IOWA HEALTH SYSTEM PHARMACY SERVICE PATIENT INFORMATION FORM (Note this is a 2 sided form)
EMPLOYEE INFORMATION Please fill in form and print out or legibly print all information. If both you and your spouse are employed by Iowa Health System, please fill in information of the spouse who carries the insurance and from whose paycheck the co-pay will be deducted. EMPLOYEE LAST NAME: FIRST: INITIAL: ADDRESS: CITY, STATE, ZIP: HOME PHONE: WORK PHONE:
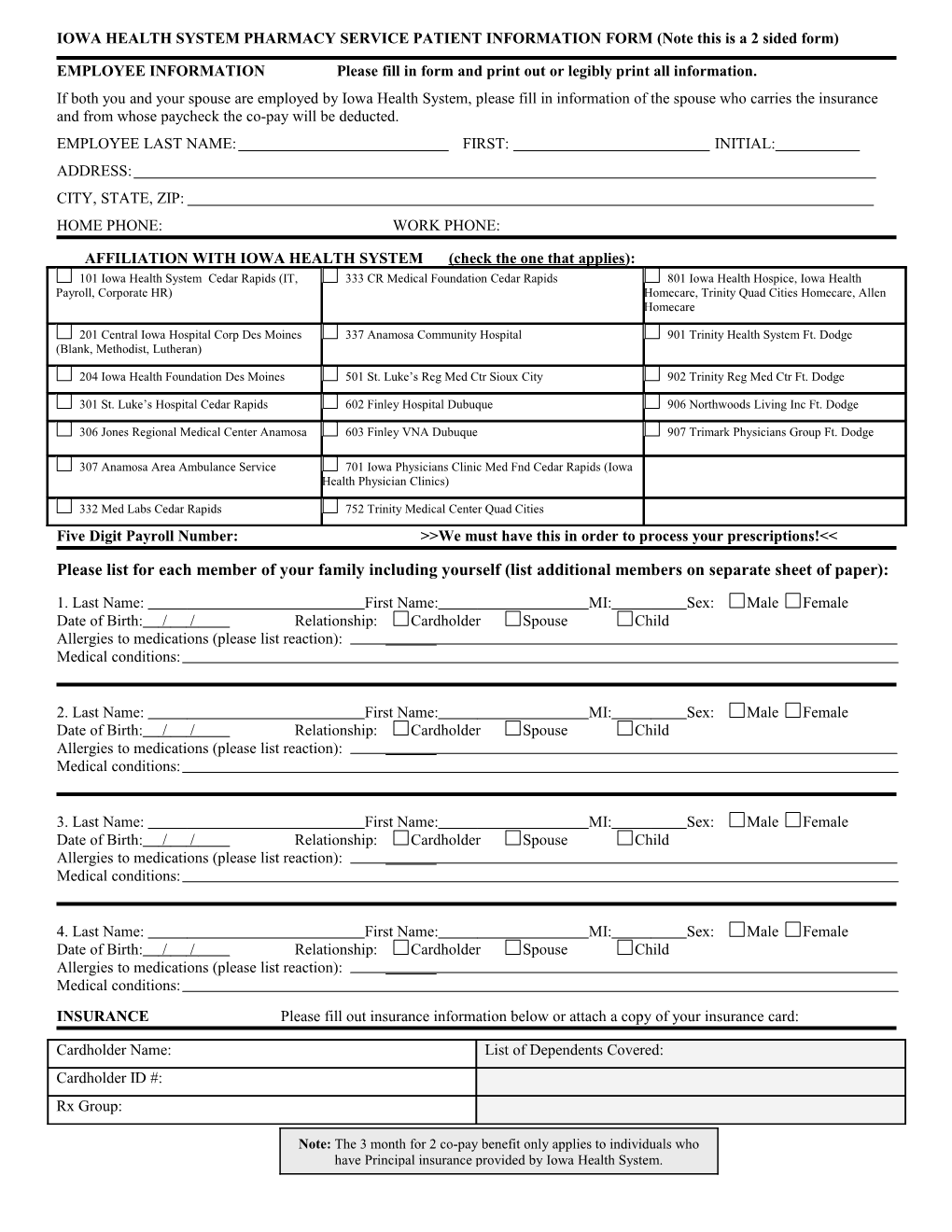
AFFILIATION WITH IOWA HEALTH SYSTEM (check the one that applies): 101 Iowa Health System Cedar Rapids (IT, 333 CR Medical Foundation Cedar Rapids 801 Iowa Health Hospice, Iowa Health Payroll, Corporate HR) Homecare, Trinity Quad Cities Homecare, Allen Homecare
201 Central Iowa Hospital Corp Des Moines 337 Anamosa Community Hospital 901 Trinity Health System Ft. Dodge (Blank, Methodist, Lutheran)
204 Iowa Health Foundation Des Moines 501 St. Luke’s Reg Med Ctr Sioux City 902 Trinity Reg Med Ctr Ft. Dodge
301 St. Luke’s Hospital Cedar Rapids 602 Finley Hospital Dubuque 906 Northwoods Living Inc Ft. Dodge
306 Jones Regional Medical Center Anamosa 603 Finley VNA Dubuque 907 Trimark Physicians Group Ft. Dodge
307 Anamosa Area Ambulance Service 701 Iowa Physicians Clinic Med Fnd Cedar Rapids (Iowa Health Physician Clinics)
332 Med Labs Cedar Rapids 752 Trinity Medical Center Quad Cities Five Digit Payroll Number: >>We must have this in order to process your prescriptions!<<
Please list for each member of your family including yourself (list additional members on separate sheet of paper):
1. Last Name: First Name: MI: Sex: Male Female Date of Birth: / / Relationship: Cardholder Spouse Child Allergies to medications (please list reaction): Medical conditions:
2. Last Name: First Name: MI: Sex: Male Female Date of Birth: / / Relationship: Cardholder Spouse Child Allergies to medications (please list reaction): Medical conditions:
3. Last Name: First Name: MI: Sex: Male Female Date of Birth: / / Relationship: Cardholder Spouse Child Allergies to medications (please list reaction): Medical conditions:
4. Last Name: First Name: MI: Sex: Male Female Date of Birth: / / Relationship: Cardholder Spouse Child Allergies to medications (please list reaction): Medical conditions: INSURANCE Please fill out insurance information below or attach a copy of your insurance card:
Cardholder Name: List of Dependents Covered: Cardholder ID #: Rx Group:
Note: The 3 month for 2 co-pay benefit only applies to individuals who have Principal insurance provided by Iowa Health System. Prescription Bottle Caps: A child resistant cap is included with every order. Check here if you would also like an easy open cap and sign here: ______Generic medications: We want to provide you with high quality medications at the best possible price. In order to do this, if a generic medication is available and is authorized by your physician, the generic version of your medication will be dispensed. If you choose not to have a generic medication, this may result in a higher co-pay and a delay in delivery so that the medication can be ordered. Please indicate when ordering if the brand name medication is necessary. Medications with dispensing limits: A small list of medications has a quantity limit per 30 days. These quantity limits will continue to apply but you are now able to purchase these medications in a 90-day supply for 2 co-pays. Example: Imitrex has a quantity limit of per 9 per 30 days, you now are able to obtain 27 per 90 days for a 2 co-pay price. For a complete listing, visit our website at www.ihsmeds.org
RECEIVING PRESCRIPTION:
Would you like to receive your prescriptions? Mail or Pick Up
Mail completed form to: Iowa Health System Pharmacy P.O Box 1847 Cedar Rapids, Iowa 52406-1847 or fax completed form to: 1-319-368-5619