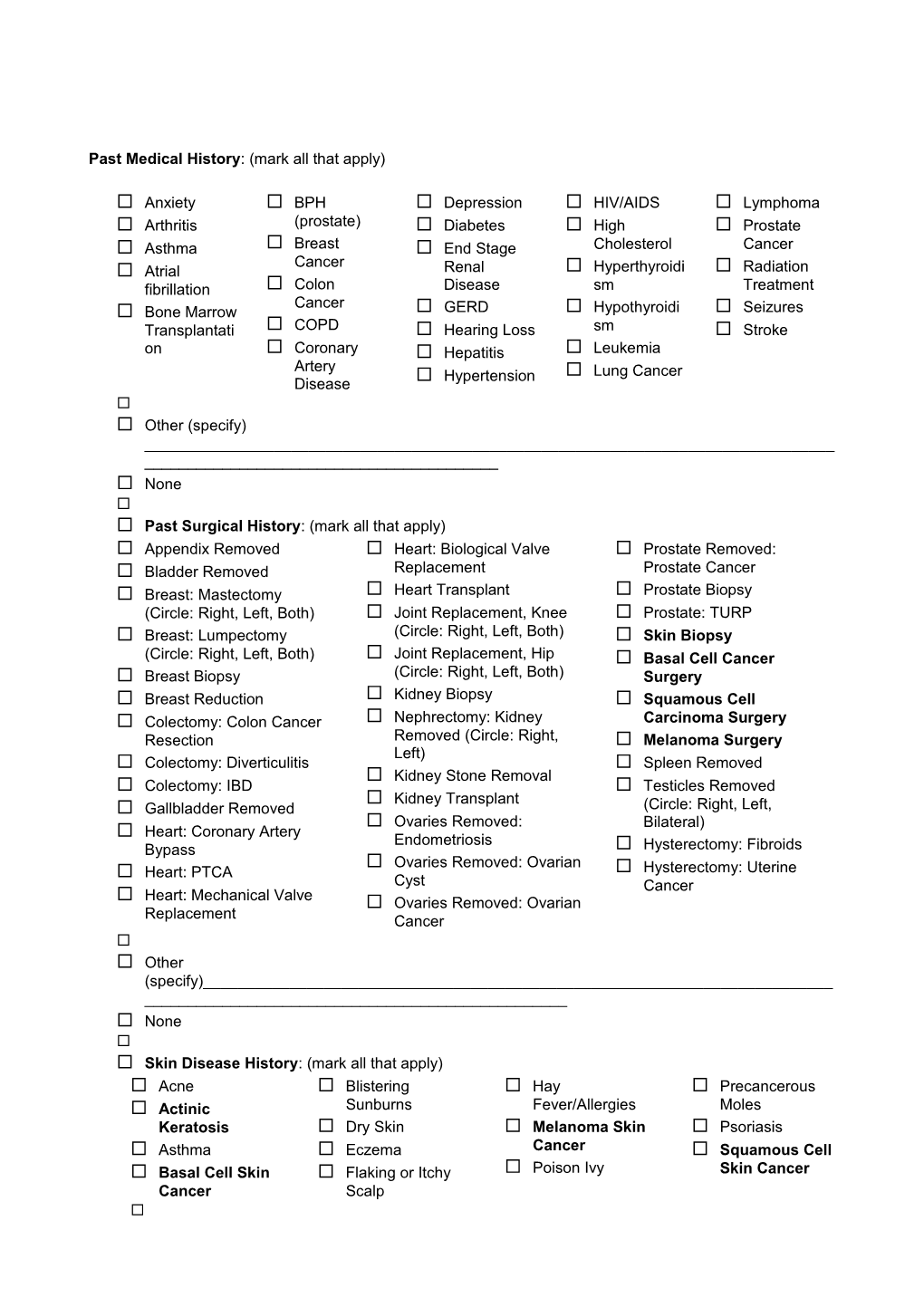
Past Medical History: (mark all that apply)
Anxiety BPH Depression HIV/AIDS Lymphoma Arthritis (prostate) Diabetes High Prostate Asthma Breast End Stage Cholesterol Cancer Cancer Atrial Renal Hyperthyroidi Radiation fibrillation Colon Disease sm Treatment Cancer Bone Marrow GERD Hypothyroidi Seizures Transplantati COPD Hearing Loss sm Stroke on Coronary Hepatitis Leukemia Artery Hypertension Lung Cancer Disease Other (specify) ______ None Past Surgical History: (mark all that apply) Appendix Removed Heart: Biological Valve Prostate Removed: Bladder Removed Replacement Prostate Cancer Breast: Mastectomy Heart Transplant Prostate Biopsy (Circle: Right, Left, Both) Joint Replacement, Knee Prostate: TURP Breast: Lumpectomy (Circle: Right, Left, Both) Skin Biopsy (Circle: Right, Left, Both) Joint Replacement, Hip Basal Cell Cancer Breast Biopsy (Circle: Right, Left, Both) Surgery Breast Reduction Kidney Biopsy Squamous Cell Colectomy: Colon Cancer Nephrectomy: Kidney Carcinoma Surgery Resection Removed (Circle: Right, Melanoma Surgery Left) Colectomy: Diverticulitis Spleen Removed Kidney Stone Removal Colectomy: IBD Testicles Removed Kidney Transplant Gallbladder Removed (Circle: Right, Left, Ovaries Removed: Bilateral) Heart: Coronary Artery Endometriosis Bypass Hysterectomy: Fibroids Ovaries Removed: Ovarian Heart: PTCA Hysterectomy: Uterine Cyst Cancer Heart: Mechanical Valve Ovaries Removed: Ovarian Replacement Cancer Other (specify)______ None Skin Disease History: (mark all that apply) Acne Blistering Hay Precancerous Actinic Sunburns Fever/Allergies Moles Keratosis Dry Skin Melanoma Skin Psoriasis Asthma Eczema Cancer Squamous Cell Basal Cell Skin Flaking or Itchy Poison Ivy Skin Cancer Cancer Scalp Other ______ None Do you have a family history of MELANOMA (NOT the same as basal cell or squamous cell carcinoma)?
Yes
No If YES to melanoma, which relative(s)? ______ If YES to melanoma, any other family history (breast, ovarian, pancreatic or prostate cancers)? ______ Have you had a Pneumonia Vaccine? Yes/NO (circle one) If Yes When? ______ Height ______Weight ______BMI ______ Medications: (enter all current medications and strengths) □ None ______ Drug Allergies: (do they cause anaphylaxis, angioedema, diarrhea, fatigue, GI upset, hives, liver toxicity, or rash?) ______
□ No Known Drug Allergies □ Latex Social History: (mark all that apply) Sexual History: Sexually active with one Sexually active with more Not sexually active partner than one partner Same Sex-Sexual partner 3 or more drinks per Safety: Illicit Drug Use: day I feel safe at home. Drug Use How many times in the I do not feel safe at home. past year have you had 4 IV Drug Use or more drinks in a day? Cigarette Smoking Less than Twice per Year (must answer): More than Twice per Alcohol (EtOH) Use: Current every day smoker Year None Current some day smoker Less than 1 drink a day Former smoker 1-2 Drinks per day Never smoker Other______ Review of Systems: Are you currently experiencing any of the following? (Please check yes or no for the following) Headaches Yes No Dryness Yes No Blurred Vision Yes No Moodiness/Anxiety Yes No Fever/Having signs of illness Yes No Problems Healing/Scars Yes No Other Symptoms: ______ Alerts: Are you currently using or experiencing any of the following? (Please check yes or no for the following) Blood thinners Yes No Currently using Accutane/Biologic Yes No Allergic to adhesive Yes No Premedication prior to procedures Yes No Pacemaker Yes No Artificial Joints within past 2 years Yes No Are you pregnant Yes No If yes, due date: ______ Other Symptoms: ______ PHARMACY (You may ALSO list your mail-order pharmacy - include PHONE and FAX number) Name ______Zip Code (or nearby zip code) ______(This is the fastest way for us to search) Address (or major cross-roads if not known): ______ Phone number: ______