«Title» «Forename» «Surname» DOB: «Date_of_birth» NHS no: «NHS_number» «Sender_organisation_name»
SUSPECTED UROLOGICAL CANCER REFERRAL FORM Press the
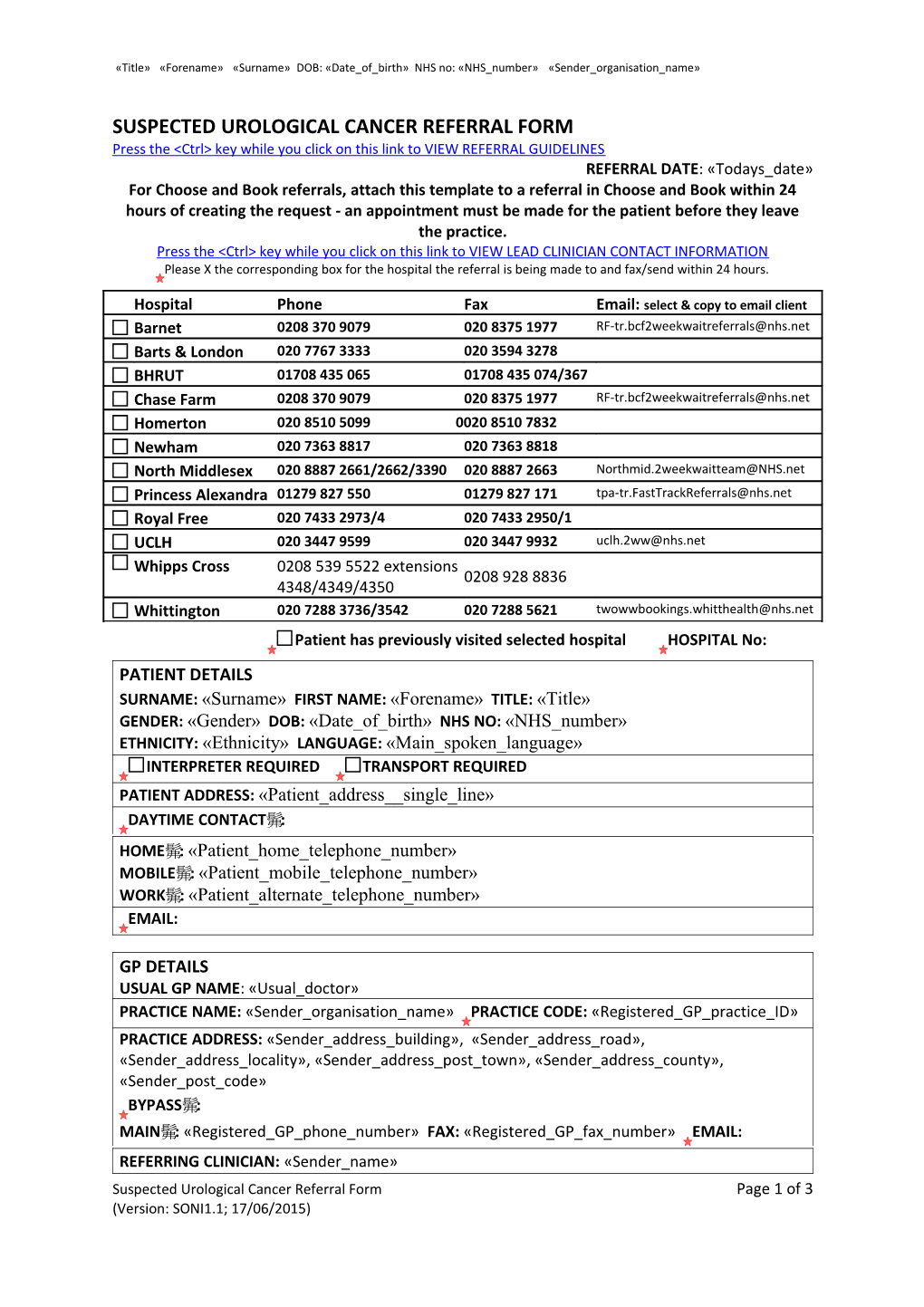
Hospital Phone Fax Email: select & copy to email client Barnet 0208 370 9079 020 8375 1977 [email protected] Barts & London 020 7767 3333 020 3594 3278 BHRUT 01708 435 065 01708 435 074/367 Chase Farm 0208 370 9079 020 8375 1977 [email protected] Homerton 020 8510 5099 0020 8510 7832 Newham 020 7363 8817 020 7363 8818 North Middlesex 020 8887 2661/2662/3390 020 8887 2663 [email protected] Princess Alexandra 01279 827 550 01279 827 171 [email protected] Royal Free 020 7433 2973/4 020 7433 2950/1 UCLH 020 3447 9599 020 3447 9932 [email protected] Whipps Cross 0208 539 5522 extensions 0208 928 8836 4348/4349/4350 Whittington 020 7288 3736/3542 020 7288 5621 [email protected] Patient has previously visited selected hospital HOSPITAL No: PATIENT DETAILS SURNAME: «Surname» FIRST NAME: «Forename» TITLE: «Title» GENDER: «Gender» DOB: «Date_of_birth» NHS NO: «NHS_number» ETHNICITY: «Ethnicity» LANGUAGE: «Main_spoken_language» INTERPRETER REQUIRED TRANSPORT REQUIRED PATIENT ADDRESS: «Patient_address__single_line» DAYTIME CONTACT: HOME: «Patient_home_telephone_number» MOBILE: «Patient_mobile_telephone_number» WORK: «Patient_alternate_telephone_number» EMAIL:
GP DETAILS USUAL GP NAME: «Usual_doctor» PRACTICE NAME: «Sender_organisation_name» PRACTICE CODE: «Registered_GP_practice_ID» PRACTICE ADDRESS: «Sender_address_building», «Sender_address_road», «Sender_address_locality», «Sender_address_post_town», «Sender_address_county», «Sender_post_code» BYPASS: MAIN: «Registered_GP_phone_number» FAX: «Registered_GP_fax_number» EMAIL: REFERRING CLINICIAN: «Sender_name» Suspected Urological Cancer Referral Form Page 1 of 3 (Version: SONI1.1; 17/06/2015) DOB: NHS no:
CLINICAL DETAILS
PROSTATE Clinically malignant prostate on DRE* *PSA should be done and result should Unexplained LUTS and/or bony pain/weight loss* accompany referral PSA as compared to age specific ranges Press the
TESTICULAR Abnormal mass/swelling within the body of the testes on examination or imaging Abnormal investigations; alpha-fetoprotein, beta HCG Worried patient with history of undescended testicle
PENILE Abnormal Lesion on the Penis (Premalignant disease or carcinoma in situ) Palpable unexplained inguinal lymph node with penile lesion Clinical features of penile cancer Rectal examination findings (if performed): Any other relevant symptoms and signs not covered by the guidelines: Family History of cancer including age at diagnosis:
I confirm that I have discussed the possibility with the patient that the diagnosis may be cancer I confirm that I have explained the two week wait appointment process to the patient
Please hand the patient a copy of the URGENT REFERRALS PATIENT INFORMATION LEAFLET Press the
This form displays all recent pathology results. However, laboratory departments may code some results in a way which might not be picked up by this form. So please review them, add any you feel are relevant and delete any which are not. Depending on the clinical context you may wish to include: U&E, eGFR, MSU, PSA, alpha-fetoprotein, beta HCG IMAGING STUDIES (Please include date and location)
RECENT PATHOLOGY RESULTS «Recent_Pathology»
Page 2 of 3 (Version: SONI1.1; 17/06/2015) DOB: NHS no:
PROBLEMS «Summary»
ALLERGIES «Allergies»
MEDICATION «Current_Repeat_Templates»
Page 3 of 3 (Version: SONI1.1; 17/06/2015)