Table of Contents
Topic Page Topic Page
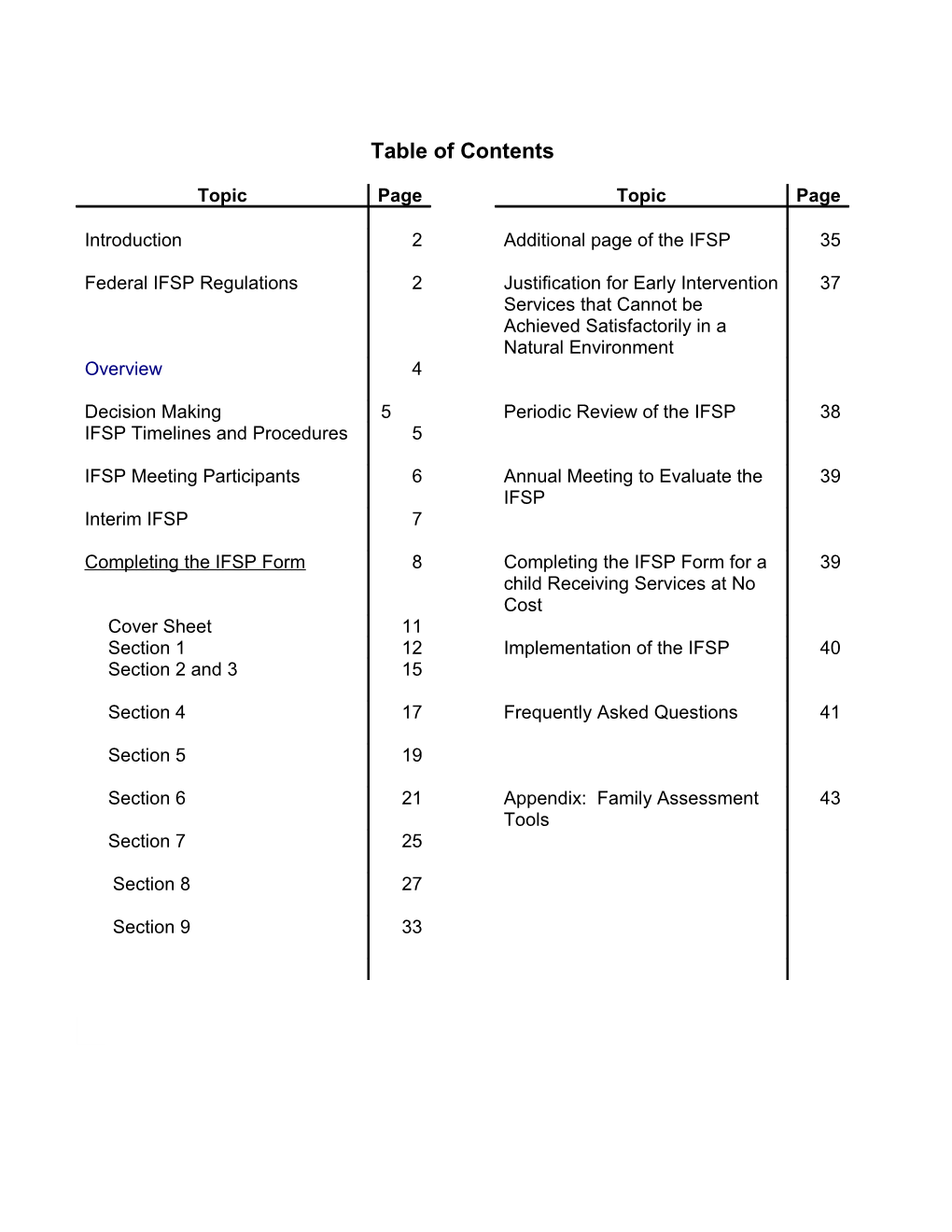
Introduction 2 Additional page of the IFSP 35
Federal IFSP Regulations 2 Justification for Early Intervention 37 Services that Cannot be Achieved Satisfactorily in a Natural Environment Overview 4
Decision Making 5 Periodic Review of the IFSP 38 IFSP Timelines and Procedures 5
IFSP Meeting Participants 6 Annual Meeting to Evaluate the 39 IFSP Interim IFSP 7
Completing the IFSP Form 8 Completing the IFSP Form for a 39 child Receiving Services at No Cost Cover Sheet 11 Section 1 12 Implementation of the IFSP 40 Section 2 and 3 15
Section 4 17 Frequently Asked Questions 41
Section 5 19
Section 6 21 Appendix: Family Assessment 43 Tools Section 7 25
Section 8 27
Section 9 33
2
Introduction
This handbook is a guide to working with the Individualized Family Service Plan (IFSP) Form 3-1, revised July 1, 2013, and used statewide in the Connecticut Birth to Three System by all programs.
When reading this handbook it is important to remember that the Connecticut IFSP document is many things to many people: It is most importantly a document for the family that describes what outcomes they can expect for their child and family and what services and supports they will receive to achieve those outcomes. It is a flexible and individualized plan for each child and family. It is a legal document. Its form and contents must comply with federal Part C of IDEA and state Birth to Three laws and regulations. It is a listing of recommendations for services and supports for the child’s physician to review. It provides information to school districts and other community programs during the process of transition. The information contained in the IFSP document supports third party billing of private insurance and Medicaid. The information from the IFSP is entered into the Birth to Three data system and is used in part to determine a Birth to Three program’s compliance with state and federal requirements, and the system’s quality assurance measures.
Federal IFSP Regulations
The Connecticut IFSP was designed to be in compliance with IDEA 2004 and Section 303.344 of the IDEA regulations as amended in 2011. Service coordinators should be familiar with the requirements of IDEA and the regulations so they understand the intent of each section of the form and the IFSP process. § 303.344 Content of an IFSP. (a) Information about the child’s status. The IFSP must include a statement of the infant or toddler with a disability’s present levels of physical development (including vision, hearing, and health status), cognitive development, communication development, social or emotional development, and adaptive development based on the information from that child’s evaluation and assessments conducted under § 303.321. (b) Family information. With the concurrence of the family, the IFSP must include a statement of the family’s resources, priorities, and concerns related to enhancing the development of the child as identified through the assessment of the family under § 303.321(c)(2). (c) Results or outcomes. The IFSP must include a statement of the measurable results or measurable outcomes expected to be achieved for the child (including pre-literacy and language skills, as developmentally appropriate for the child) and family, and the criteria, procedures, and timelines used to determine— (1) The degree to which progress toward achieving the results or outcomes identified in the IFSP is being made; and (2) Whether modifications or revisions of the expected results or outcomes, or early intervention services identified in the IFSP are necessary. 3
(d) Early intervention services. (1) The IFSP must include a statement of the specific early intervention services, based on peer-reviewed research (to the extent practicable), that are necessary to meet the unique needs of the child and the family to achieve the results or outcomes identified in paragraph (c) of this section, including— (i) The length, duration, frequency, intensity, and method of delivering the early intervention services; (ii)(A) A statement that each early intervention service is provided in the natural environment for that child or service to the maximum extent appropriate, consistent with §§ 303.13(a)(8), 303.26 and 303.126, or, subject to paragraph (d)(1)(ii)(B) of this section, a justification as to why an early intervention service will not be provided in the natural environment. (B) The determination of the appropriate setting for providing early intervention services to an infant or toddler with a disability, including any justification for not providing a particular early intervention service in the natural environment for that infant or toddler with a disability and service, must be— (1) Made by the IFSP Team (which includes the parent and other team members); (2) Consistent with the provisions in §§ 303.13(a)(8), 303.26, and 303.126; and (3) Based on the child’s outcomes that are identified by the IFSP Team in paragraph (c) of this section; (iii) The location of the early intervention services; and (iv) The payment arrangements, if any. (2) As used in paragraph (d)(1)(i) of this section— (i) Frequency and intensity mean the number of days or sessions that a service will be provided, and whether the service is provided on an individual or group basis; (ii) Method means how a service is provided; (iii) Length means the length of time the service is provided during each session of that service (such as an hour or other specified time period); and (iv) Duration means projecting when a given service will no longer be provided (such as when the child is expected to achieve the results or outcomes in his or her IFSP). (3) As used in paragraph (d)(1)(iii) of this section, location means the actual place or places where a service will be provided. (4) For children who are at least three years of age, the IFSP must include an educational component that promotes school readiness and incorporates preliteracy, language, and numeracy skills. (e) Other services. To the extent appropriate, the IFSP also must— (1) Identify medical and other services that the child or family needs or is receiving through other sources, but that are neither required nor funded under this part; and (2) If those services are not currently being provided, include a description of the steps the service coordinator or family may take to assist the child and family in securing those other services. (f) Dates and duration of services. The IFSP must include— (1) The projected date for the initiation of each early intervention service in paragraph (d)(1) of this section, which date must be as soon as possible after the parent consents to the service, as required in §§ 303.342(e) and 303.420(a)(3); and (2) The anticipated duration of each service. (g) Service coordinator. (1) The IFSP must include the name of the service coordinator from the profession most relevant to the child’s or family’s needs (or who is otherwise qualified to carry out all applicable responsibilities under this part), who will be responsible for
4
implementing the early intervention services identified in a child’s IFSP, including transition services, and coordination with other agencies and persons. (2) In meeting the requirements in paragraph (g)(1) of this section, the term ‘‘profession’’ includes ‘‘service coordination.’’ (h) Transition from Part C services. (1) The IFSP must include the steps and services to be taken to support the smooth transition of the child, in accordance with §§ 303.209 and 303.211(b)(6), from part C services to— (i) Preschool services under part B of the Act, to the extent that those services are appropriate; (ii) Part C services under § 303.211; or (iii) Other appropriate services. (2) The steps required in paragraph (h)(1) of this section must include— (i) Discussions with, and training of, parents, as appropriate, regarding future placements and other matters related to the child’s transition; (ii) Procedures to prepare the child for changes in service delivery, including steps to help the child adjust to, and function in, a new setting; (iii) Confirmation that child find information about the child has been transmitted to the LEA or other relevant agency, in accordance with § 303.209(b) (and any policy adopted by the State under § 303.401(e)) and, with parental consent if required under § 303.414, transmission of additional information needed by the LEA to ensure continuity of services from the part C program to the part B program, including a copy of the most recent evaluation and assessments of the child and the family and most recent IFSP developed in accordance with §§ 303.340 through 303.345; and (iv) Identification of transition services and other activities that the IFSP Team determines are necessary to support the transition of the child. (Authority: 20 U.S.C. 1435(a)(10) (B), 1435(a)(16), 1436(a)(3), 1436(d), 1437(a)(9)– (10), 1440)
Overview
The individualized family service planning process is used to develop a plan for appropriate early intervention services for an infant or toddler with disabilities and his or her family. The mission of the Connecticut Birth to Three System is to strengthen the capacity of Connecticut’s families to meet the developmental and health-related needs of their infants and toddlers who have delays or disabilities. The system will ensure that all families have equal access to a coordinated program of comprehensive services and supports that: Foster collaborative partnerships Are family centered Occur in natural environments Recognize current best practices in early intervention Are built upon mutual respect and choice
The components of the mission are embedded into the IFSP process and into the way early intervention services are delivered in Connecticut. In accordance with best practice, a transdisciplinary approach to service delivery is used for all early intervention and support services. This means 1) the parent along with providers from two or more disciplines teach, learn, and work together across traditional discipline specific or professional boundaries to meet the family’s goals. 2) One team member is designated as the team lead, primary interventionist, and service coordinator for the family. Whenever possible, this person should be from the profession most relevant to the family’s and or child’s needs. 3) Other team members provide direct services to the family or act as a consultant/coach to the primary provider. 4) All team members respect the 5 diversity of families with whom they work. 5) Services are delivered in natural environments and embedded into the routines and activities of the family, and, 6) Written materials provided to the family (including the IFSP) should be free of professional jargon.
Decision Making
Professionals and parents must work together to develop the IFSP. Throughout the IFSP process, family members and service providers work as a team to identify the family’s concerns and priorities. This is facilitated by reviewing the results of current assessments and completing the pages of the IFSP that identify who and what are important to the family during their daily routines. Then, the team reaches agreement on the strategies, activities, and services that will result in achievement of the outcomes. For this reason all Birth to Three staff members must speak for their agency when identifying the services and supports to be provided. They cannot defer to someone outside the team to decide if the services identified are appropriate. To arrive at good decisions regarding the IFSP, parents and professionals should trust and respect each other’s expertise and roles.
IFSP Timelines and Procedures
Procedures for IFSP development, review, and evaluation (34 CFR sec. 303.342-343) are:
A meeting to develop the initial IFSP must be held within 45 calendar days of the child’s referral to the Birth to Three System (i.e. the call to Child Development Infoline).
This meeting must be conducted in settings and at times that are convenient to the family.
In the native language of the family or other mode of communication used by the family, unless it is clearly not feasible to do so. This may involve use of an interpreter.
Meeting arrangements must be made with, and written notice provided to, the family and other participants early enough before the meeting date to ensure that they will be able to attend.
IDEA Part C requires that parents be given prior written notice a reasonable time before the program proposes, or refuses, to initiate or change the identification, evaluation or provision of early intervention services. Prior Written Notice, Form 1-6 must be given to the family prior to the interim or initial IFSP meeting and before all IFSP meetings to review or evaluate the plan.
The contents of the IFSP must be fully explained to the parents and informed written consent obtained. Parents are given prior written notice before services begin by signing Section 8 of the IFSP Form 3-1.
Each early intervention service must be provided as soon as possible after the parent provides consent for that service and the IFSP has been signed by the primary health care provider. Part C of IDEA requires that eligible children and their families receive timely services. Connecticut has defined “timely” as within 45 days of the parent(s)’ signature(s) on the IFSP, therefore, in order to be in compliance with the law, all services that are scheduled to start
6
within 45 days of the parent signature on the IFSP must be delivered on time. This data will be reviewed annually, and program level data will be displayed on the Birth to Three website (www.birth23.org).
The IFSP must be reviewed at least every six months or more frequently if changes are needed or if the family requests a review. The purpose of this periodic review is to determine the degree of progress made toward achieving the outcomes and whether modifications or revision of the outcomes or services is necessary.
A meeting must be conducted on at least an annual basis to evaluate and revise as appropriate the IFSP for a child and family. The results of any current evaluations and other information available from the assessments of the child and family should be used to evaluate the IFSP. The updated assessment information about the child’s development must be in all five areas (cognitive, physical including vision and hearing, communication, social or emotional and adaptive).
For each child who may be eligible for preschool special education services (IDEA Part B), a transition conference must be convened with the approval of the family at least 90 days or at the discretion of the parties, up to 9 months, before the child’s third birthday. If the IFSP will be reviewed and possibly revised at this meeting, then Prior Written Notice Form 1-6 must be sent to the family in advance of the meeting.
For each child who is not being referred for preschool special education services (IDEA Part B), reasonable efforts should be made with the approval of the family, to convene a transition conference at least three months prior to the child’s exit from the Birth to Three System to review or develop a plan as part of the IFSP that supports the child’s transition to other appropriate services. If the IFSP will be reviewed and possibly revised at this meeting, then Prior Written Notice Form 1-6 must be sent to the family in advance of the meeting.
IFSP Meeting Participants
Per Section 303.343(a)(1) of the Part C Regulations under IDEA, the IFSP team must include the involvement of the parent and two or more individuals from separate disciplines or professions and one of these individuals must be the service coordinator.
Specifically at the initial meeting and each annual IFSP Team meeting to evaluate the IFSP, the team must include: (i) The parent or parents of the child,
(ii) Other family members, as requested by the parent, if feasible to do so, (iii) An advocate or person outside of the family, if the parent requests that the person participate. (iv) The service coordinator designated by the public agency to be responsible for implementing the IFSP, (v) A person or persons directly involved in conducting the evaluations and assessments. (vi) As appropriate, persons who will be providing early intervention services under this part to the child or family. 7
For periodic reviews the multidisciplinary IFSP team must include persons listed in (i) through (iv) above and if conditions warrant, provisions must be made for the participation of other representatives identified in (v) and (vi) above.
If a person listed in (v) above is unable to attend a meeting, arrangements must be made for the person’s involvement through other means, including one of the following: (i) Participating in a telephone conference call. (ii) Having a knowledgeable authorized representative attend the meeting. (iii) Making pertinent records available at the meeting.
Involvement of the Primary Health Care Provider
Connecticut General Statute 17a-248e(c) requires that the IFSP be developed in consultation with the child’s primary health care provider who is licensed in Connecticut or a contiguous state. To meet this requirement, the service coordinator should obtain parental permission to contact the primary health care provider indicating that his or her input is requested for a patient’s IFSP. The primary health care provider’s input should be sought regarding services that will be recommended and whether there are any contraindications warranted by the child’s medical status. Following the IFSP meeting, the IFSP form must be sent to the primary health care provider (physician or advanced practice registered nurse) for review and signature before implementation of services can begin. This signature serves as authorization for insurance billing. Since the IFSP is used to bill commercial insurance, the primary health care provider signing the IFSP must meet the insurance plan’s definition of primary health care provider. A faxed signature from the primary health care provider on the service page of the IFSP is acceptable.
The child’s primary health care provider (physician or advanced practice registered nurse) must sign the IFSP initially, whenever a service is added or increased and they must sign the IFSP after it has been evaluated which is done at least annually. When the primary health care provider signature is being sought for one of these reasons (other than the Initial IFSP), services that are continuing from a previous IFSP can continue uninterrupted, with parent agreement.
Interim IFSP
Early intervention services may begin for a child who is eligible for Birth to Three services prior to the completion of the multidisciplinary assessment if the following conditions apply:
A. Parental consent to develop an interim IFSP is obtained and the parent has been given prior written notice of the development of an interim IFSP using Form 1-6.
B. An interim IFSP is developed that includes: 1. the name of the service coordinator who will be responsible for the implementation of the interim IFSP and coordination with other agencies and persons, and 2. the early intervention services that have been determined to be needed immediately by the child and the child’s family.
8
C. The child’s primary health care provider (physician or advanced practice registered nurse) reviews and signs the IFSP.
D. The multidisciplinary assessment and the Initial IFSP must be completed within 45 calendar days from the child’s date of referral to Child Development Infoline.
An interim IFSP document contains all the IFSP pages and sections. Sections relating to the multidisciplinary assessment of the child which has not yet been completed may be brief.
Completing the IFSP Form
The Connecticut Birth to Three System’s IFSP form was created to support the concept that the development of this plan is a process that begins with the family’s first contact with the Birth to Three System. The IFSP form helps to document the process. If at any time while developing the IFSP one page of the form is not sufficient to record all the information, there is an additional blank page formatted to record the information and become part of the IFSP document. If the service coordinator does not have extra copies of this formatted page any blank piece of paper can be used and then made part of the document. The Parent/Guardian should initial or sign any additional pages that are added to the IFSP document.
When completing the IFSP form, clear and accurate documentation will prevent confusion and misunderstandings later on. The IFSP is a legal document that the parent signs upon completion. Whiteout and crossed out information should not be used on the form. If an error is made in writing information pertinent to the delivery of services and it is necessary to cross it out the change will need to be initialed and dated by the parent. This is especially important when completing section 8, Early Intervention Services and Supports.
If the service coordinator chooses to use a laptop computer on-site to produce the IFSP or chooses to enter the information and produce a typed version at the office, the parent must review and sign the typed version for it to be considered valid.
Throughout the IFSP form, an asterisk (*) next to an item denotes that the information for that item is part of the electronic record maintained in the CT Birth to Three Data System.
The following pages of this handbook show each section of the CT Birth to Three System’s IFSP form and the directions for completing this form. Throughout this handbook there are ideas that have been gained from service coordinators that will appear as a suggestion located in a separate text box following the directions for completing that section.
For additional information on the IFSP meeting please see the Birth to Three IFSP Procedure. 9
This page was intentionally left blank
10 11
Section 1 Child and Family Information
Purpose: Includes information about the child, family, primary health care provider, and service coordinator. This page must be completed as part of all IFSP meetings.
Meeting Type: One of the following should be checked to indicate the type of meeting:
Interim - If there are immediate needs for a child who has been determined eligible to receive services prior to the completion of the multidisciplinary assessment.
Initial - If this is the first complete IFSP written for the child and family.
Annual - If this is the meeting scheduled at least annually to evaluate the IFSP.
Review - If this is a review of the IFSP.
Meeting Start Date: The date that the IFSP Team began the meeting is the start date. The date the parent signs the completed IFSP is the date used to determine the 45 day timeline for the start of services.
Child's Name: The first and last name of the child.
Date of Birth: The month/day/year of the child's birth.
Male or Female: The box that applies should be checked.
Parent/Foster Parent/Guardian/Family Member: There are two boxes allowing for parents or guardians with separate addresses and contact information. The boxes may also be used to indicate that there is a parent and a foster parent involved with the child. The box on the left should be used for the person with whom the child lives. There is space for their home address, telephone number, and email address. The relationship of the person(s) listed to the child should be circled in the space above their name.
Program Contact Information: The name of the service coordinator assigned to the child and family, their contact number, the Birth to Three program they work for and the program director’s name and contact number, the program address and email address are written here. The service coordinator should be from the profession most relevant to the family’s or child’s needs and be qualified to carry out all applicable responsibilities. This person must hold a certificate indicating successful completion of service coordination training in Connecticut.
Physician/Health Care Provider: The child's primary health care provider name, telephone number, address and FAX number are written here.
Suggestion: To save time, this information should be filled in prior to the meeting. If the IFSP is printed from the child’s record in the CT Birth to Three Data System this information will be on the form. Reviewing the information with the family is advised in case there are changes or errors.
12
Section 2. Information about My Child
Purpose: Serves as a summary of information that has been gathered regarding the child's present abilities, strengths, and needs. The information must be based on current (no more than 3 months old) evaluation and assessment results, observations and parent report. This section must include a statement of the child's present level of physical development, (including vision, hearing, and health status), cognitive development, communication, social and emotional development, and adaptive development.
1. List any evaluations or assessments completed since last IFSP. Are reports attached? Yes _ No_. Check the appropriate box to indicate if reports are attached to this IFSP. Reports are listed by their type, not title. As an example, “Audiological, September 12, 2011", "Developmental Assessment, October 5, 2011", "Speech and Language Evaluation, November 2011”. Copies of these reports must be attached to the IFSP and are then considered part of the IFSP document and should be filed with the IFSP in the child’s record. If this is a periodic review of the IFSP and there are no recent assessments note that in this space.
2. General Health and Development Information: how is my child doing in these areas of development? So as not to repeat already reported information, the text, "see developmental summary dated…" may be written in this space. The report must then be attached to the IFSP. Additional comments could include a statement from the parent or professionals of developmental skills that the child has recently acquired that are not included in the referenced report. Some people may choose to summarize the assessment reports in this section. This is not necessary if the reports will be attached. 13
This page was intentionally left blank.
14 15
Section 3: Information about Our Family
Purpose: To assist families in identifying the important people and places in their family’s life.
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces.
Our Family Map (ECO Map): An eco-map is a simple tool that allows the service coordinator and family an opportunity to identify the important people and supports a family uses during the week. There is no right or wrong way to do an eco-map. One of the simplest ways involves drawing a circle in the middle of the page that contains the names of the people living in the home. Other lines connect from this main circle to other circles that may contain the names of extended family members, friends, clergy, medical personnel or others that the family identifies as supports.
It is important to read through the directions with the family before beginning the eco-map so they can understand its purpose. It is also important to stress that an eco-map can be changed throughout a family’s time in Birth to Three. People can be added or removed as life circumstances change or families become more comfortable sharing information. Most families enjoy talking about the people who are important in their lives. Others will need a few prompts such as “Do you have any family members who you regularly rely on for support or who you call on a regular basis to talk about your child?” You might ask specifically about grandparents, aunts, uncles, friends, coworkers or clergy if the family is slow to identify people.
If a family chooses to share minimal information with you, it is important to at least understand who is living in the home with the child in order to determine who to include when teaching families strategies. Assure the family that they can always add to the eco-map throughout their time in Birth to Three.
Places we go: This section allows the service coordinator and family to talk about where the child is during the day and evening in order to determine where services will take place. For example, a child may be at a childcare center on Monday, Wednesday and Friday mornings, at his paternal grandparents on those afternoons and at his aunts on Tuesdays and Thursdays. Understanding where the child is during the week makes it easier for the family and service coordinator to determine where and with who services will be scheduled.
16 17
Section 4: Daily Activities
Purpose: To understand what a family’s daily life looks like, what is working well and what they identify are areas of concern. This will help facilitate meaningful outcomes for the team.
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces
How is it going? There are seven times of the day that are typical for most families and an “other” box that can be used if needed or left blank. Begin each time of day segment by using a prompt like: “Tell me about what happens when people wake up?” Or: “How is it taking your child on outings? What’s working well?”
Developmental Skills Used. For those areas of development that are involved in the routines shared by the family, place a checkmark to indicate if this is an area of strength or concern. As an example; for a child who can pull to stand in his crib and then screams until his mother or father come into the room, you might check movement/sensory as a strength and communication as a concern. This helps the parent understand how what is happening during their daily routines is closely tied to the developmental needs of their child and whether it is something that needs to be addressed.
Either at the end of the page or after each time of day ask the family to indicate whether this is an easy time of day or there is some difficulty or it is difficult.
Again, either at the end of the page or after each time of day ask the family if this is an area of concern or a priority that the family would like to work on.
Suggestion: Sometimes the flow of the conversation is easier if the area of development and identification of areas of concern are completed after the discussion about the times of day. The service coordinator or team member can look at the routines and point out what developmental areas appear to be strengths or concerns. For example, “It looks like his movement and sensory skills are very strong however communication comes up in several times of the day as a concern.” Not all of the areas need to have a check in each column just those where is applies.
In the same manner asking the parent to prioritize which of the times of the day are priorities after the whole day has been discussed may make more sense.
18 19
Section 5: What Else is Important?
Purpose: To allow families further opportunity to talk about their child and any other family concerns.
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces
More information that will help everyone know what’s really important: Use the statements bulleted along the left side of the page as conversation prompts with the family. The lines are provided to record the family’s responses. The family members should be offered the chance to respond to the statements but not forced to give an answer to each.
Some of the information requested on this page may already have been gathered through the child/and family assessment. If that is the case you can remind them of the information they already shared and ask if they would like it recorded here. There is no need to have families repeat information they might have already given however, keep in mind most families enjoy sharing information about their children, even newborns, again and again.
What’s on my mind: These three questions give parents an opportunity to identify their biggest concerns and what they would like help with.
The adults in my child’s life learn best by: Because the plan and intervention will be geared toward the adults who are with the child daily, this section asks specific information about a learning style. This will allow the Birth to Three service providers to tailor how they explain and coach families on the techniques and strategies they are using with their children.
I am interested in being contacted by another parent whose child has gone through Birth to Three: Research shows that families often receive their greatest source of support from other parents whose children have similar disabilities but who are older. It is important to ask families if they would like to be contacted by another parent whose child has gone through Birth to Three rather than simply giving them a brochure on a parent organization or telephone number to call. Often family members are too overwhelmed to initiate a call or they lose the number or brochure under the avalanche of initial paperwork. If a parent is interested in being contacted by another parent or an organization, have them sign a CT Birth to Three release of information (Form 3-3) or one provided by the parent organization. You can then notify the parent or the organization of the contact information of the interested family. If the parent is initially not interested in being contacted, there is a space to indicate when the parent may be interested in being ask again. The service coordinator should continue to ask this question not just at each IFSP meeting, but throughout the family’s time in the Birth to Three System.
20 21
Section 6: Child/Family Outcomes
Purpose: Indicates the changes the family wants for themselves or for their child and relates to developmental information. This section must contain child outcomes and may include family outcomes. Outcomes should be functional and make sense to the family in the context of their everyday routines, activities, and environments. Outcomes should be based on a one year basis unless the child will be turning three sooner. Per IDEA 2004 the IFSP shall be in writing and contain “… a statement of the measurable results and or outcomes expected to be achieved for the infant and toddler and the family, including pre-literacy and language skills as developmentally appropriate for the child.
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces.
What we want to see for our child or family is: The desired major outcome for the child or family is recorded here using the family's words.
Suggestion: Often a family will express a very general need such as: "We want Timmy to walk" or “We want Timmy to talk”. To make the outcome more functional, go back to the family’s page on their daily routines and ask “when during the day is his walking/talking especially difficult?” This may lead to “We want Timmy to be able to get from room to room so that he doesn’t constantly cry to be picked up and carried to another activity”. The major outcome could be written as “We want Timmy to be able to get around the house on his own and let us know when he needs help”.
How will we know when we are making progress or done? These lines provide space for smaller, measurable steps (objectives). The objectives should be stated in language clear enough to answer the question: “Did it happen or not?” when they are reviewed. Service coordinators need to facilitate the conversation among parents and providers to keep the plan aimed at meaningful objectives centered on child and family routines.
Expected Timeline: This is only an estimate, so write the approximate timeframe for reaching each step. Some objectives may have the month/year or actual date listed (e.g. an audiological should be completed), but often timeframes will be reported in the number of months from the date of the plan being written. Timeframes should coincide with the sequence of implementation for the objectives. For example the first objective is projected to be reached in 2 months, the second objective in 4 months, 8 months (up to 12 months) unless the nature of the objectives has them occurring simultaneously. Ranges such as 2-4 months should not be used.
Met/Continue. The column to the right of the objectives is for use during the IFSP reviews. This can indicate whether the objective has been met or is being continued at Review #1, and again at Review #2.
What will we do to accomplish this? This space should be used by the team to identify the strategies that will be used to accomplish the outcome. It may be a brief description of specific
22 ideas that can be used in the child and family's daily routines or this section can clarify for the family what is going to happen during home visits. For example: “The primary Birth to Three staff person will start each visit by reviewing how Timmy is doing and ask what has been happening during his daily routines with caregivers. Ideas for activities will be generated and input from other team members will be sought on how to support Timmy’s abilities.”
This is also the section where methodologies such as Applied Behavior Analysis (ABA) or Picture Exchange Communication System (PECS) should be indicated.
If the team is considering the use of an assistive technology device, obtaining the device should be listed as a strategy.
Progress Updates: Space is available for at least two updates of the outcome at subsequent IFSP reviews. In the column to the right under Outcome, circle the word Met, Continued or Revised to indicate the current status of this outcome.
Suggestion: When reviewing the IFSP bring the full document (copy or original) to reference and be sure to have copies of the outcome pages so that the updates can be written directly on the page and added to the new IFSP document. Additional blank pages of the IFSP, especially outcome pages, should be brought so that those sections can be updated as needed.
Other Services Related to this Outcome That Are In Place or That are Needed
Purpose: Birth to Three is only a piece of the larger support network for the child and family. This section identifies services that are in place or desired by the family to address this outcome. These supports or services are not required early intervention services under Part C of IDEA, yet they will be considered as part of the overall plan. The service coordinator is responsible for assisting the family to obtain and coordinate these services with the Birth to Three services.
What other services and supports do we need?: This space may contain the name and type of the support that is in place or one that the family is seeking to support this outcome. This includes all services such as medical (beyond routine medical services, unless they are required services that are not being provided so listing them here means the service coordinator will assist family to access them), religious, social or other child-related services that the child needs but are not required early intervention services under Part C of IDEA.
Since there is space for other services on each outcome page the services listed should be specific to the outcome. If these other services listed for the first outcome are connected to several outcomes, then the service should be briefly stated on each additional outcome that it supports.
Who will pay for it? The funding or payment source for each of the other service or supports is listed here. For example, a family has enrolled their child at the Happy Valley Daycare Center and she attends that program three days per week. The payment source is the family. This space is left blank if the payment source is not yet known. 23
This page was intentionally left blank.
24 25
Section 7: What’s Next for us (Transition Plan)
Purpose: It provides an opportunity to record the discussion of the family’s concerns for the changes that may be coming up and the child’s eventual transition from the Birth to Three System. The plan must include the steps to be taken to support the transition of the child including discussion with, and training of, parents regarding future placements and other matters related to the child’s transition; procedures to prepare the child for changes in service delivery, including steps to help the child adjust to, and function in, a new setting. This plan must be completed during the initial and annual IFSP and revised as needed during periodic IFSP reviews.
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces
What changes are coming up for us in the next few months? Briefly state what if any changes are coming up for the family. This may include planning for a parent going back to work, the child starting childcare or preparing for an upcoming move.
What will help us prepare for this? Using the table identify What actions or activities may help the change written above, Who will help and the approximate date or timeframe under When?
Plan for Transition from the Birth to Three System: This part of the Transition plan is specific to planning for when the child will exit Birth to Three. There is room to indicate what concerns the parent has and what options were discussed. A list is given of possible options that the family may be interested in having the service coordinator work with them to identify. This should not be seen as a list of options for the LEA to provide.
Transition Timeline Dates: This space is used to document the dates that will meet the transition timelines if the family is planning on referring their child to the local school district for a determination of eligibility for preschool special education.
With parent permission, the child’s school district can be notified and information shared at any time that the child is enrolled in the Birth to Three System using the Authorization to Release Information, (Form 3-3). School districts need this information for planning purposes and parents should be encouraged to give their permission as early as possible. There is a space to indicate the date that the IFSP team is recommending for a formal referral to be sent to the local school district (Form 3-8). Optimally this should occur by 24 months of age, if it appears that preschool special education services will be needed. Completing this section will help the parent and team plan ahead for the transition. Space is also available to indicate the timing or completion of the Transition Conference which must occur no later than 90 days before the child’s third birthday.
School District Contact Information, Name and Phone: The name of the school district that will be responsible if the child requires preschool special education services at age three and the school district contact person and their telephone number is indicated here. The name of the school district and contact person can be obtained by going to the CT Birth to Three website
26 www.birth23.org, locating the town that will be responsible for the child at age 3 and then clicking on the preschool contact information for that town.
What will help prepare our family and child for the next setting? Using the table identify What actions or activities may help with the transition from Birth to Three services, Who will help and the approximate date or timeframe under When? 27
This page was intentionally left blank
28 2444 29
Section 8. Early Intervention Services and Supports
Purpose: Indicates the early intervention services and supports necessary to meet the unique needs of the child and family to achieve the desired outcomes as previously written. The decisions regarding what services and supports will be provided, including type, frequency, location, intensity, and duration, can only be made after the development of outcomes and strategies. Services (including assistive technology devices and services) that address the strategies are determined through discussion with the family and must be delivered as indicated on the IFSP. Family members and professionals are encouraged to talk about services and supports openly and to make joint decisions based upon the outcomes chosen and the strategies developed by the team. The decision to provide a service or support cannot be based solely upon factors such as: nature or severity of disability, age of child, availability of services, administrative convenience, family preference, payment methodology, or service provider preference.
The early intervention services under Part C of IDEA are: assistive technology devices and services; audiology, family training; counseling and home visits; health services necessary to enable the child to benefit from other EI services; medical services only for diagnostic or evaluation purposes; nursing services; nutrition services; occupational therapy; physical therapy; psychological services; service coordination; sign language and cued language services; social work services; special instruction; speech-language pathology; transportation and related costs; and vision services. (see the Services Procedure for more information).
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces
Meeting Type: Checked the appropriate box to indicate the type of meeting
Program Name/Fax Number: The name the Birth to Three program and Fax number should be clearly written in this space. That way if this page gets separated from the complete IFSP when being sent to the primary health care provider, the name and Fax number of the program to return it to is present.
What is Going to Happen: This space should indicate to the parent the kind of service or support that will be provided to their child and family. These are necessary early intervention services. The options for this column when entering the IFSP into the Birth to Three data system are: Assessment, Assistive Tech Service, Audiological Management, Consultation, EI Visit, Family Counseling, or Family Training, health services, medical services, mobility training, teaming with family, vision services or transportation. List only those services and supports that will actually be delivered when this IFSP is implemented. This is a working document and it should be revised as needed.
Each child’s IFSP will specify any transportation arrangements and related costs that are necessary to enable a child to receive early intervention services. The program may provide transportation directly, contract it from a commercial carrier or reimburse the family at a reasonable
30 rate for the use of their own car. There will be a check box in the data system to indicate if transportation or related costs are included on the IFSP.
Suggestion: Consultation is when a visit is made to the child and family for the purpose of giving advice to the family, primary interventionist, or team. When the team knows a consultation is needed it should be listed on the IFSP, if the need arises later for someone to consult it can still occur without being on the IFSP. In this case it should be indicated in a visit contact note and in the child’s attendance in the data system. If there will be future visits as a result of the consult, then the IFSP should be updated to reflect the new service.
It is possible to list a service considered by the IFSP team to be a necessary service, which might be provided or funded by another agency (e.g. Board of Education and Services for the Blind). If it is listed here and the other agency is not able to deliver the service or discontinues it, the Birth to Three program is still responsible to provide this service. The delivery of the service by the outside agency does not need to be reflected in the data system but should be tracked by the service coordinator and reflected in the contact or service coordination notes.
Suggestion: For a child receiving intensive services, a regularly scheduled team meeting with the family is recommended to ensure that everyone is providing coordinated services. This should be listed as team meeting under “What is Going to Happen” and the team members who will participate should be listed under “Delivered by”. For programs that receive supplemental funding for those children receiving intensive services, team meetings will not be counted toward the reimbursement unless it is listed on the IFSP.
If assistive technology devices or services are to be part of the IFSP, they must be listed separately in this section and also be indicated as a strategy for one or more of the outcomes.
Suggestion: For an assistive technology device, the boxes for “Location”, “How Often” and “How Long” may not apply and can be left blank. In the box for “Start Date”, write the expected date of delivery of the service or device, allowing for processing of insurance claims and ordering time. When entering assistive technology devices into the Birth to Three Data System the box indicating that assistive technology is part of the plan is checked but the service grid will not be completed for the device.
Delivered by (discipline responsible): The discipline of the person who will be delivering the early intervention service or support is indicated here (see CT Birth to Three System Procedures Manual - Personnel Standards for disciplines approved to deliver early intervention services in CT).
Suggestion: Each individual delivering a service should be represented on a different line. If several disciplines are listed on one line it means they are regularly providing the service at the same time. For example: parent support group may be written as 1 time a week for one hour with the social worker and nurse. Another instance where several disciplines may be listed on the same line is if there will be several disciplines regularly meeting as a team with the family. It is important to be very clear with the family what services they can expect to be delivered by whom and for what length of time. If visits that are intended to be joint visits are listed on 31
separate lines, there must be somewhere else in the IFSP such as the additional page to indicate that they understand that visits will be made at the same time.
Location: The service coordinator indicates where the service will be delivered using only one location per box. If the physical therapist will be regularly making an early intervention visit at home and also at the child’s Early Head Start classroom, they must each be listed on separate lines with separate frequency and intensity. It is reasonable to occasionally vary the location of a service listed for the home by providing it in a community setting such as the neighborhood playground or the local grocery store. This change should be noted in contact or service coordination notes but does not affect the IFSP as written.
Suggestion: IFSPs for children requiring intensive services may pose an organizational difficulty for the service coordinator who is conducting the meeting and trying to fill out the form at the same time. In these cases, it is suggested that the information that is required for Section 8, the service grid, be written on a chart or calendar page first and then recorded on the IFSP document after the team has agreed on the services. The chart will enable everyone participating in the meeting to review the proposed services and see what the daily/weekly schedule looks like for the child and family. This will lead to fewer errors on the final IFSP document. This chart or calendar page can be attached to the IFSP document as an additional page.
How Often: This is where the team indicates how often (frequency) the service will be delivered. The terms "up to" when used in "up to four times a month" and "as needed" do not help families predict a schedule for delivery of services. Frequency such as one time a week, four times a month or monthly should be used instead. There will be instances where service delivery will occasionally exceed or be less than the amount indicated on the IFSP. Any variation in service must be documented in the service coordination notes. The attendance in the data system should reflect the services actually delivered. If the changes are more than occasional, the IFSP will need to be revised.
Often the team will identify an assessment that needs to occur prior to the next scheduled IFSP review and wish to document it as a listed service. The type of assessment should be written in the "What is Going to Happen" box. "How Often" should state the number of anticipated sessions, for example 1-2 visits. "How Long" should state the anticipated length of each session, for example 1-3 hours. Only in the instance of assessments, may estimated rather than actual number of sessions and hours be written.
If there is no documentation in the IFSP that agreement with the family has been reached about program schedules, such as vacations, meetings, etc., the program is legally obligated to deliver exactly the number of hours as specified. Use the meeting notes in section 9 or an additional page to document this agreement and discussion.
How long: The length of time (intensity) the service will be delivered each time is written here. For example: "1 hr.”
Start Date: The date services will begin should be written here. For an initial IFSP or for one with new services, this date should reflect an estimate of when the primary health care provider’s
32
signature will be obtained. When services are going to be phased in or out, use two lines on the grid to indicate the date each service will begin and end.
End Date: The date that the services listed on this line will end is indicated here. The IFSP is written for up to one year. Unless the plan is to adjust the services at an earlier date, the service end date should be listed as the date of the projected annual meeting to evaluate the IFSP or the day before the child’s third birthday if that date comes first.
How Start End What is Going to Happen Delivered by: Location How Often (discipline responsible) Long Date Date Early Intervention visit Teacher Home 2 times a week 2 hours 3/3/11 3/16/11 Early Intervention visit Teacher Home 4 times a week 2 hours 3/17/11 3/17/12 Using the start and end dates, the plan can reflect a phase-in of the frequency/intensity of services or addition of service types on the service grid using staggered start and end dates.
For example, the grid above shows that an Early Intervention teacher will increase from 2 times a week to 4 times a week in two weeks. This could also be done in the reverse where services will decrease over time.
Part C Services are paid for by the Birth to Three System unless otherwise indicated here: Under Connecticut statute, the Birth to Three System is the payer of last resort. If there is some payment arrangement for an early intervention service listed in the grid above it should be listed here.
Check if any early intervention service cannot be achieved satisfactorily in a natural environment and attach a justification for each service: If any service listed is not delivered in a natural environment, the Justification for Early Intervention Service that Cannot be Achieved Satisfactorily in a Natural Environment page of the IFSP must be completed for each applicable service. Audiological testing, parent groups and counseling for parents do not require justification (for additional information regarding natural environments see CT Birth to Three System Service Guideline #2: Natural Environments).
Informed Consent by Parents: There are two very important acknowledgements that a parent makes in this section. First, parents must give their permission for services to be delivered by checking line A. If they do not agree with the complete plan they can indicate this by checking B and listing those services that they do agree to have start on the lines below. If an IFSP is already in place and is not expiring and the parent does not agree with a revision of an IFSP that has been developed, then the existing IFSP continues to be carried out until the team can develop a plan to which the parent gives consent.
When a parent does not accept an IFSP fully, the provider must take steps to resolve the issue and in the meantime the services that are agreed upon must be delivered. By checking B the parent is acknowledging that if the team cannot come to an agreement within one month, they will request mediation, file a written complaint, and / or request a hearing. 33
Second, under Federal law, parents must indicate that they understand their rights. The service coordinator gives the CT Birth to Three System booklet entitled Parent’s Rights Under IDEA, Part C out initially and at least annually to parents and takes the time to review these rights with the parents. The parent documents that they understand their rights by signing this page.
Parent Signature: The parent, the appointed surrogate parent, or someone who is acting in the parental role must sign here. Department of Children and Families staff members or contractors such as safe home staff may not sign the IFSP because they do not meet the IDEA definition of parent.
Physician Signature: The child’s primary health care provider (physician or advanced practice registered nurse) signs here indicating confirmation of the appropriateness of the diagnosis(es) as stated by the diagnostic code and the recommendations for the services as they are written. This signature serves as an authorization for insurance billing. Form 3-6 is the cover letter that should accompany the initial IFSP being sent to the primary health care provider and Form 3-7 should accompany revised IFSPs. To expedite the return of the signed service page, a faxed signature is acceptable.
Lic#: The physician or Advance Practice Registered Nurse (APRN) writes his or her CT license number here.
Date: The physician or APRN writes the date he or she signed the IFSP here. No new services can be provided prior to this date.
Print name: The service coordinator prints the name of the physician here.
ICD-9 Code(s): The service coordinator lists suggested ICD-9 code(s) (International Classification of Diseases-9th revision) for the physician or APRN to approve.
34 35
Section 9 IFSP Team Members
Purpose: Serves as a record of the persons who participated at the IFSP meeting either by being present or by providing information via a report or some other means. This helps the team identify those team members who are not present but who are going to assist in the implementation of the IFSP.
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces.
Name/relationship/phone: Each person’s name, relationship to the child, and phone number and method of participation is listed here. A signature is not required; the recorder can list the team members who participated.
Method of participation : Check the box that indicates how that team member participated in the development of the IFSP.
Meeting notes: This section is used to record notes about what occurred at the IFSP meeting. For example this may include decisions by parent to not have services provided at the childcare setting or plans to make some visits at a relative’s home.
Missed Visits: This statement gives the language regarding the policy on cancelations and rescheduling visits. The service coordinator needs to have discussions with the family about the program’s schedule and the effects of cancellations on that schedule. Service coordinators should negotiate these terms with families and make sure it is documented here or on an additional page that then becomes part of the IFSP document. The service coordinator should clarify with the family if there are known days that will be a problem for the family or Birth to Three staff and how these missed visits will be handled including whether someone and if so who, will substitute. A check of this box is all that is required to indicate it has been discussed. Blanket statements issued by agencies on holidays and cancellations will not cover the legal obligation of the program to provide the services that are listed on the IFSP.
36 37
Additional Page
Purpose: Serves as extra space to be used, if needed, for reporting information or discussion under any section of the IFSP. When used, this page becomes a part of the IFSP document.
Child’s Name/DOB/Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP, are written in these spaces.
This page has been formatted to be used as an additional page for any sections of the IFSP form where there is insufficient space to record the required information.
This page should not be used for any way to provide specific program information that implies is it part of the CT Birth to Three System’s IFSP form.
38
39
Justification for Early Intervention Service that cannot be Achieved Satisfactorily in a Natural Environment.
Purpose: This page serves as a place to write a justification of the extent to which services will not be provided in a natural environment. Per regulations all early intervention services must be delivered in the child’s natural environments as described in Section 303.26. If a service cannot be achieved satisfactorily in a natural environment, the box on Section 8 Early Intervention Services and Supports is checked and a justification page must be completed for each service not provided in a natural environment.
Because audiologicals and counseling or support groups for parents do not usually occur in the child’s natural environment they do not require justification. (For additional information regarding natural environments see CT Birth to Three System Service Guideline #2: Natural Environments).
Child's Name/DOB/Meeting Start Date: The first and last name of the child, the child’s month/day/year of birth, and the date or dates that the meeting was held to develop the IFSP are written in these spaces.
Service: Indicate the service that will not be provided in a natural environment.
Location: Indicate the location of each service that will not be provided in a natural environment.
Complete the following questions for the service: Explain how and why the child’s outcome(s) could not be met if the service were provided in the child’s natural environment with supplementary supports. If the child has not made satisfactory progress towards an outcome in a natural environment, include a description of why alternative natural environments have not been selected or outcome not modified.
Explain how services provided in this location will be generalized to support the child’s ability to function in his or her natural environment.
Describe a plan with timelines and supports necessary to allow the child’s outcome(s) to be satisfactorily achieved in his or her natural environment.
40
Language & Communication Plan For Children in the Connecticut Birth to Three System
This tool is designed to assist the IFSP team in identifying the ongoing unique communication considerations of children who are deaf or hard of hearing that should be reflected in the IFSP.
Child’s Name: ______Date: ______Service Coordinator’s Name: ______Program: ______
The service coordinator and the IFSP team have considered and discussed:
1. Issues related to making a decision about a communication approach 0 How does the child’s family communicate? ______What communication approaches has the family been informed about for their child? ______What are the family’s wishes with regards to child’s communication mode at this time? ______
2. Opportunities for direct communication with children and, or adults who are deaf or hard of hearing and who are using the chosen communication approach: ______
3. The child and family will be supported by the following professionals who are knowledgeable and experienced in working with children with hearing loss and the chosen communication approach: ______
4. Assistive technology devices that will be used with the child while enrolled in the Birth to Three System: ______
5. Additional comments or concerns: ______
For more information, please see the CT Birth to Three Service Guideline #5 Young Children Who are Hard of Hearing or Deaf.
Connecticut Birth to Three System Form 3-19 (7/1/13) 41
Language & Communication Plan For Children in the Connecticut Birth to Three System
The Language and Communication Plan (LCP) for children in the Connecticut Birth to Three System, Form 3-19, should be completed with the family by the IFSP team prior to the initial, annual or any periodic review of the IFSP. It may also be helpful for the parent to review in preparation for transitioning out of the Birth to Three System. The plan was developed to prompt a discussion about the family’s understanding of their child’s needs and the possible outcomes, strategies or services that the IFSP should address. For more information, please see the CT Birth to Three Service Guideline #5 Young Children Who are Hard of Hearing or Deaf.
There is also a Communication and Language Plan as part of the Connecticut Individualized Educational Plan (IEP). To view the IEP document go to the Connecticut State Department of Education website www.ct.gov/sde, There is also a copy of the LCP in Appendix Six of the Connecticut Birth to Three Service Guideline #5 Young Children Who are Hard of Hearing or Deaf.
42
Periodic Review of the IFSP
The IFSP is reviewed at least every six months; (more frequently if conditions warrant or the family requests such a review) and evaluated at least annually. Each time an IFSP is reviewed the clock starts again on the requirement that IFSPs be reviewed at least every six months but does not change the date for evaluating the complete IFSP on at least an annual basis. The purpose of a periodic review is to determine the degree to which progress toward achieving the outcomes is being made and whether modifications or revision of the outcomes, services or other information (such as the plan for transition is necessary).
The service coordinator is responsible for making sure there is a multidisciplinary team to review the IFSP and that prior written notice is given before all reviews of the IFSP, unless the parents have initiated the request to review the plan.
The following sections of the IFSP must be included in a review: Section 1 Child and Family Information and
Section 2 Information about My Child
Section 6 Child/Family Outcomes –for all reviews the service coordinator will bring a copy of the original IFSP outcome pages so that they may be reviewed and updated during the meeting. These pages then become part of the IFSP review. Additional blank outcome pages may be needed if an outcome is rewritten or a new one is added.
Section 8 Early Intervention Services and Supports
Section 9 Who is Part of Our Team
Any of the other pages of the IFSP form may be added as needed to document the meeting.
The child’s primary health care provider (physician or advanced practice registered nurse) must sign the IFSP whenever a service is added or increased. Services that are continuing from a previous IFSP can continue uninterrupted, with parent agreement, until the IFSP is signed.
Suggestion: if the sole purpose of the periodic review of the IFSP is to review or revise a transition plan during a transition conference with school district personnel present, the service coordinator may choose to update the progress on the child’s and family’s outcomes in 44 advance of the conference and complete those sections of the page prior to the transition conference. This will allow more time to focus on the next steps in transitioning from the Birth to Three System. 43
Annual Meeting to Evaluate the IFSP
Purpose: Addresses the requirement in federal regulation that the IFSP be evaluated completely on an annual basis. A review of the progress made toward achieving the child and family’s outcomes as well as information from current evaluations and ongoing assessments of the child’s abilities should form the basis for this review.
According to IDEA Part C regulations, a meeting must be conducted at least annually to evaluate the IFSP for a child and family, and, as appropriate, to revise its provisions. The service coordinator should give the family prior written notice (Form 1-6) of this meeting. The results of any current evaluations (within the past three months) conducted under § 303.321 and other information available from the ongoing assessment of the child and family must be used in determining what services are needed and will be provided. Therefore, there must be current information available on the child’s development in all five domains. This information does not need to be the result of a multidisciplinary assessment. The child’s primary interventionist (if that person is an E.I. professional) can provide all of the assessment information, although if there are others team members serving the child and family, their information should be included.
To evaluate the IFSP, the service coordinator should ensure that proper notice of the meeting is sent to the participants. The IFSP meeting arrangements must be made and prior written notice provided to the family. Use Form 1-6 (Prior Written Notice) for this purpose.
The multidisciplinary team for this meeting must include the parent, the service coordinator and a person or persons directly involved in conducting the most recent evaluation or assessment. Other people who may attend are family members as requested by the parent if feasible to do so, and an advocate or person outside of the family if the parent requests their participation. To document the complete evaluation of the IFSP, the service coordinator will complete all sections of the IFSP form. The service coordinator should bring a copy of the most current IFSP outcomes to review before new outcomes are written. It will also be helpful to have the last full IFSP form to use as a starting point when it comes to updating the other sections of the IFSP.
In Section 8, the start dates for all services should reflect the new date of this meeting. This IFSP must be sent to the primary health care provider with parent permission, for review and signature.
Completing the IFSP Form for a Child Receiving Those Services Provided at No Cost
If a family of an eligible child meets the criteria for the Family Cost Participation fee (see Family Cost Participation Procedure) they may request to receive only those services that are available at no cost. By IDEA Part C regulations, the following services must be provided at no cost to the family: evaluation, assessment (initial and annually), IFSP development and review, service coordination (including transition planning) and procedural safeguards.
When a family of a child eligible for Birth to Three services chooses to only receive those services available at no cost to the family the entire IFSP should be completed as it would be for any IFSP, reflecting information about the child and the family concerns as well as outcomes, transition plans
44 and the team members who participated in the development of the plan. The outcome page must include strategies that reflect family and community resources since Birth to Three direct services will not be provided.
The service grid on Section 8 can be left blank or an annual assessment can be listed on the grid. Service coordination is already identified on the page and can be highlighted making sure the correct name and contact information is listed.
The parent still signs the IFSP indicating they have received their rights and are in agreement with the plan. If they give written permission to send a copy of the plan to the primary health care provider, the completed IFSP is sent, however the primary health care provider's signature is not required since no direct services are being provided.
The same procedures should be used when doing a periodic review or annual review of the IFSP for a family that will be receiving only those services provided at no cost as would be done with a family that is receiving direct services.
Suggestion: To help the family understand what will be happening as a result of this plan, it is recommended that the service coordinator attached a page to the IFSP or use the meeting notes section to write a brief description of what will be happening (e.g. monthly contact by phone and a face to face visit quarterly by a service coordinator, etc.).
The same timelines, meeting participants and review process and due process rights that have been outlined in this handbook should be followed when working with a family that will be receiving only those services provided at no cost.
Implementation of the IFSP
After the initial IFSP or any IFSP review that results in adding a new service or an increase in the frequency of an existing service, as well as the IFSP that is evaluated and rewritten at least annually, the service coordinator will get a signed release (Form 3-3) from the parent to send the IFSP to the child’s primary health care provider for signature. This signature is required before the start of the initial IFSP services and any new or increased services that are planned.
As soon as possible following any IFSP meeting, the service coordinator should send a full copy of the IFSP (with all referenced reports attached) to the parent and copies to anyone else the parent has listed on a signed release (Form 3-3).
Programs must ensure provision of the services described in the IFSP as soon as possible after obtaining the required primary health care provider’s signature (see Services Procedure for the definition of Timely Services). Programs cannot provide or arrange for a service for which the parent has not given consent or for which consent has been withdrawn in writing. 45
Frequently Asked Questions
Q. What if the family I am working with is very reluctant to fill out the eco-map or talk about their daily routines?
A. It is important to explain to families why we are asking questions about their families and their daily life before the IFSP begins. For some families an explanation may be all it takes overcome their reluctance. For others gentle prompts such as “Who do you call when you are worried about something?” Or “Tell me about your morning routine, how do you get all three children out the door and to childcare before 7:00 AM?” If a family gives brief or incomplete answers assure them that you can always return to this section and add to it at a future IFSP.
For the very rare family who refuses to talk about family or routines this might be a good opportunity to talk about the coaching model. A family expecting services to be delivered in a more traditional outpatient rehabilitation model may see no need to share personal information. Understanding that in Birth to Three professionals demonstrate and show them techniques to use with their child throughout their daily routines may help them share information. Ultimately a family can share as much or as little as they want to and still receive Birth to Three services.
Q. Some of the questions I ask during the IFSP have already been covered in the assessment. Do I have to ask the family to repeat their answer?
A. No. You can fill that information in before the IFSP if you like. You can also use the information from the assessment as a way to enhance their previous answers and learn more about the family during the IFSP. For example, “I know you mentioned your mother and grandmother were a huge source of support to you when your baby was in the hospital. Now that he is home, who are the other people in your life that you know you can count on for support?”
Q. Where do I put discrete trial training or ABA on the IFSP?
A. The strategies should be written in Section 6 Child/Family Outcome as a strategy not as a service in Section 8 Early Intervention Services and Supports. These are methods used to achieve an outcome.
Q. How can we document that we have encouraged a family to consider a service or a higher frequency of a service that was not accepted?
A. This could be reflected as part of a discussion and the parent’s refusal or reluctance to accept the service or service frequency in the Meeting Notes in Section 9. The additional blank page can be used if more space is needed.
Q. What if the family wants an “alternative” approach like cranio sacral or mega vitamin therapy?
A. The Birth to Three System does not provide these alternative treatments but will support a parent’s effort to pursue that treatment on their own. If appropriate this should be listed in Section
46
6 under Other Services that are related to this Outcome that are in Place or Needed and coordinated with the child’s Birth to Three services as much as possible.
Q. If I need the occupational therapist for a one time consult, do I need to revise the IFSP to indicate this as a service?
A. No. One time consults that are needed during the course of delivering services to a child that did not come up at the IFSP meeting do not have to be listed on the IFSP. However, if at the IFSP meeting the team already knows that a consult by the occupational therapist to the primary service provider will be needed in the next six months, list it on the IFSP with an expected start date several months from the date of the IFSP.
Q. If I want to add an outcome that does not change the services being delivered, do I have to do a review?
A. The purpose of reviewing the IFSP is so that the parent knows something has changed for the child. Something would have had to change to warrant a new outcome. If the IFSP will not be reviewed then instead of a new outcome this change should be reflected in the contact notes.
Q. Where on the IFSP do I list services provided by Board of Education and Services for the Blind (BESB)?
A. If the service being provided by BESB is a required service under IDEA Part C, it must be listed in Section 8 under “What is Going to Happen” and BESB should then be listed in the box entitled “Services are paid for by the Birth to Three System unless otherwise indicated”. In the event BESB discontinues delivering the service; the program is still responsible to provide the service as written on the IFSP. If BESB or another agency is providing a service or support to a family that the team wants to be reflected on the plan but the service is not one required under IDEA Part C then this service or support should be written in Section 6 under Other Services Related to this Outcome that are in Place or Needed. 47
APPENDIX Family Assessment Tools
Samples included:
Family Needs Scale C.J. Dunst, C. M. Trivette, and A.G. Deal (1988). Enabling and empowering families: Principles and guidelines for practice. Cambridge, MA: Brookline Books.
Family Resource Needs, A Screening Tool Adapted with permission from Project Dakota Outreach, 680 O’Neill Drive, Eagan, MN 55121
Family Resource Scale Healthy Families America, 1996
Others suggested family assessment tools not included:
Routines Based Interview – Robin McWilliam http://www.siskinresearch.org
AEPS Family Interest Survey Assessment, Evaluation and Programming System (AEPS) for Infants and Children By Juliann Cripe, Ph.D., and Diane Bricker, Ph.D. Brooks Publishing Co., P O Box 10624, Baltimore, MD 21285
48 Family Needs Scale Carl J. Dunst, Carolyn S. Cooper, Janet C. Weeldreyer, Kathy D. Snyder, & Joyce H. Chase
Name ______Date ______
This scale asks you to indicate if you have a need for any type of help or assistance in 41 different areas. Please circle the response that best describes how you feel about needing help in those areas.
To what extent do you feel the need for any Not Almost Almost of the following types of help or assistance: Applicable Never Seldom Sometimes Often Always
1. Having money to buy necessities and pay bills...... NA 1 2 3 4 5 2. Budgeting money...... NA 1 2 3 4 5 3. Paying for special needs of my child...... NA 1 2 3 4 5 4. Saving money for the future...... NA 1 2 3 4 5 5. Having clean water to drink...... NA 1 2 3 4 5 6. Having food for two meals for my family...... NA 1 2 3 4 5 7. Having time to cook healthy meals for my family...... NA 1 2 3 4 5 8. Feeding my child...... NA 1 2 3 4 5 9. Getting a place to live...... NA 1 2 3 4 5 10. Having plumbing, lighting, heat...... NA 1 2 3 4 5 11. Getting furniture, clothes, toys...... NA 1 2 3 4 5 12. Completing chores, repairs, home improvements...... NA 1 2 3 4 5 13. Adapting my house for my child...... NA 1 2 3 4 5 14. Getting a job...... NA 1 2 3 4 5 15. Having a satisfying job...... NA 1 2 3 4 5 16. Planning for future job of my child...... NA 1 2 3 4 5 17. Getting where I need to go...... NA 1 2 3 4 5 18. Getting in touch with people I need to talk to...... NA 1 2 3 4 5 19. Transporting my child...... NA 1 2 3 4 5 20. Having special travel equipment for my child...... NA 1 2 3 4 5 21. Finding someone to talk to about my child...... NA 1 2 3 4 5 22. Having someone to talk to...... NA 1 2 3 4 5 23. Having medical and dental care for my family...... NA 1 2 3 4 5 24. Having time to take care of myself...... NA 1 2 3 4 5 25. Having emergency health care...... NA 1 2 3 4 5 26. Finding special dental and medical care for my child.....NA 1 2 3 4 5 27. Planning for future health needs...... NA 1 2 3 4 5 28. Managing the daily needs of my child at home...... NA 1 2 3 4 5 29. Caring for my child during work hours...... NA 1 2 3 4 5 30. Having emergency child care...... NA 1 2 3 4 5 31. Getting respite care for my child...... NA 1 2 3 4 5 32. Finding care for my child in the future...... NA 1 2 3 4 5 33. Finding a school placement for my child...... NA 1 2 3 4 5 34. Getting equipment or therapy for my child...... NA 1 2 3 4 5 35. Having time to take my child to appointments...... NA 1 2 3 4 5 36. Exploring future educational options for my child...... NA 1 2 3 4 5 37. Expanding my education, skills, and interests...... NA 1 2 3 4 5 38. Doing things that I enjoy...... NA 1 2 3 4 5 39. Doing things with my family...... NA 1 2 3 4 5 40. Participation in parent groups or clubs...... NA 1 2 3 4 5 41. Traveling/vacationing with my child...... NA 1 2 3 4 5
Source: C.J. Dunst, C.M. Trivette, and A.G. Deal (1988). Enabling and empowering families: Principles and guidelines for practice. Cambridge, MA: Brookline Books May be reproduced. 49
Family Resource Needs A Screening Tool
1. What concerns you most about your child or caring for your child?
2. Do you need information or assistance for weekday, weekend, and overnight childcare or respite?
3. We know of parents who would be willing to visit with you by phone or in person to offer support and a listening ear. Does this interest you?
4. Would you like more information or assistance regarding medical/health services?
5. Do you want more information or assistance with early intervention services or adaptive equipment?
6. Would you find it helpful to hear about different types of financial assistance for medical costs or other expenses that you have?
7. Would you like (more) assistance in finding resources, working out problems with agencies, and getting more appropriate services, transportation, or communications with agencies?
8. Is there other information you are looking for now?
Project Dakota Outreach Healthy Families America Training Manual ©1996 50 Family Resource Scale This scale is designed to assess what resources you need for your family. For each item please check the response that best describes how well each need is met on a regular basis (that is month to month). To what extent are the Does Almost Not at all Seldom Sometimes Usually following resources Not always adequate Adequate Adequate Adequate adequate for your family: Apply adequate 1.Food for two meals a day
2. House or apartment
3. Money to buy necessities
4. Enough clothes for your family
5. Heat for your house or apartment
6. Indoor plumbing/water
7. Money to pay monthly bills
8. Good job for yourself or spouse/partner
9. Medical care for your family
10. Public Assistance (SSI, TANF, Medicaid, SNAP etc)
11. Dependable transportation
12. Time to get enough sleep/rest
13. Furniture for your home or apartment
14. Time to be by yourself
15. Time for family to be together
16. Time to be with your child/children 17. Time to be with spouse/partner or close friend 18. Telephone or access to a phone 19. Babysitting for your child/children 20. Child care for your child/ children 21. Money to buy supplies for your child/children
22. Dental care for your family