Strangles Horse Owner Fact Sheet
Strangles (Streptococcus equi subspecies equi infection)
What is strangles?
Strangles is a highly contagious infectious disease caused by bacteria called Streptococcus equi subspecies equi (S. equi). It is the most commonly diagnosed equine infectious disease in the United Kingdom. It is an infection of the upper respiratory tract (nose and throat) and can cause abscesses in the head region. Strangles is not usually fatal but can cause severe disease such as not being able to eat or, rarely, struggling to breath due to the abscesses pushing on the airway. Rarely, complications can occur such as bastard (metastatic) strangles, where abscesses can form elsewhere in the body, and purpura haemorrhagica, where the body’s immune system starts attacking the body tissues.
How is the disease spread?
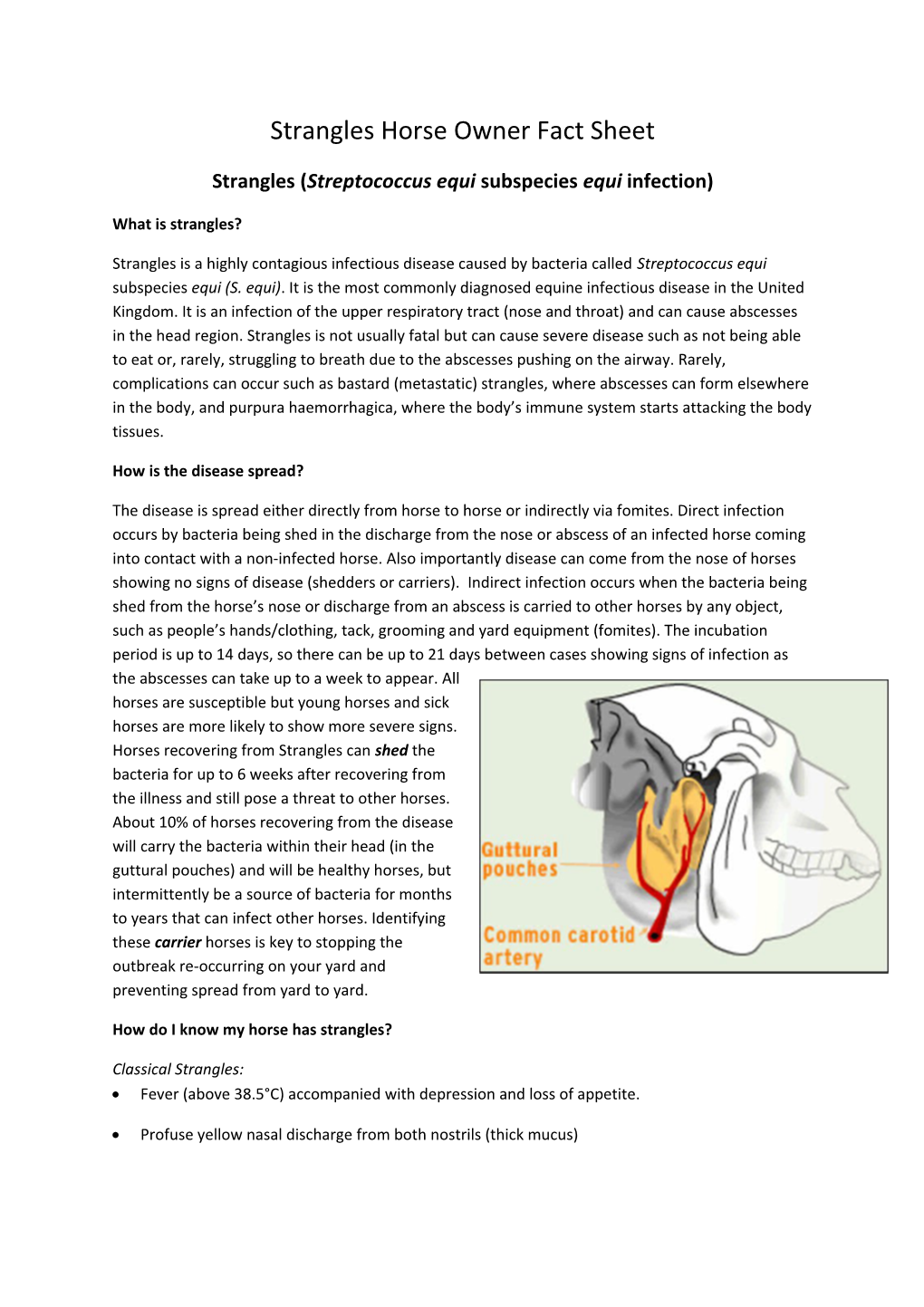
The disease is spread either directly from horse to horse or indirectly via fomites. Direct infection occurs by bacteria being shed in the discharge from the nose or abscess of an infected horse coming into contact with a non-infected horse. Also importantly disease can come from the nose of horses showing no signs of disease (shedders or carriers). Indirect infection occurs when the bacteria being shed from the horse’s nose or discharge from an abscess is carried to other horses by any object, such as people’s hands/clothing, tack, grooming and yard equipment (fomites). The incubation period is up to 14 days, so there can be up to 21 days between cases showing signs of infection as the abscesses can take up to a week to appear. All horses are susceptible but young horses and sick horses are more likely to show more severe signs. Horses recovering from Strangles can shed the bacteria for up to 6 weeks after recovering from the illness and still pose a threat to other horses. About 10% of horses recovering from the disease will carry the bacteria within their head (in the guttural pouches) and will be healthy horses, but intermittently be a source of bacteria for months to years that can infect other horses. Identifying these carrier horses is key to stopping the outbreak re-occurring on your yard and preventing spread from yard to yard.
How do I know my horse has strangles?
Classical Strangles: Fever (above 38.5°C) accompanied with depression and loss of appetite.
Profuse yellow nasal discharge from both nostrils (thick mucus) Swellings on the side of the head and throat which may burst and discharge pus. These abscesses are usually hot and painful and occur some days after the initial fever.
Sore throat – difficulty eating, extending the head.
Atypical Strangles: (becoming more common especially in healthy adult horses) Mild short term fever – may loose appetite for a brief period of time.
Mild clear nasal discharge.
No abscess formation.
These horses are a risk to other horses and should be treated as infectious.
N.B. These clinical signs can be seen with a wide variety of diseases and not just strangles.
Isolating affected horses and seeking immediate veterinary attention is essential to stop the spread of the disease.
Diagnosis:
Diagnosis of an individual horse is based on identifying the bacteria cultured (grown) in a lab from throat swabs or aspirates/swabs from abscesses. However the bacteria is very difficult to grow and will only be found in about 30% of cases. Therefore a molecular technique (PCR) can be performed on the samples to increase the sensitivity of the test. However horses that do have strangles may have negative results for culture and PCR; these horses will need another sample at your veterinary surgeon’s discretion. If the horse has classical clinical signs or the bacteria has been already identified on the yard laboratory confirmation may not be required at the attending veterinary surgeon’s discretion. A new blood test (serology) is available that detects antibodies to the bacteria The antibodies take up to two weeks to form and therefore the test cannot be used in the initial stages of infection. The antibodies stay elevated for up to six months after infection and therefore a positive test may not mean your horse has strangles at that moment, just that the horse has been exposed to the disease in the last six months. Culture and PCR on swabs would be required to confirm active infection. The blood test can be used to highlight potential carriers. To confirm a horse is a carrier, endoscopy of the head (guttural pouches) is required and washes need to be taken and submitted for culture and PCR.
Isolation:
Strict hygiene and disinfection protocols are essential. Personnel and equipment that only look after the isolated horses is ideal. Creating an isolation area which has a foot dip and specific overalls is important. Nothing that enters the isolation area should leave the isolation area without thorough disinfection.
Treatment:
If the diagnosis is positive either based on clinical signs, culture, PCR or blood test then your veterinary surgeon will discuss treatment options with you. Most cases just need intensive nursing care including rest and a dry warm environment. Feeding soft palatable feeds is important. Abscesses can be hot-packed to encourage them to burst. Occasionally your vet may lance the abscess to enable them to drain. Use of antibiotics in strangles cases remains controversial and should be judged on an individual patient basis by the attending veterinary surgeon. However, most horses do not need antibiotics. Severe cases may require antibiotics and using antibiotics in early cases (e.g. those who have very recently spiked a fever) may be beneficial at your veterinary surgeon’s discretion.
Control and Prevention:
Recovered horses can shed bacteria for at least 4 weeks. Maintaining isolation during this time is critical.
At the end of this time screening the recovered horses for carrier horses is important (around 10% of affected horses may be carriers.) This can be done a number of ways depending on the individual yard circumstances.
o Culture and PCR of three throat swabs (nasopharyngeal) 5-7 days apart
. Any horses returning positive results need guttural pouch lavage via endoscopy
o Culture and PCR of one guttural pouch lavage via endoscopy
o Serology blood test
. Any horses with positive results need guttural pouch lavage via endoscopy
Preventing strangles entering a yard: Isolate all horses for three weeks and monitor horses closely for a fever and nasal discharge.
Consider performing serology blood test on all new horses moving on to a yard. Horses with positive results should have one guttural pouch lavage via endoscopy and the fluid collected submitted for culture and PCR.
Equilis StrepE was a vaccine which is injected into the lip is now available again.
o Initial course is two injections 4 weeks a part.
o Then depending on the risk of disease to the yard of strangles then either 3 or 6 monthly boosters. This should be determined in consultation with your veterinary surgeon. o The vaccine can cause your horse to be unwell for 24 hours after vaccination and some horses will need a small amount of anti-inflammatory such as phenylbutazone ‘bute’.
o It is live bacterial vaccine and therefore different to tetanus and influenza (‘flu’) that horse owners in the UK are used to. Therefore careful discussion with your veterinary surgeon whether this vaccination is appropriate for your yard.
A custom made prevention plan to which all members of yard agree to be devised by a veterinary surgeon is the gold standard approach to preventing strangles. The prevention strategies can vary and balance of risk against benefit – see risk assessment guide.
Risk Assessment Guide
Cool Hot
Single horse Multiple horses Multiple horses & owners Large yard ; Livery yard
No contact with other horsesOccasional contact with Regular contact with Frequent contact with horses horses of known health horses of known health of unknown health status status status No new arrivals into yard New arrivals unusual New arrivals several Frequent new arrivals; times each year high throughput of Previoushorses strangles; no No previous strangles No previous strangles Previous strangles; but investigations for carriers investigations for carriers Annual health Quarantine of new Quarantine of new No quarantine or testing plans/preventive arrivals with testing arrivals but no testing of new arrivals health plans in place Communal water Separate water troughs troughs; shared feed No personnel traffic between Little personnel traffic between Personnel traffic between Personnelutensils traffic between horses, biosecurity in place horses, with biosecurity horses, with biosecurity horses, no biosecurity
Low risk (disease unlikely) High risk (disease more likely)
Vaccination optional. 6 month vaccination intervals 3 month vaccination intervals May be appropriate for risk-averse owners