authorized Signature Authorized Signer's Name and Title (Please Print)
013684 (07-2016) An Independent Licensees of the Blue Cross Blue Shield Association