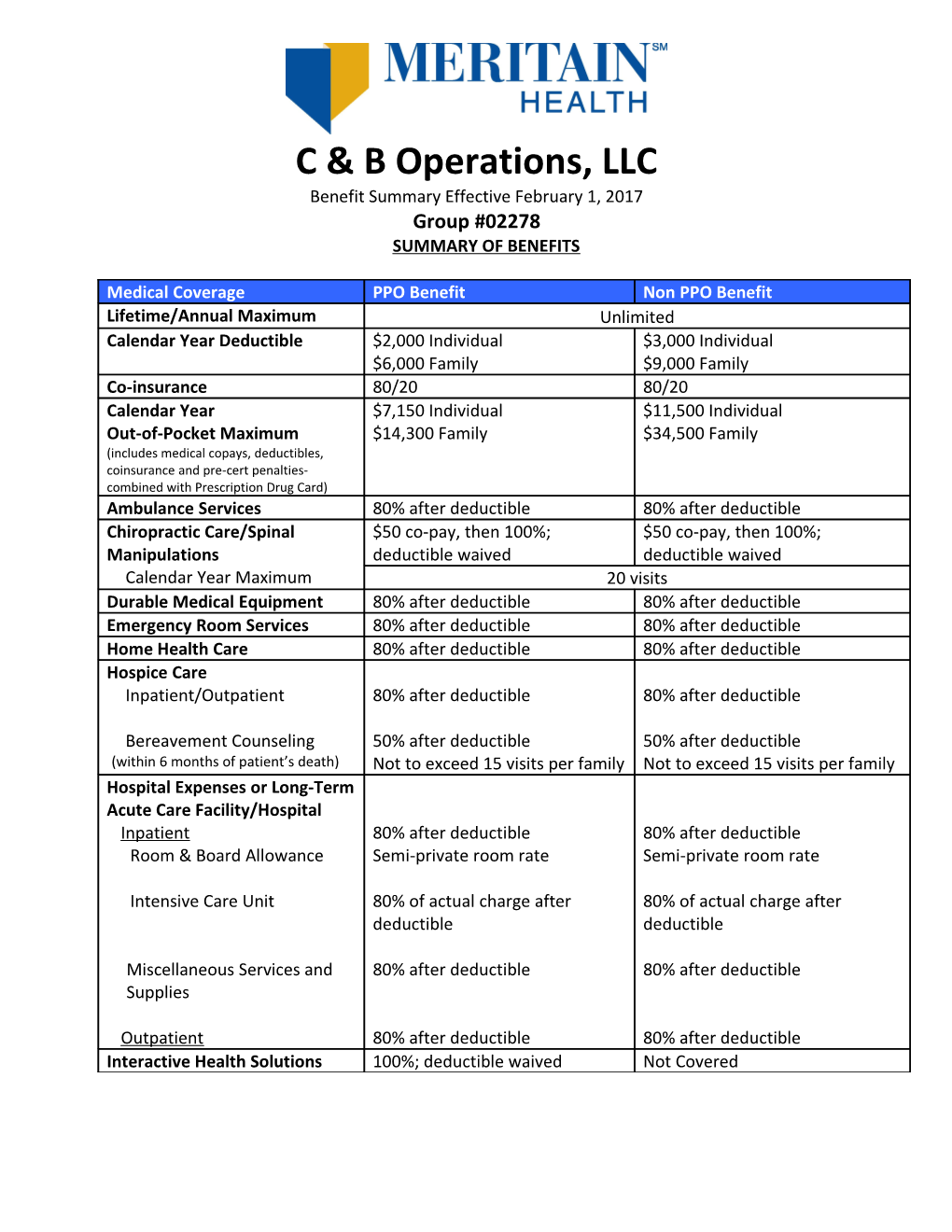
C & B Operations, LLC Benefit Summary Effective February 1, 2017 Group #02278 SUMMARY OF BENEFITS
Medical Coverage PPO Benefit Non PPO Benefit Lifetime/Annual Maximum Unlimited Calendar Year Deductible $2,000 Individual $3,000 Individual $6,000 Family $9,000 Family Co-insurance 80/20 80/20 Calendar Year $7,150 Individual $11,500 Individual Out-of-Pocket Maximum $14,300 Family $34,500 Family (includes medical copays, deductibles, coinsurance and pre-cert penalties- combined with Prescription Drug Card) Ambulance Services 80% after deductible 80% after deductible Chiropractic Care/Spinal $50 co-pay, then 100%; $50 co-pay, then 100%; Manipulations deductible waived deductible waived Calendar Year Maximum 20 visits Durable Medical Equipment 80% after deductible 80% after deductible Emergency Room Services 80% after deductible 80% after deductible Home Health Care 80% after deductible 80% after deductible Hospice Care Inpatient/Outpatient 80% after deductible 80% after deductible
Bereavement Counseling 50% after deductible 50% after deductible (within 6 months of patient’s death) Not to exceed 15 visits per family Not to exceed 15 visits per family Hospital Expenses or Long-Term Acute Care Facility/Hospital Inpatient 80% after deductible 80% after deductible Room & Board Allowance Semi-private room rate Semi-private room rate
Intensive Care Unit 80% of actual charge after 80% of actual charge after deductible deductible
Miscellaneous Services and 80% after deductible 80% after deductible Supplies
Outpatient 80% after deductible 80% after deductible Interactive Health Solutions 100%; deductible waived Not Covered Medical Coverage PPO Benefit Non PPO Benefit Mental Disorders/Substance Use Disorders Inpatient 80% after deductible 80% after deductible Semi-private room rate Semi-private room rate Outpatient Office Visits $50 co-pay, then 100%; $50 co-pay, then 100%; deductible waived deductible waived
All Other Outpatient Services 80% after deductible 80% after deductible
Emergency Care 80% after deductible 80% after PPO deductible, subject (ambulance and emergency room) to PPO coinsurance Outpatient Therapies $50 co-pay, then 100%; $50 co-pay, then 100%; (physical, speech, deductible waived deductible waived occupational) 25 visits Combined Calendar Year Maximum Physician’s Services Inpatient and Outpatient Services 80% after deductible 80% after deductible
Office Surgery 80% after deductible 80% after deductible
Office Visits $50 co-pay, then 100%; $50 co-pay, then 100%; deductible waived deductible waived Pregnancy (professional fees) Preventive prenatal & breastfeeding support (other than lactation consultations 100%; deductible waived 80% after deductible
Lactation Consultations 100%; deductible waived 100%; deductible waived
All other prenatal & postnatal 80% after deductible 80% after deductible care
Delivery 80% after deductible 80% after deductible Preventive Care 100%; deductible waived 80% after deductible (includes office visit and any other eligible item or service received at the same time as any preventive service benefit, whether billed at the same time or separately) Routine Mammograms $50 co-pay, then 100%; $50 co-pay, then 100%; (coverage otherwise included for coverage under the Preventive Services section of deductible waived deductible waived the Plan)is in addition to and to the extent they are not Medical Coverage PPO Benefit Non PPO Benefit Scalp Hair Prosthesis 80% after deductible 80% after deductible Lifetime Maximum Benefit 1 wig Skilled Nursing Facility and 80% after deductible 80% after deductible Rehabilitation Facility
Calendar Year Maximum 60 days Urgent Care Facility 80% after deductible 80% after deductible All Other Eligible Expenses 80% after deductible 80% after deductible
Prescription Drug Coverage
Calendar Year Out of Pocket Limit (includes Copays-combined with major medical) Individual $7,150 Family $14,300
Prescription Drugs Retail (34 or 90 day supply) Generic $35 co-pay, then 100% Preferred Brand Name $100 co-pay, then 100% Non-Preferred Brand Name $200 co-pay, then 100% Specialty $400 co-pay, then 100% Preventive Generic 100%; no co-pay
Mail Order (90 day supply) Generic $35 co-pay, then 100% Preferred Brand Name $100 co-pay, then 100% Non-Preferred Brand Name $200 co-pay, then 100% Specialty $400 co-pay, then 100% Preventive Generic 100%; no co-pay
Dental Coverage Calendar Year Deductible $75 Individual $225 Family Class A Expenses (Preventive Services) 100%; deductible waived Class B Expenses (Basic Services) 80% after deductible Class C Expenses (Major Services) 50% after deductible Calendar Year Maximum $1,500 (Classes A, B and C Expenses Combined per Person) 50% after deductible Orthodontia Treatment (For dependents under age 19) $2,000 Lifetime Orthodontia Maximum C&B Operations, LLC Group #02278
MERITAIN HEALTH: Meritain Health administers your health plan benefits on behalf of C&B Operations, LLC, in accordance with the C&B Operations, LLC Employee Plan Document.
Meritain Health Benefit/Claim Customer Service 1-800-925-2272: A Meritain Health Customer Service Representative will be able to assist you with benefit/claims questions.
Meritain Health 24 Hour Automated Customer Service Info Line 1-800-566-9311: An Interactive Voice Response System provides rapid access to benefits, claim status and eligibility information. You can receive a fax verification of eligibility, a status of submitted claims, faxed copy of an Explanation of Benefits, request a new I.D. card, request a HIPAA Certification of Coverage and more features are being added. www.myMERITAIN.com: Corporate information is available through the Meritain Health website, as well as helpful links and other useful information.
PRE-CERTIFICATION
Meritain Health Medical Management: Meritain Health Medical Management is Meritain Health’s in-house utilization review service.
Meritain Health Medical Management must pre-authorize non-emergency Inpatient Hospital admissions 48 hours prior to admission. Meritain Health Medical Management must also be notified of all emergency Inpatient Hospital admissions within 48 hours of admission. (If emergency admission occurs on a weekend or holiday, notification can be extended to the first business day following the emergency admission.) If these procedures are not followed, you may be financially responsible for any medically unnecessary services.
Pre-Certification is required on the below items: Chemotherapy - all settings including services rendered in a Physician's office. Dialysis - all settings including services rendered in a Physician's office. Durable Medical Equipment (other than breast pumps covered as a preventive service) - in excess of $1,500. Home health care, including IV home infusion therapy. Hospice care. Imaging, limited to the following: CT/MRA/MRI/PET scans, scintimammography, capsule endoscopy and U.S. bone density (heel). Inpatient admissions, including inpatient admissions to a Skilled Nursing Facility, Extended Care Facility, Rehabilitation Facility, and inpatient admissions due to a Mental Disorder or Substance Use Disorder. Outpatient Surgical procedures, excluding Surgery rendered in a Physician's office. Radiation - all settings including services rendered in a Physician's office. Transplants, including transportation and lodging.
Meritain Health Medical Management 1-800-242-1199 Express Scripts: Express Scripts is the provider of prescription services for C&B Operations, LLC.
Express Scripts Customer Service 877-468-6592: They will be able to answer any questions you may have regarding your prescriptions. They are also available to assist a pharmacist with any questions, or concerns they might have. If you must pick up a prescription before your card is available, present the following information to the pharmacist: Bin #003858 Carrier/Group/PCN-A4, Group #PRXS, your name and your group number.
For Mail Order Prescriptions: Express Script Order Service handles all the mail order prescriptions for Scrip World. For information and access please call: 800-810-6549.
www.express-scripts.com: This website is extremely useful and provides information including, but not limited to specific prescription drugs, mail order service and access to the Scrip World Prescription Drug Formulary.
When an eligible prescription is filled at a participating Express Scripts pharmacy, you will only be responsible to pay the applicable co-pay and it will not be necessary to file a claim with Express Scripts. If you paid for a prescription in full and need a reimbursement send the prescription receipt to:
Express Scripts 10150 S. Centennial Parkway Suite 450 Sandy, UT 84070
For Medical Plan participating providers:
PPO Network Name Aetna
Send Claims to: Meritain Health, Inc. P.O. Box 853921 Richardson, TX 75085-3921 To identify an Aetna provider, call: 1-800-343-3140 Or go to: www.myMERITAIN.com
To expedite payment, please identify your Group Number and your Name on all claims submitted.
This is only a brief summary of the benefits available. Some restrictions may apply. For more specific information about the coverage details including limitations, exclusions and other requirements, please refer to the actual Summary Plan Description.