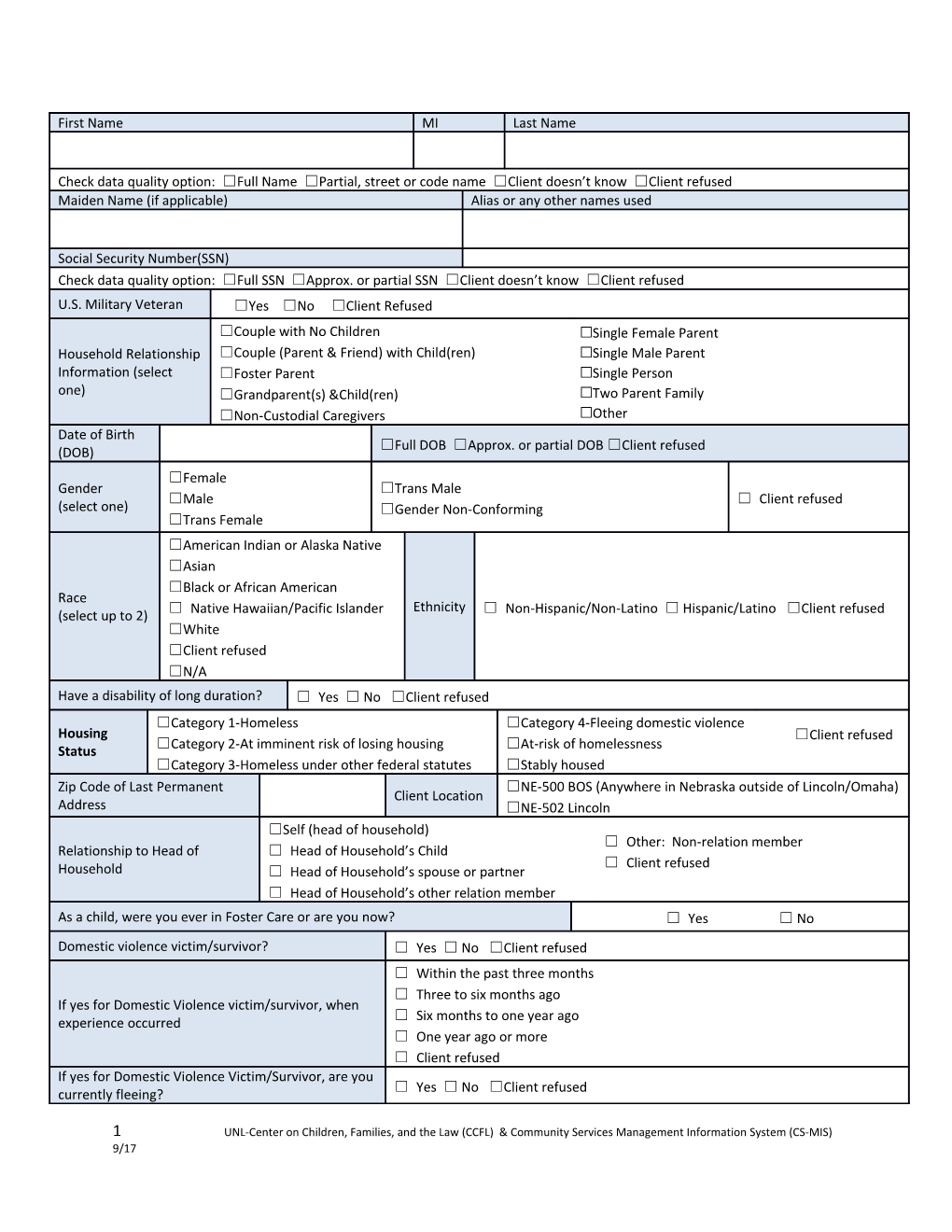
First Name MI Last Name
Check data quality option: ☐Full Name ☐Partial, street or code name ☐Client doesn’t know ☐Client refused Maiden Name (if applicable) Alias or any other names used
Social Security Number(SSN) Check data quality option: ☐Full SSN ☐Approx. or partial SSN ☐Client doesn’t know ☐Client refused U.S. Military Veteran ☐Yes ☐No ☐Client Refused ☐Couple with No Children ☐Single Female Parent Household Relationship ☐Couple (Parent & Friend) with Child(ren) ☐Single Male Parent Information (select ☐Foster Parent ☐Single Person one) ☐Grandparent(s) &Child(ren) ☐Two Parent Family ☐Non-Custodial Caregivers ☐Other Date of Birth ☐Full DOB ☐Approx. or partial DOB ☐Client refused (DOB) ☐Female Gender ☐Trans Male ☐Male ☐ Client refused (select one) ☐Gender Non-Conforming ☐Trans Female ☐American Indian or Alaska Native ☐Asian ☐Black or African American Race ☐ Native Hawaiian/Pacific Islander Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (select up to 2) ☐White ☐Client refused ☐N/A Have a disability of long duration? ☐ Yes ☐ No ☐Client refused ☐Category 1-Homeless ☐Category 4-Fleeing domestic violence Housing ☐Client refused ☐Category 2-At imminent risk of losing housing ☐At-risk of homelessness Status ☐Category 3-Homeless under other federal statutes ☐Stably housed Zip Code of Last Permanent ☐NE-500 BOS (Anywhere in Nebraska outside of Lincoln/Omaha) Client Location Address ☐NE-502 Lincoln ☐Self (head of household) ☐ Other: Non-relation member Relationship to Head of ☐ Head of Household’s Child ☐ Client refused Household ☐ Head of Household’s spouse or partner ☐ Head of Household’s other relation member As a child, were you ever in Foster Care or are you now? ☐ Yes ☐ No Domestic violence victim/survivor? ☐ Yes ☐ No ☐Client refused ☐ Within the past three months ☐ Three to six months ago If yes for Domestic Violence victim/survivor, when ☐ Six months to one year ago experience occurred ☐ One year ago or more ☐ Client refused If yes for Domestic Violence Victim/Survivor, are you ☐ Yes ☐ No ☐Client refused currently fleeing?
1 UNL-Center on Children, Families, and the Law (CCFL) & Community Services Management Information System (CS-MIS) 9/17 ☐ No schooling completed ☐ GED ☐ Nursery school to 4th grade ☐ Post-Secondary School ☐ 5th or 6th grade ☐ Some College ☐ 7th grade or 8th grade ☐ Some Technical School ☐ 9th grade ☐ Graduate Degree Highest level of education attained ☐ 10th grade ☐ Technical School Certification ☐ 11th grade ☐ Client refused ☐ 12th grade, no diploma ☐ Some High School ☐ High school diploma Income Information
Income from any source? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused Total Monthly CASH income: Write in total $ amount and complete the table below Total Monthly Income: $______Receives Income Sources Yes Monthly Amount $ No
AABD (Aid to Aged, Blind & Disabled) ☐ $ ☐ Alimony or Other Spousal Support ☐ $ ☐ Child Support ☐ $ ☐ Contributions from other People ☐ $ ☐ Earned Income (from job) ☐ $ ☐ General Assistance ☐ $ ☐ Pension or retirement income from job ☐ $ ☐ Pension/Retirement ☐ $ ☐ Private Disability Insurance ☐ $ ☐ Retirement Income from Social Security ☐ $ ☐ Self Employment Wages ☐ $ ☐ SSA ☐ $ ☐ SSDI ☐ $ ☐ SSI ☐ $ ☐ Stipend ☐ $ ☐ Unemployment Insurance ☐ $ ☐ VA Non-service connected disability compensation ☐ $ ☐ VA service-connected disability compensation ☐ $ ☐ Worker’s Compensation ☐ $ ☐ Other (specify): ☐ $ ☐
2 UNL-Center on Children, Families, and the Law (CCFL) & Community Services Management Information System (CS-MIS) 9/17 Non-Cash Benefits Information
Non-cash benefits from any source ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused Receives the following Non-cash Benefit Types: Yes Monthly Amount $ (if known) No Supplemental Nutrition Assistance Program (SNAP) ☐ $ ☐ (Food Stamps) Special Supplemental Nutrition for Women, infants, ☐ N/A ☐ children(WIC) TANF Child Care Services ☐ $ ☐ TANF Transportation services ☐ N/A ☐ Other TANF funded services ☐ N/A ☐ Other (specify): ☐ $ ☐ Health Insurance Information
Covered by Health Insurance ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused Type Covered Covered (Select all that apply) Yes No Medicaid ☐ ☐ Medicare ☐ ☐ State Children’s Health Insurance Program ☐ ☐ Veteran’s Administration (VA) Medical Services ☐ ☐ Employer-Provided Health Insurance ☐ ☐ Health Insurance obtained through COBRA ☐ ☐ Private Pay Health Insurance ☐ ☐ State Health Insurance for Adults ☐ ☐ Indian Health Services Program ☐ ☐ Other ( Specify): ☐ ☐ Client’s Residence/Last Permanent Address Street Address City State Zip code County of Current County of Legal Residence Residence Home Phone Number Cell Phone Work
Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
3 UNL-Center on Children, Families, and the Law (CCFL) & Community Services Management Information System (CS-MIS) 9/17 Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Trans Female ☐Client doesn’t know ☐Male (select one) ☐ Gender Non-Conforming ☐ Client refused ☐Trans Male Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member □ Medicaid □ Employer Provided □ Indian Health Covered by Health Insurance □ State Children’s □ COBRA □ Other (Specify): ☐ Yes ☐ No Health □ Private Pay □ Veteran’s Medical
Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Trans Female ☐Client doesn’t know ☐Male (select one) ☐Gender Non-Conforming ☐ Client refused ☐Trans Male Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member □ Medicaid □ Employer Provided □ Indian Health Covered by Health Insurance □ State Children’s □ COBRA □ Other (Specify): ☐ Yes ☐ No Health □ Private Pay □ Veteran’s Medical
4 UNL-Center on Children, Families, and the Law (CCFL) & Community Services Management Information System (CS-MIS) 9/17 Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Trans Female ☐Client doesn’t know ☐Male (select one) ☐Gender Non-Conforming ☐ Client refused ☐Trans Male Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member □ Medicaid □ Employer Provided □ Indian Health Covered by Health Insurance □ State Children’s □ COBRA □ Other (Specify): ☐ Yes ☐ No Health □ Private Pay □ Veteran’s Medical
Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Trans Female ☐Client doesn’t know ☐Male (select one) ☐Gender Non-Conforming ☐ Client refused ☐Trans Male Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member Covered by Health Insurance □ Medicaid □ Employer Provided □ Indian Health ☐ Yes ☐ No □ State Children’s □ COBRA □ Other (Specify): Health □ Private Pay
5 UNL-Center on Children, Families, and the Law (CCFL) & Community Services Management Information System (CS-MIS) 9/17 □ Veteran’s Medical
6 UNL-Center on Children, Families, and the Law (CCFL) & Community Services Management Information System (CS-MIS) 9/17 I ______understand information about me and/or my dependents listed below is entered into a database system called ServicePoint. This system helps to better understand homelessness, to improve service delivery and to evaluate the effectiveness of services provided. Participation in data collection is a critical component of our community’s ability to provide the most effective services and housing possible. The information that is collected is protected by limiting access to the database and limiting what information may be shared. Access to the data and sharing of the data is in compliance with the standards set by the federal, state and local regulations governing confidentially of client records. Every person and agency that is authorized to read or enter information into the system has signed an agreement to maintain the security and confidentiality of the information.
By signing this form, I authorize the following: The information collected by this agency will be included in ServicePoint and only partner agencies, which have entered into an HMIS Agency Participation Agreement, may be used to:
Produce a client profile at intake that will be shared with collaborating agencies
Produce aggregate level reports regarding use of services
Track individual program-level outcomes
Identify unfilled service needs and plan for enhancements
Allocate resources among agencies engaged in services
By signing this form, I authorize the following: I authorize the partner agencies and their representatives to share basic information regarding my family members listed below and/or me. I understand that this information is for the purpose of assessing my/our needs for housing, utility assistance, food, counseling and/or other services.
The information may consist of the following PPI (Personal Protected Information):
Name Homeless History Disabling Condition Date of Birth Family Composition Photo (if applicable) Social Security Number Income/Non-cash Housing information Gender Veteran Status Health Insurance Status Ethnicity and Race Domestic Violence Client Location Residence Prior to Project Entry VI-SPDAT
I Understand That:
The partner agencies have signed agreements to treat my information in a professional and confidential manner. I have the right to view the client confidentiality polices used by the HMIS partner agencies
Staff members of the partner agencies who will see my information have signed agreements to maintain confidentiality regarding my information. 10/2016 The release of my information does not guarantee that I will receive assistance; my refusal to authorize the use of my information does not disqualify me from receiving assistance.
My records are protected by federal, state, and local regulations governing confidentially of client records and cannot be disclosed without my written consent unless otherwise provided for in the regulations.
This authorization will remain in effect until I revoke it in writing, and I may revoke authorization at any time, if I revoke my authorization, all information about me already in the database will remain.
This release if valid for ______years from the date of my signature below.
I understand I may withdraw my consent at any time.
Partner Agencies: A list of the partner agencies within the Nebraska Homeless Management Information System may be viewed prior to signing this form.
List all Dependent Children under 18 in the household, if any (first, last and DOB) 1. 2. 3. 4. 5. 6. 7. 8.
Auditors or funders who have legal rights to review the work of this agency, including the U.S. Department of Housing and Urban Development and Nebraska Department of Health and Human Services Homeless Assistance Program may see my complete file in HMIS if services received are funded by their Department/s.
Please initial one of the following levels of consent:
___ I give authorization for me and my dependents listed above, Protected Personal and relevant Information to be entered into the NMIS and shared between Partner Agencies.
Or
___I do not consent to the inclusion of personal information in the NMIS about me and any dependents listed above.
______Consumer’s Signature Date
______Agency Staff Name(print) Agency Staff Signature Date 10/2016 10/2016