Vaccine Immunology Claire-Anne Siegrist
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lactoferrin and Its Detection Methods: a Review
nutrients Review Lactoferrin and Its Detection Methods: A Review Yingqi Zhang, Chao Lu and Jin Zhang * Department of Chemical and Biochemical Engineering, University of Western Ontario, London, ON N6A 5B9, Canada; [email protected] (Y.Z.); [email protected] (C.L.) * Correspondence: [email protected] Abstract: Lactoferrin (LF) is one of the major functional proteins in maintaining human health due to its antioxidant, antibacterial, antiviral, and anti-inflammatory activities. Abnormal levels of LF in the human body are related to some serious diseases, such as inflammatory bowel disease, Alzheimer’s disease and dry eye disease. Recent studies indicate that LF can be used as a biomarker for diagnosis of these diseases. Many methods have been developed to detect the level of LF. In this review, the biofunctions of LF and its potential to work as a biomarker are introduced. In addition, the current methods of detecting lactoferrin have been presented and discussed. We hope that this review will inspire efforts in the development of new sensing systems for LF detection. Keywords: lactoferrin; biomarkers; immunoassay; instrumental analysis; sensor 1. Introduction Lactoferrin (known as lactotransferrin, LF), with a molecular weight of about 80 kDa, is a functional glycoprotein, which contains about 690 amino acid residues. It was first isolated from bovine milk by Sorensen in 1939 and was first isolated from human milk by Citation: Zhang, Y.; Lu, C.; Zhang, J. Johanson in 1960 [1,2]. The three-dimensional structure of LF has been unveiled by high Lactoferrin and Its Detection resolution X-ray crystallographic analysis, and it consists of two homologous globular lobes Methods: A Review. -
IFM Innate Immunity Infographic
UNDERSTANDING INNATE IMMUNITY INTRODUCTION The immune system is comprised of two arms that work together to protect the body – the innate and adaptive immune systems. INNATE ADAPTIVE γδ T Cell Dendritic B Cell Cell Macrophage Antibodies Natural Killer Lymphocites Neutrophil T Cell CD4+ CD8+ T Cell T Cell TIME 6 hours 12 hours 1 week INNATE IMMUNITY ADAPTIVE IMMUNITY Innate immunity is the body’s first The adaptive, or acquired, immune line of immunological response system is activated when the innate and reacts quickly to anything that immune system is not able to fully should not be present. address a threat, but responses are slow, taking up to a week to fully respond. Pathogen evades the innate Dendritic immune system T Cell Cell Through antigen Pathogen presentation, the dendritic cell informs T cells of the pathogen, which informs Macrophage B cells B Cell B cells create antibodies against the pathogen Macrophages engulf and destroy Antibodies label invading pathogens pathogens for destruction Scientists estimate innate immunity comprises approximately: The adaptive immune system develops of the immune memory of pathogen exposures, so that 80% system B and T cells can respond quickly to eliminate repeat invaders. IMMUNE SYSTEM AND DISEASE If the immune system consistently under-responds or over-responds, serious diseases can result. CANCER INFLAMMATION Innate system is TOO ACTIVE Innate system NOT ACTIVE ENOUGH Cancers grow and spread when tumor Certain diseases trigger the innate cells evade detection by the immune immune system to unnecessarily system. The innate immune system is respond and cause excessive inflammation. responsible for detecting cancer cells and This type of chronic inflammation is signaling to the adaptive immune system associated with autoimmune and for the destruction of the cancer cells. -

Adoptive Cell Therapy Using Engineered Natural Killer Cells
Bone Marrow Transplantation (2019) 54:785–788 https://doi.org/10.1038/s41409-019-0601-6 REVIEW ARTICLE Adoptive cell therapy using engineered natural killer cells Katayoun Rezvani1 © The Author(s), under exclusive licence to Springer Nature Limited 2019 Abstract The generation of autologous T cells expressing a chimeric antigen receptor (CAR) have revolutionized the field of adoptive cellular therapy. CAR-T cells directed against CD19 have resulted in remarkable clinical responses in patients affected by B-lymphoid malignancies. However, the production of allogeneic CAR-T cells products remains expensive and clinically challenging. Moreover, the toxicity profile of CAR T-cells means that currently these life-saving treatments are only delivered in specialized centers. Therefore, efforts are underway to develop reliable off-the-shelf cellular products with acceptable safety profiles for the treatment of patients with cancer. Natural killer (NK) cells are innate effector lymphocytes with potent antitumor activity. The availability of NK cells from multiple sources and their proven safety profile in the allogeneic setting positions them as attractive contenders for cancer immunotherapy. In this review, we discuss advantages and potential drawbacks of using NK cells as a novel cellular therapy against hematologic malignancies, as well as strategies 1234567890();,: 1234567890();,: to further enhance their effector function. Introduction need for inpatient care may ultimately be economically unviable for many health care systems; (iii) the longer time Adoptive cell therapy has become a powerful treatment that is required to generate CAR T-cells may result in modality for advanced cancers refractory to conventional unavoidable delays in therapy, especially for patients with therapy. -

Adaptive Tdetect Fact Sheet for Recipient
FACT SHEET FOR RECIPIENTS Coronavirus Adaptive Biotechnologies Corporation September 2, 2021 Disease 2019 T-Detect COVID Test (COVID-19) You are being given this Fact Sheet because your coughing, difficulty breathing, etc.). A full list of sample is being tested or was tested for an adaptive T- symptoms of COVID-19 can be found at the following cell immune response to the virus that causes link: https://www.cdc.gov/coronavirus/2019- Coronavirus Disease 2019 (COVID-19) using the T- ncov/symptoms-testing/symptoms.html. Detect COVID Test. How are people tested for COVID-19? Two main kinds of tests are currently available for You should not interpret the results of this COVID-19: diagnostic tests and adaptive immune response tests. test to indicate the presence or absence of immunity or protection from COVID-19 • A diagnostic test tells you if you have a current infection. infection. • An adaptive immune response test tells you if you may have had a previous infection This Fact Sheet contains information to help you understand the risks and benefits of using this test to What is the T-Detect COVID Test? evaluate your adaptive immune response to SARS-CoV- This test is similar to an antibody test in that it measures 2, the virus that causes COVID-19. After reading this your adaptive immune response to SARS-CoV-2, the Fact Sheet, if you have questions or would like to virus that causes COVID-19. However in this case it discuss the information provided, please talk to your specifically measures your adaptive T-cell immune healthcare provider. -

B Cell Activation and Escape of Tolerance Checkpoints: Recent Insights from Studying Autoreactive B Cells
cells Review B Cell Activation and Escape of Tolerance Checkpoints: Recent Insights from Studying Autoreactive B Cells Carlo G. Bonasia 1 , Wayel H. Abdulahad 1,2 , Abraham Rutgers 1, Peter Heeringa 2 and Nicolaas A. Bos 1,* 1 Department of Rheumatology and Clinical Immunology, University Medical Center Groningen, University of Groningen, 9713 Groningen, GZ, The Netherlands; [email protected] (C.G.B.); [email protected] (W.H.A.); [email protected] (A.R.) 2 Department of Pathology and Medical Biology, University Medical Center Groningen, University of Groningen, 9713 Groningen, GZ, The Netherlands; [email protected] * Correspondence: [email protected] Abstract: Autoreactive B cells are key drivers of pathogenic processes in autoimmune diseases by the production of autoantibodies, secretion of cytokines, and presentation of autoantigens to T cells. However, the mechanisms that underlie the development of autoreactive B cells are not well understood. Here, we review recent studies leveraging novel techniques to identify and characterize (auto)antigen-specific B cells. The insights gained from such studies pertaining to the mechanisms involved in the escape of tolerance checkpoints and the activation of autoreactive B cells are discussed. Citation: Bonasia, C.G.; Abdulahad, W.H.; Rutgers, A.; Heeringa, P.; Bos, In addition, we briefly highlight potential therapeutic strategies to target and eliminate autoreactive N.A. B Cell Activation and Escape of B cells in autoimmune diseases. Tolerance Checkpoints: Recent Insights from Studying Autoreactive Keywords: autoimmune diseases; B cells; autoreactive B cells; tolerance B Cells. Cells 2021, 10, 1190. https:// doi.org/10.3390/cells10051190 Academic Editor: Juan Pablo de 1. -

Case of the Anti HIV-1 Antibody, B12
Spectrum of Somatic Hypermutations and Implication on Antibody Function: Case of the anti HIV-1 antibody, b12 Mesfin Mulugeta Gewe A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Washington 2015 Reading Committee: Roland Strong, Chair Nancy Maizels Jessica A. Hamerman Program Authorized to Offer Degree: Molecular and Cellular Biology i ii ©Copyright 2015 Mesfin Mulugeta Gewe iii University of Washington Abstract Spectrum of Somatic Hypermutations and Implication on Antibody Function: Case of the anti HIV-1 antibody, b12 Mesfin Mulugeta Gewe Chair of the Supervisory Committee: Roland Strong, Full Member Fred Hutchinson Cancer Research Center Sequence diversity, ability to evade immune detection and establishment of human immunodeficiency virus type 1 (HIV-1) latent reservoirs present a formidable challenge to the development of an HIV-1 vaccine. Structure based vaccine design stenciled on infection elicited broadly neutralizing antibodies (bNAbs) is a promising approach, in some measure to circumvent existing challenges. Understanding the antibody maturation process and importance of the high frequency mutations observed in anti-HIV-1 broadly neutralizing antibodies are imperative to the success of structure based vaccine immunogen design. Here we report a biochemical and structural characterization for the affinity maturation of infection elicited neutralizing antibodies IgG1 b12 (b12). We investigated the importance of affinity maturation and mutations accumulated therein in overall antibody function and their potential implications to vaccine development. Using a panel of point iv reversions, we examined relevance of individual amino acid mutations acquired during the affinity maturation process to deduce the role of somatic hypermutation in antibody function. -

Antimicrobial Glycoconjugate Vaccines: an Overview of Classic and Modern Approaches Cite This: Chem
Chem Soc Rev View Article Online TUTORIAL REVIEW View Journal | View Issue Antimicrobial glycoconjugate vaccines: an overview of classic and modern approaches Cite this: Chem. Soc. Rev., 2018, 47, 9015 for protein modification Francesco Berti * and Roberto Adamo * Glycoconjugate vaccines obtained by chemical linkage of a carbohydrate antigen to a protein are part of routine vaccinations in many countries. Licensed antimicrobial glycan–protein conjugate vaccines are obtained by random conjugation of native or sized polysaccharides to lysine, aspartic or glutamic amino acid residues that are generally abundantly exposed on the protein surface. In the last few years, the structural approaches for the definition of the polysaccharide portion (epitope) responsible for the immunological activity has shown potential to aid a deeper understanding of the mode of action of glycoconjugates and to lead to the rational design of more efficacious and safer vaccines. The combination of technologies to obtain more defined carbohydrate antigens of higher purity and novel approaches for Creative Commons Attribution-NonCommercial 3.0 Unported Licence. Received 12th June 2018 protein modification has a fundamental role. In particular, methods for site selective glycoconjugation like DOI: 10.1039/c8cs00495a chemical or enzymatic modification of specific amino acid residues, incorporation of unnatural amino acids and glycoengineering, are rapidly evolving. Here we discuss the state of the art of protein engineering with rsc.li/chem-soc-rev carbohydrates to obtain glycococonjugates vaccines and future perspectives. Key learning points (a) The covalent linkage with proteins is fundamental to transform carbohydrates, which are per se T-cell independent antigens, in immunogens capable of This article is licensed under a evoking a long-lasting T-cell memory response. -

Our Immune System (Children's Book)
OurOur ImmuneImmune SystemSystem A story for children with primary immunodeficiency diseases Written by IMMUNE DEFICIENCY Sara LeBien FOUNDATION A note from the author The purpose of this book is to help young children who are immune deficient to better understand their immune system. What is a “B-cell,” a “T-cell,” an “immunoglobulin” or “IgG”? They hear doctors use these words, but what do they mean? With cheerful illustrations, Our Immune System explains how a normal immune system works and what treatments may be necessary when the system is deficient. In this second edition, a description of a new treatment has been included. I hope this book will enable these children and their families to explore together the immune system, and that it will help alleviate any confusion or fears they may have. Sara LeBien This book contains general medical information which cannot be applied safely to any individual case. Medical knowledge and practice can change rapidly. Therefore, this book should not be used as a substitute for professional medical advice. SECOND EDITION COPYRIGHT 1990, 2007 IMMUNE DEFICIENCY FOUNDATION Copyright 2007 by Immune Deficiency Foundation, USA. Readers may redistribute this article to other individuals for non-commercial use, provided that the text, html codes, and this notice remain intact and unaltered in any way. Our Immune System may not be resold, reprinted or redistributed for compensation of any kind without prior written permission from Immune Deficiency Foundation. If you have any questions about permission, please contact: Immune Deficiency Foundation, 40 West Chesapeake Avenue, Suite 308, Towson, MD 21204, USA; or by telephone at 1-800-296-4433. -

Systematic Booster After Rabies Pre-Exposure Prophylaxis to Alleviate Rabies Antibody Monitoring in Individuals at Risk of Occupational Exposure
Article Systematic Booster after Rabies Pre-Exposure Prophylaxis to Alleviate Rabies Antibody Monitoring in Individuals at Risk of Occupational Exposure Perrine Parize 1,*, Jérémie Sommé 2 , Laura Schaeffer 3, Florence Ribadeau-Dumas 1, Sheherazade Benabdelkader 1, Agnès Durand 4, Arnaud Tarantola 1, Johann Cailhol 5, Julia Goesch 5, Lauriane Kergoat 1 , Anne-Sophie Le Guern 6, Marie-Laurence Mousel 2, Laurent Dacheux 1 , Paul-Henri Consigny 5, Arnaud Fontanet 3,7, Beata Francuz 2 and Hervé Bourhy 1 1 Institut Pasteur, Unit Lyssavirus Epidemiology and Neuropathology, National Reference Center for Rabies and WHO Collaborating Centre for Reference and Research on Rabies, 75015 Paris, France; fl[email protected] (F.R.-D.); [email protected] (S.B.); [email protected] (A.T.); [email protected] (L.K.); [email protected] (L.D.); [email protected] (H.B.) 2 Institut Pasteur, Occupational Health Department, 75015 Paris, France; [email protected] (J.S.); [email protected] (M.-L.M.); [email protected] (B.F.) 3 Institut Pasteur, Emerging Diseases Epidemiology Unit, Centre for Global Health Research and Education, 75015 Paris, France; [email protected] (L.S.); [email protected] (A.F.) 4 Laboratoire Cerballiance, 75017 Paris, France; [email protected] 5 Citation: Parize, P.; Sommé, J.; Institut Pasteur, Centre Médical, Centre d’Infectiologie Necker-Pasteur, 75015 Paris, France; Schaeffer, L.; Ribadeau-Dumas, F.; [email protected] (J.C.); [email protected] (J.G.); [email protected] (P.-H.C.) 6 Benabdelkader, S.; Durand, A.; Institut Pasteur, Laboratory of the Medical Center, 75015 Paris, France; [email protected] 7 Conservatoire National des Arts et Métiers, 75003 Paris, France Tarantola, A.; Cailhol, J.; Goesch, J.; * Correspondence: [email protected]; Tel.: +33-140-613-436 Kergoat, L.; et al. -
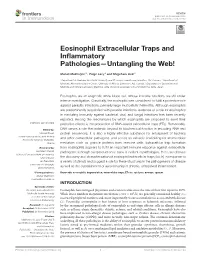
Eosinophil Extracellular Traps and Inflammatory Pathologies—Untangling the Web!
REVIEW published: 26 November 2018 doi: 10.3389/fimmu.2018.02763 Eosinophil Extracellular Traps and Inflammatory Pathologies—Untangling the Web! Manali Mukherjee 1*, Paige Lacy 2 and Shigeharu Ueki 3 1 Department of Medicine, McMaster University and St Joseph’s Healthcare, Hamilton, ON, Canada, 2 Department of Medicine, Alberta Respiratory Centre, University of Alberta, Edmonton, AB, Canada, 3 Department of General Internal Medicine and Clinical Laboratory Medicine, Akita University Graduate School of Medicine, Akita, Japan Eosinophils are an enigmatic white blood cell, whose immune functions are still under intense investigation. Classically, the eosinophil was considered to fulfill a protective role against parasitic infections, primarily large multicellular helminths. Although eosinophils are predominantly associated with parasite infections, evidence of a role for eosinophils in mediating immunity against bacterial, viral, and fungal infections has been recently reported. Among the mechanisms by which eosinophils are proposed to exert their protective effects is the production of DNA-based extracellular traps (ETs). Remarkably, Edited by: DNA serves a role that extends beyond its biochemical function in encoding RNA and Moncef Zouali, protein sequences; it is also a highly effective substance for entrapment of bacteria Institut National de la Santé et de la and other extracellular pathogens, and serves as valuable scaffolding for antimicrobial Recherche Médicale (INSERM), France mediators such as granule proteins from immune cells. Extracellular -

Monoclonal Antibody Playbook
Federal Response to COVID-19: Monoclonal Antibody Clinical Implementation Guide Outpatient administration guide for healthcare providers 2 SEPTEMBER 2021 1 Introduction to COVID-19 Monoclonal Antibody Therapy 2 Overview of Emergency Use Authorizations 3 Site and Patient Logistics Site preparation Patient pathways to monoclonal administration 4 Team Roles and Responsibilities Leadership Administrative Clinical Table of 5 Monoclonal Antibody Indications and Administration Indications Contents Preparation Administration Response to adverse events 6 Supplies and Resources Infrastructure Administrative Patient Intake Administration 7 Examples: Sites of Administration and Staffing Patterns 8 Additional Resources 1 1. Introduction to Monoclonal Therapy 2 As of 08/13/21 Summary of COVID-19 Therapeutics 1 • No Illness . Health, no infections • Exposed Asymptomatic Infected . Scope of this Implementation Guide . Not hospitalized, no limitations . Monoclonal Antibodies for post-exposure prophylaxis (Casirivimab + Imdevimab (RGN)) – EUA Issued. • Early Symptomatic . Scope of this Implementation Guide . Not hospitalized, with limitations . Monoclonal Antibodies for treatment (EUA issued): Bamlanivimab + Etesevimab1 (Lilly) Casirivimab + Imdevimab (RGN) Sotrovimab (GSK/Vir) • Hospital Adminission. Treated with Remdesivir (FDA Approved) or Tocilizumab (EUA Issued) . Hospitalized, no acute medical problems . Hospitalized, not on oxygen . Hospitlaized, on oxygen • ICU Admission . Hospitalized, high flow oxygen, non-invasive ventilation -
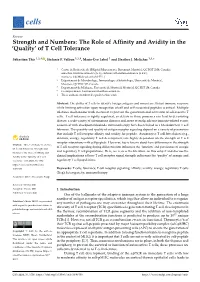
Of T Cell Tolerance
cells Review Strength and Numbers: The Role of Affinity and Avidity in the ‘Quality’ of T Cell Tolerance Sébastien This 1,2,† , Stefanie F. Valbon 1,2,†, Marie-Ève Lebel 1 and Heather J. Melichar 1,3,* 1 Centre de Recherche de l’Hôpital Maisonneuve-Rosemont, Montréal, QC H1T 2M4, Canada; [email protected] (S.T.); [email protected] (S.F.V.); [email protected] (M.-È.L.) 2 Département de Microbiologie, Immunologie et Infectiologie, Université de Montréal, Montréal, QC H3C 3J7, Canada 3 Département de Médecine, Université de Montréal, Montréal, QC H3T 1J4, Canada * Correspondence: [email protected] † These authors contributed equally to this work. Abstract: The ability of T cells to identify foreign antigens and mount an efficient immune response while limiting activation upon recognition of self and self-associated peptides is critical. Multiple tolerance mechanisms work in concert to prevent the generation and activation of self-reactive T cells. T cell tolerance is tightly regulated, as defects in these processes can lead to devastating disease; a wide variety of autoimmune diseases and, more recently, adverse immune-related events associated with checkpoint blockade immunotherapy have been linked to a breakdown in T cell tolerance. The quantity and quality of antigen receptor signaling depend on a variety of parameters that include T cell receptor affinity and avidity for peptide. Autoreactive T cell fate choices (e.g., deletion, anergy, regulatory T cell development) are highly dependent on the strength of T cell receptor interactions with self-peptide. However, less is known about how differences in the strength Citation: This, S.; Valbon, S.F.; Lebel, of T cell receptor signaling during differentiation influences the ‘function’ and persistence of anergic M.-È.; Melichar, H.J.