New Mexico Midwives Association: Practice Guidelines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Risk Factors Associated with Maternal Age and Other Parameters in Assisted Reproductive Technologies - a Brief Review
Available online at www.pelagiaresearchlibrary.com Pelagia Research Library Advances in Applied Science Research, 2017, 8(2):15-19 ISSN : 0976-8610 CODEN (USA): AASRFC Risk Factors Associated with Maternal Age and Other Parameters in Assisted Reproductive Technologies - A Brief Review Shanza Ghafoor* and Nadia Zeeshan Department of Biochemistry and Biotechnology, University of Gujrat, Hafiz Hayat Campus, Gujrat, Punjab, Pakistan ABSTRACT Assisted reproductive technology is advancing at fast pace. Increased use of ART (Assisted reproductive technology) is due to changing living standards which involve increased educational and career demand, higher rate of infertility due to poor lifestyle and child conceivement after second marriage. This study gives an overview that how advancing age affects maternal and neonatal outcomes in ART (Assisted reproductive technology). Also it illustrates how other factor like obesity and twin pregnancies complicates the scenario. The studies find an increased rate of preterm birth .gestational hypertension, cesarean delivery chances, high density plasma, Preeclampsia and fetal death at advanced age. The study also shows the combinatorial effects of mother age with number of embryos along with number of good quality embryos which are transferred in ART (Assisted reproductive technology). In advanced age women high clinical and multiple pregnancy rate is achieved by increasing the number along with quality of embryos. Keywords: Reproductive techniques, Fertility, Lifestyle, Preterm delivery, Obesity, Infertility INTRODUCTION Assisted reproductive technology actually involves group of treatments which are used to achieve pregnancy when patients are suffering from issues like infertility or subfertility. The treatments can involve invitro fertilization [IVF], intracytoplasmic sperm injection [ICSI], embryo transfer, egg donation, sperm donation, cryopreservation, etc., [1]. -

Spectrum of Benign Breast Diseases in Females- a 10 Years Study
Original Article Spectrum of Benign Breast Diseases in Females- a 10 years study Ahmed S1, Awal A2 Abstract their life time would have had the sign or symptom of benign breast disease2. Both the physical and specially the The study was conducted to determine the frequency of psychological sufferings of those females should not be various benign breast diseases in female patients, to underestimated and must be taken care of. In fact some analyze the percentage of incidence of benign breast benign breast lesions can be a predisposing risk factor for diseases, the age distribution and their different mode of developing malignancy in later part of life2,3. So it is presentation. This is a prospective cohort study of all female patients visiting a female surgeon with benign essential to recognize and study these lesions in detail to breast problems. The study was conducted at Chittagong identify the high risk group of patients and providing regular Metropolitn Hospital and CSCR hospital in Chittagong surveillance can lead to early detection and management. As over a period of 10 years starting from July 2007 to June the study includes a great number of patients, this may 2017. All female patients visiting with breast problems reflect the spectrum of breast diseases among females in were included in the study. Patients with obvious clinical Bangladesh. features of malignancy or those who on work up were Aims and Objectives diagnosed as carcinoma were excluded from the study. The findings were tabulated in excel sheet and analyzed The objective of the study was to determine the frequency of for the frequency of each lesion, their distribution in various breast diseases in female patients and to analyze the various age group. -

Breastfeeding and Women's Mental Health
BREASTFEEDING AND WOMEN’S MENTAL HEALTH Julie Demetree, MD University of Arizona Department of Psychiatry Disclosures ◦ Nothing to disclose, currently paid by Banner University Medical Center, and on faculty at University of Arizona. Goals and Objectives ◦ Review the basic physiology involved in breastfeeding ◦ Learn about literature available regarding mood, sleep and breastfeeding ◦ Know the resources available to refer to regarding pharmacology and breast feeding ◦ Understand principles of psychopharmacology involved in breastfeeding, including learning about some specific medications, to be able to counsel a woman and obtain informed consent ◦ Be aware of syndrome described as Dysphoric Milk Ejection Reflex Lactation Physiology https://courses.lumenlearning.com/boundless-ap/chapter/lactation/ AAP Material on Breastfeeding AAP: Breastfeeding Your Baby 2015 AAP Material on Breastfeeding AAP: Breastfeeding Your Baby 2015 A Few Numbers ◦ About 80% of US women breastfeed ◦ 10-15% of women suffer from post partum depression or anxiety ◦ 1-2/1000 suffer from post partum psychosis Depression and Infant Care ◦ Depressed mothers are: ◦ More likely to misread infant cues 64 ◦ Less likely to read to infant ◦ Less likely to follow proper safety measures ◦ Less likely to follow preventative care advice 65 Depression is Associated with Decreased Chance of Breastfeeding ◦ A review of 75 articles found “women with depressive symptomatology in the early postpartum period may be at increased risk for negative infant-feeding outcomes including decreased breastfeeding duration, increased breastfeeding difficulties, and decreased levels of breastfeeding self-efficacy.” 1 Depressive Symptoms and Risk of Formula Feeding ◦ An Italian study with 592 mothers participating by completing the Edinburgh Postnatal Depression Scale immediately after delivery and then feeding was assessed at 12-14 weeks where asked if breast, formula or combo feeding. -

Tongue and Lip Ties: Best Evidence June 16, 2015
Tongue and Lip Ties: Best Evidence June 16, 2015 limited elevation in tongue tied baby Tongue and Lip Ties: Best Evidence By: Lee-Ann Grenier Tongue and lip tie (often abbreviated to TT/LT) have become buzzwords among lactation consultants bloggers and new mothers. For many these are strange new words despite the fact that it is a relatively common condition. Treating tongue tie fell out of medical favour in the early 1950s. In breastfeeding circles, it was talked about occasionally, but until recently few health care professionals screened babies for tongue tie and it was frequently overlooked as a cause of common breastfeeding difficulties. In the last few years tongue tie and the related condition lip tie have exploded into the consciousness of mothers and breastfeeding helpers. So why all the fuss about tongue and lip ties all of a sudden? Tongue tie seems to be a relatively common problem, affecting 4-11%1 of the population and it can have a drastic impact on breastfeeding. The presence of tongue tie triples the risk of weaning in the first week of life.2 Here in Alberta it has been challenging to find competent assessment and treatment, prompting several Alberta mothers and their babies to fly to New York in 2011 and 2012 to receive treatment. The dedication and persistence of these mothers has spurred action on providing education and treatment options for Alberta families. In August of 2012, The Breastfeeding Action Committee of Edmonton (BACE) brought Dr. Lawrence Kotlow to Edmonton to provide information and training to area health care providers. -

PLANNED OUT-OF-HOSPITAL BIRTH Approved 11/12/15
HEALTH EVIDENCE REVIEW COMMISSION (HERC) COVERAGE GUIDANCE: PLANNED OUT-OF-HOSPITAL BIRTH Approved 11/12/15 HERC COVERAGE GUIDANCE Planned out-of-hospital (OOH) birth is recommended for coverage for women who do not have high- risk coverage exclusion criteria as outlined below (weak recommendation). This coverage recommendation is based on the performance of appropriate risk assessments1 and the OOH birth attendant’s compliance with the consultation and transfer criteria as outlined below. Planned OOH birth is not recommended for coverage for women who have high risk coverage exclusion criteria as outlined below, or when appropriate risk assessments are not performed, or where the attendant does not comply with the consultation and transfer criteria as outlined below (strong recommendation). High-risk coverage exclusion criteria: Complications in a previous pregnancy: Maternal surgical history Cesarean section or other hysterotomy Uterine rupture Retained placenta requiring surgical removal Fourth-degree laceration without satisfactory functional recovery Maternal medical history Pre-eclampsia requiring preterm birth Eclampsia HELLP syndrome Fetal Unexplained stillbirth/neonatal death or previous death related to intrapartum difficulty Baby with neonatal encephalopathy Placental abruption with adverse outcome Complications of current pregnancy: Maternal Induction of labor Prelabor rupture of membranes > 24 hours 1 Pre-existing chronic hypertension; Pregnancy-induced hypertension with diastolic blood pressure greater than -

Extended Abstract
Extended abstract Effect of intrauterine development and nutritional status on perinatal, intrauterine and neonatal mortality 1 Péter Berkő, 2 Kálmán Joubert, 3 Éva Gárdos, 4 Gyula Gyenis 1Faculty of Healthcare, Miskolc University, BAZ County and University Teaching Hospital Miskolc, Hungary, - 2Demographic Research Institute, Hungarian Central Statistical Office, Budapest, - 3Hungarian Central Statistical Office, Budapest, - 4Department of Biological Anthropology, Faculty of Science, Eötvös Lorand University, Budapest, Hungary At least 50-60% of 3 million of intrauterine and near 4 million deaths that occur worldwide every year are associated with low birth weight, caused by intrauterine growth restriction, preterm delivery, and genetic abnormalities. Fetal growth restriction is the second leading cause of perinatal morbidity and mortality. The authors study to what extent bodily development and nutritional status influence the viability, or perinatal mortality of foetuses and neonates. In the present study the authors describe their novel method, the MDN system (MDN: Maturity, Development, Nutritional status) and its application: 1./ to determine the nutritional status of a neonate on the basis of its gestational age, length and weight development considered simultaneously; - 2./ to differentiate the most viable and the most endangered neonates on the basis of their development and nutritional status; - 3./ to demonstrate the influence of a neonate’s nutritional status by the gestational age on its perinatal mortality. Method – the MDN system The authors have developed a new method, the MDN system (MDN: Maturity, Development, Nutritional status) to determine the weight and length standard positions of neonates in relation to reference standards on the basis of their gestational ages, birth weights and lengths. -

Cervical Insufficiency
Cervical Insufficiency Sonia S. Hassan, MD 1,4 , Roberto Romero, MD 1,2,3 , Francesca Gotsch, MD 5, Lorraine Nikita, RN 1, and Tinnakorn Chaiworapongsa, MD 1,4 1Perinatology Research Branch, Eunice Kennedy Shriver National Institute of Child Health and Human Development/National Institutes of Health/Department of Health and Human Services, Bethesda, MD and Detroit, MI, USA; 2Center for Molecular Medicine and Genetics, Wayne State University, Detroit, Michigan, USA; 3Department of Epidemiology, Michigan State University, East Lansing, Michigan, USA., 4Department of Obstetrics and Gynecology, Wayne State University, Detroit, Michigan, USA, 5Department of Obstetrics and Gynecology Azienda Ospedaliera Universitaria Integrata Verona, Italy 1 Introduction The uterine cervix has a central role in the maintenance of pregnancy and in normal parturition. Preterm cervical ripening may lead to cervical insufficiency or preterm delivery. Moreover, delayed cervical ripening has been implicated in a prolonged latent phase of labor at term. This chapter will review the anatomy and physiology of the uterine cervix during pregnancy and focus on the diagnostic and therapeutic challenges of cervical insufficiency and the role of cerclage in obstetrics. Anatomy The uterus is composed of three parts: corpus, isthmus and cervix. The corpus is the upper segment of the organ and predominantly contains smooth muscle (myometrium). The isthmus lies between the anatomical internal os of the cervix and the histological internal os, and during labor, gives rise to the lower uterine segment. The anatomical internal os refers to the junction between the uterine cavity and the cervical canal, while the histologic internal os is the region where the epithelium changes from endometrial to endocervical.1 The term “fibromuscular junction” was introduced by Danforth, who identified the boundary between the connective tissue of the cervix and the myometrium. -

Nitric Oxide in Human Uterine Cervix: Role in Cervical Ripening
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Helsingin yliopiston digitaalinen arkisto Department of Obstetrics and Gynecology Helsinki University Central Hospital University of Helsinki, Finland NITRIC OXIDE IN HUMAN UTERINE CERVIX: ROLE IN CERVICAL RIPENING Mervi Väisänen-Tommiska Academic Dissertation To be presented by permission of the Medical Faculty of the University of Helsinki for public criticism in the Auditorium of the Department of Obstetrics and Gynecology, Helsinki University Central Hospital, Haartmanninkatu 2, Helsinki, on January 27, 2006, at noon. Helsinki 2006 Supervised by Professor Olavi Ylikorkala, M.D., Ph.D. Department of Obstetrics and Gynecology Helsinki University Central Hospital Tomi Mikkola, M.D., Ph.D. Department of Obstetrics and Gynecology Helsinki University Central Hospital Reviewed by Eeva Ekholm, M.D., Ph.D. Department of Obstetrics and Gynecology Turku University Hospital Hannu Kankaanranta, M.D., Ph.D. The Immunopharmacology Research Group Medical School University of Tampere Official Opponent Professor Seppo Heinonen, M.D., Ph.D. Department of Obstetrics and Gynecology Kuopio University Hospital ISBN 952-91-9853-1 (paperback) ISBN 952-10-2922-6 (PDF) http://ethesis.helsinki.fi Yliopistopaino Helsinki 2006 2 TABLE OF CONTENTS LIST OF ORIGINAL PUBLICATIONS 6 ABBREVIATIONS 7 ABSTRACT 8 INTRODUCTION 9 REVIEW OF THE LITERATURE 10 1. NITRIC OXIDE...................................................................................................................... 10 1.1 SYNTHESIS 10 1.2 AS A MEDIATOR 12 1.3 ASSESSMENT 12 1.4 GENERAL EFFECTS 13 1.5 IN REPRODUCTION 13 2. CERVICAL RIPENING......................................................................................................... 16 2.1 CONTROL 17 2.2 ASSESSMENT 19 2.3 INDUCTION 19 Misoprostol 19 Mifepristone 20 2.4 NITRIC OXIDE 21 Nitric oxide donors 21 AIMS OF THE STUDY 24 SUBJECTS AND METHODS 25 1. -

Clinical, Pathologic and Pharmacologic Correlations 2004
HUMAN REPRODUCTION: CLINICAL, PATHOLOGIC AND PHARMACOLOGIC CORRELATIONS 2004 Course Co-Director Kirtly Parker Jones, M.D. Professor Vice Chair for Educational Affairs Department of Obstetrics and Gynecology Course Co-Director C. Matthew Peterson, M.D. Professor and Chief Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology 1 Welcome to the course on Human Reproduction. This syllabus has been recently revised to incorporate the most recent information available and to insure success on national qualifying examinations. This course is designed to be used in conjunction with our website which has interactive materials, visual displays and practice tests to assist your endeavors to master the material. Group discussions are provided to allow in-depth coverage. We encourage you to attend these sessions. For those of you who are web learners, please visit our web site that has case studies, clinical/pathological correlations, and test questions. http://medstat.med.utah.edu/kw/human_reprod 2 TABLE OF CONTENTS Page Lectures/Examination................................................................................................................................... 4 Schedule........................................................................................................................................................ 5 Faculty .......................................................................................................................................................... 8 Groups ......................................................................................................................................................... -

Quinacrine Sterilization Induce Cryptomenorrhoea: a Rare Complication
JMSCR Volume||2||Issue||4||Pages 726-729||April 2014 2014 www.jmscr.igmpublication.org Impact Factcor-1.1147 ISSN (e)-2347-176x Quinacrine Sterilization Induce Cryptomenorrhoea: A Rare Complication Authors Brig Kumar Praveen MD (Gynae) *, Gp Capt JC Sharma MD (Gynae)1, Dr Rupa Talukdar , MD (Gynae )2 *Consultant (Obs & Gynae) Base Hospital Lucknow 1Associate prof ( Obs & Gyn) Army college of medical sciences Delhi Cantt. 2 Senior Gynaecologist , cantonment general hospital, Delhi Cantt. Email: [email protected] Abstract- Quinacrine was used as a non-surgical technique for permanent sterilization was been under study several years back . It was used and propagated by several resource poor countries to control population . It was relatively inexpensive and had mass acceptability due to similarity in procedure of IUCD insertion.. The side effects of this sterilization process have been reported to be low as compared to surgical methods. Menstrual abnormalities in the form of menorrhagia and ammenorrhoea have been reported but cryptomenorrhea was very uncommon complication. Here we present a case of quinacrin induced crypyomenorrhoea in a young women. Keywords: quinacrine, cryptomenorrhoea, trans cervical sterilization, heamatometra. INTRODUCTION population. It was relatively inexpensive and had Quinacrine was used as a non-surgical technique mass acceptability due to similarity in procedure for permanent sterilization was been under study of IUCD insertion.. The side effects of this several years back . It was used and propagated sterilization process have been reported to be low by several resource poor countries to control as compared to surgical methods. Menstrual Brig Kumar Praveen et al JMSCR Volume 2 Issue 4 April 2014 Page 726 JMSCR Volume||2||Issue||4||Pages 726-729||April 2014 2014 abnormalities in the form of menorrhagia and About100 ml of collected altered blood was ammenorrhoea have been reported but drained and sent for culture and sensitivity.(Fig 1). -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
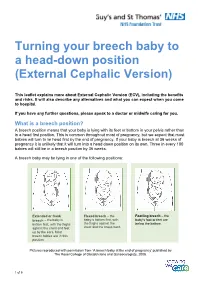
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus).