RECORD of INVESTIGATION INTO DEATH Ref No: 42/13
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Register of Authorised Hospitals in Western Australia
Register of Authorised Hospitals in Western Australia Mental Health Act 2014 Section 542 Correct as of 4 August 2020 (OCP23859) www.chiefpsychiatrist.wa.gov.au Introduction Section 542 of the Mental Health Act 2014 provides for the Governor, by order published in the Western Australian Government Gazette to authorise a public hospital or part of a public hospital to be an ‘authorised hospital’ for the purposes of reception and admission of patients requiring involuntary treatment and care. Section 541 provides for a private hospital whose license is endorsed under section 26DA(2) of the Hospitals and Health Services Act 1927 to be an ‘authorised hospital’ on the recommendation by/of the Chief Psychiatrist, for the reception and admission of patients requiring involuntary treatment and care. Please Note: Grant of Leave under section 105(1)(a)(ii) of the Mental Health Act 2014 from an Authorised part of a Hospital to a Non-Authorised part of a Hospital Subdivision 2 of Division 6 of Part 7 of the Mental Health Act 2014 provides for the granting of leave for an involuntary detained patient from an authorised hospital. Section 105 (1)(a)(ii) provides specifically for leave to be granted to a General Hospital for a patient who requires medical or surgical treatment or treatment likely to benefit the inpatient’s physical health in some other way. When an authorised hospital is within a general hospital campus and an involuntary inpatient needs to be treated in the general part of the hospital it is as though it is leave being granted from the authorised facility to the general hospital, despite the fact that both hospitals (authorised and general) are within the same grounds. -
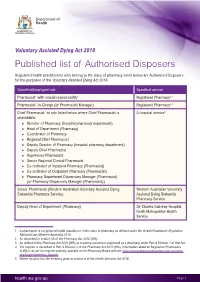
Published List of Authorised Disposers
Voluntary Assisted Dying Act 2019 Published list of Authorised Disposers Registered health practitioners who belong to the class of pharmacy listed below are Authorised Disposers for the purposes of the Voluntary Assisted Dying Act 2019. Specified/Employed role Specified service Pharmacist1 with overall responsibility2 Registered Pharmacy3,4 Pharmacist1-in-Charge (or Pharmacist Manager) Registered Pharmacy3,4 Chief Pharmacist1 or role listed below where Chief Pharmacist is A hospital service5 unavailable: * Director of Pharmacy (hospital pharmacy department) * Head of Department (Pharmacy) * Coordinator of Pharmacy * Regional Chief Pharmacist * Deputy Director of Pharmacy (hospital pharmacy department) * Deputy Chief Pharmacist * Supervisor Pharmacist * Senior Regional Clinical Pharmacist * Co-ordinator of Inpatient Pharmacy (Pharmacist) * Co-ordinator of Outpatient Pharmacy (Pharmacist) * Pharmacy Department Dispensary Manager (Pharmacist) (or Pharmacy Dispensary Manager (Pharmacist)) Senior Pharmacist (Western Australian Voluntary Assisted Dying Western Australian Voluntary Statewide Pharmacy Service) Assisted Dying Statewide Pharmacy Service Deputy Head of Department (Pharmacy) Sir Charles Gairdner Hospital, North Metropolitan Health Service 1 A pharmacist is a registered health practitioner in the class of pharmacy as defined under the Health Practitioner Regulation National Law (Western Australia) 2010 2 As described in section 56 of the Pharmacy Act 2010 (WA) 3 As defined in the Pharmacy Act 2010 (WA) as meaning a premises registered -
Inquest Finding (PDF)
Coroners Act 1996 [Section 26(1)] Western Australia RECORD OF INVESTIGATION INTO DEATH Ref No: 12/19 I, Michael Andrew Gliddon Jenkin, Coroner, having investigated the death of Lorna May WOODS with an inquest held at Perth Coroner’s Court, Court 85, CLC Building, 501 Hay Street, Perth, on 6 March 2019 find that the identity of the deceased person was Lorna May WOODS and that death occurred on 10 January 2017 at Joondalup Health Campus, from pulmonary thromboembolism due to deep vein thrombosis and sepsis due to pyelonephritis on a background of metastatic ovarian cancer in the following circumstances:- Counsel Appearing: Mr D Jones assisted the Coroner Mr Mark Williams (MinterEllison) appeared on behalf of Joondalup Health Campus, Dr P Grolman and Dr C Singam Table of Contents INTRODUCTION ............................................................................................................ 2 THE DECEASED .............................................................................................................. 3 Background ....................................................................................................... 3 Offending history .............................................................................................. 4 Overview of Medical Conditions ...................................................................... 4 DECEASED’S ADMISSION 7 - 8 JANUARY 2017 ............................................................. 6 PLACING THE DECEASED ON A TREATMENT ORDER ................................................... -

Resident Medical Officer Streams
Royal Perth Bentley Group Resident Medical Officer Streams Accelerate your career with Royal Perth Bentley Group (RPBG) With an established international reputation for contribution to healthcare, training and research as well as the provision of extensive, tailored career opportunities, RPBG provides an ideal launch pad for your career in the medical profession. RPBG is keenly invested in the personal and professional progression of its staff and their engagement in strategic organisational decisions. With support and active engagement from the medical wellbeing program and peer support services, as well as tailored streams of clinical rotations that provide JMOs with the necessary skills and experience to pursue their desired Key reasons you should career pathway. work for RPBG The streams in the Resident Medical Officer Defined streams of medical rotations tailored program are outlined overleaf, covering rotations to provide doctors with the necessary skills at Royal Perth Hospital, Bentley Health Service, and experience to progress down intended Armadale Health Service, Kalgoorlie Hospital, career pathways. Bunbury Regional Hospital and Hedland Health Expanding medical wellbeing program and Campus, and specialised rotations within the peer support systems. Perth Metropolitan area (SJOG Midland Hospital, Mount Hospital, Perth Children’s Hospital and Opportunities for rotation variations including Joondalup Health Campus). Service Improvement, Perioperative, Anaesthetic ED, Silver Chain and CRP rural rotations. Supportive of part–time/flexible training arrangement negotiations. Doctors have the opportunity to be engaged with the Hospital Executive and Area Board through an active JMO Liasion Committee. More information Postgraduate Medical Education: 9224 7091 Medical Workforce (Recruitment): 9224 1693 MEDICAL STREAM In the medical rotation you will get between one and three terms in an acute/general medicine ward (combination of RPH AMU, AHS General Medicine and SJOG Midland, Medicine Unit), as well as one leave relief or after hours term. -

There Will Be 14 Authorised Mental Health Beds in Broome Regional Resource Centre
US Ie STANDING COMMITTEE ON ESTIMATES AND FINANCIAL OPERATIONS QUESTIONS RELATING TO 2008/09 ONGOING BUDGET ESTIMATES DEPARTMENT OF HEALTH 1. HON. HELEN MORTON MLC ASKED- Page 556 1.1 How many mental health beds will be built in the Broome Regional Resource Centre, and how many will be secured beds? Answer: (1) There will be 14 authorised mental health beds in Broome Regional Resource Centre. (2) There will be three secure beds at Broome Regional Resource Centre. 1.2 What is the Broome Regional Resource Centre, and what will it comprise? Answer: The policy framework for country health services involves a regional network model, based on the concepts of service integration and strategic partnership. The regional network model has five interrelated elements, as follows: Regional Resource Centres. Integrated district health services. Health services for towns. Health services for small communities/settlements. Partner metropolitan health service(s). As the largest town in the Kimberley region, Broome has been identified as the most appropriate town for the regional resource centre. As such, it will provide services and support for the following resident specialist and regional health care programs for the Kimberley: Aged care/rehabilitation. Anaesthetics/high dependency. Dental health. Emergency. General medicine. General surgery. Visiting specialist surgery. Medical imaging. Mental health. Obstetrics. Paediatric. Population health. Estimates and Financial Operations Committee Page 2 1.3 What specific initiatives will the $12.5 million for the redevelopment stage 2 of Kalamunda Hospital be spent on from 2009 until 2013. Answer: Planning for Stage 2 of the Kalamunda Hospital redevelopment has not commenced. Funding of $3.2M has been allocated to the refurbishment of the theatres at Kalamunda Hospital. -

Research Proposal Has Been Approved
The University of Notre Dame Australia ResearchOnline@ND Theses 2016 An investigation of nurse education service models in acute care metropolitan hospitals across Australia Carolyn Keane The University of Notre Dame Australia Follow this and additional works at: http://researchonline.nd.edu.au/theses Part of the Nursing Commons COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING The am terial in this communication may be subject to copyright under the Act. Any further copying or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice. Publication Details Keane, C. (2016). An investigation of nurse education service models in acute care metropolitan hospitals across Australia (Doctor of Nursing). University of Notre Dame Australia. http://researchonline.nd.edu.au/theses/138 This dissertation/thesis is brought to you by ResearchOnline@ND. It has been accepted for inclusion in Theses by an authorized administrator of ResearchOnline@ND. For more information, please contact [email protected]. Appendices Appendix 1. National Safety and Quality Health Service Standards 276 Appendix 2: UNDA Ethics Approval Letter 277 Appendix 3: SMHS Nursing Research Review Committee Approval Letter Government of Western Australia Department of Health Fremantle Hospital and Health Service 3rd February 2014 Carolyn Keane A/Nursing Director, Corporate Services Fremantle Hospital Professional Doctorate in Nursing student, University of Notre Dame Australia. Professor Selma Alliex Dean of the school of nursing University of Notre Dame Australia. Dear Carolyn and Dr Alliex Project title: An Investigation of Nurse Education Services Models in Acute Care Metropolitan Hospitals across Australia. Thankyou for submitting the above project for review by the South Metro Health Service (SMHS) Nursing Research Review Committee. -

Cancer Care Closer to Home May 2016
Cancer care closer to home May 2016 WA Health has strongly invested in cancer care to support the 11,700 Western Australians diagnosed with cancer every year. The recent opening of Fiona Stanley Hospital and St John of God Midland Public Hospital ensure patients have access to excellent cancer care no matter where they live in the metropolitan area. These services are complemented by existing services at the Comprehensive Cancer Centre at Sir Charles Gairdner Hospital, Royal Perth Hospital, Rockingham General Hospital and Joondalup Health Campus with specialist cancer care at Princess Margaret Hospital and King Edward Memorial Hospital. Fiona Stanley Hospital (FSH) also houses a Comprehensive Cancer Centre which includes 22 consulting/interview rooms for cancer outpatients, a chemotherapy unit, a day therapy unit, a radiation oncology suite, radiation therapy planning and a breast assessment centre. The Cancer Centre has been developed around a private courtyard and features a separate entrance and drop-off area to improve privacy and access for patients and their visitors. What treatment can patients expect? With 80 per cent of FSH's cancer patients treated as outpatients, the cancer service has taken a multidisciplinary approach to treatment. This means several specialties work together, including physicians, radiology, pathology, radiation, medical oncology, nursing, counselling, family support services, and allied health. Patients also have access to services such as physiotherapy, clinical psychology, occupational therapy, social work, pharmacy, dietetics and speech pathology, all in one location. 1 Patients receiving targeted radiation therapies benefit from greatly reduced waiting times and faster treatment with state- of-the- art equipment such as the latest in linear accelerator (linac) technology. -
Western Australia Emergency Access Target Performance Monthly Report
Western Australia Emergency Access Target Performance Monthly Report February 2019 health.wa.gov.au February 2019 | Western Australia Emergency Access Target Performance Monthly Report What is the WA Emergency Access Target (WEAT)? In February 2016, WA Health system established the WA Emergency Access Target (WEAT) to continue to drive local improvement in patient access to emergency services. This replaced the National Emergency Access Target (NEAT) following the expiry of the Commonwealth National Partnership Agreement on Improving Public Hospital Services in 2015. The WEAT requires 90 per cent of all patients presenting to a hospital emergency department (ED) to be seen and admitted, transferred or discharged within four hours. What hospitals does it cover? Child and Adolescent Health Service (CAHS): Perth Children’s Hospital and Princess Margaret Hospital. East Metropolitan Health Service (EMHS): Royal Perth Hospital, Armadale Health Service and St John of God Midland Public Hospital. North Metropolitan Health Service (NMHS): Sir Charles Gairdner Hospital, King Edward Memorial Hospital and Joondalup Health Campus. South Metropolitan Health Service (SMHS): Fiona Stanley Hospital, Rockingham General Hospital and Peel Health Campus. WA Country Health Service (WACHS): Albany Hospital, Broome Hospital, Bunbury Hospital, Busselton Hospital, Carnarvon Hospital, Derby Hospital, Esperance Hospital, Geraldton Hospital, Hedland Health Campus, Kalgoorlie Hospital, Karratha Health Campus, Kununurra Hospital, Narrogin Hospital and Northam Hospital. Providing the best care All hospitals and Health Service Providers (HSPs) continue to examine and improve processes across the entire patient journey, from ED and the wards through to hospital discharge. In 2017–18, Western Australia was the best performing state for patients treated and admitted, transferred or discharged within four hours. -

LA QON 1238 Tabled Paper Table 1: Number of Obstetric-Related
LA QON 1238 Tabled Paper Table 1: Number of obstetric-related separations that occurred in WA public hospitals between 1 January 2017 and 28 February 2017 (inclusive), by hospital. Number of Obstetric- Hospital related separations Albany Hospital 138 Armadale-Kelmscott Memorial Hospital 448 Bentley Hospital 161 Bridgetown Hospital < 5 Broome Hospital 100 Bunbury Hospital 286 Busselton Hospital 67 Carnarvon Hospital 14 Collie Hospital 18 Derby Hospital 33 Esperance Hospital 52 Exmouth Hospital < 5 Fiona Stanley Hospital 692 Fitzroy Crossing Hospital 7 Fremantle Hospital < 5 Geraldton Hospital 120 Graylands Hospital < 5 Halls Creek Hospital 5 Hedland Health Campus 109 Joondalup Health Campus (public patients) 634 Kalgoorlie Hospital 182 Katanning Hospital 5 Kellerberrin Hospital < 5 King Edward Memorial Hospital 1364 Kununurra Hospital 27 Margaret River Hospital 38 Meekatharra Hospital < 5 Merredin Hospital < 5 Moora Hospital < 5 Narrogin Hospital 23 Newman Hospital < 5 Next Step Drug and Alcohol Services, East Perth < 5 Nickol Bay Karratha Hospital 70 Norseman Hospital < 5 Northam Hospital < 5 Onslow Hospital < 5 Osborne Park Hospital 274 Peel Heel Campus (public patients) 258 Rockingham General Hospital 368 Royal Perth Hospital 23 Sir Charles Gairdner Hospital 26 Sir Charles Gairdner Hospital Mental Health Services < 5 St John Of God Midland (public patients) 404 Tom Price Hospital < 5 Warren Manjimup Hospital < 5 Total 5974 Page 1 of 4 LA QON 1238 Tabled Paper Table 2: Number of babies born at Western Australian public hospitals between -

Who Can Make a Complaint Or Provide Feedback?
How to make a complaint in the WA Health System Carly Parry- Advocacy Manager In the WA Health System, anyone can make a complaint or provide feedback, including…….. • Consumers • Families • Carers • Visitors Making a complaint, which option is right for you? Direct to The Health Service If you wish to comment on, compliment or complain about, any service received in a hospital or health service, you might want to first raise your concerns with the attending staff, either verbally or in writing. If you want the service to provide you with a response, you can request this. You can ask the service to provide their response to you verbally and/or in writing. When providing feedback or making a complaint, let the service know if you are seeking a specific resolution/outcome. Resolution for you might be…. • An apology • A change to a service’s processes • A reimbursement or refund • A second medical opinion WA Hospitals and Public Health Services….. Each WA Public Health Service & Hospital has an internal department that manages complaints and feedback. These departments are often referred to as a Family, Patient or Consumer Liaison/ Experience Service. You can contact a hospital’s main switchboard and ask to be transferred to the Patient Liaison Office. You can make a complaint over the phone or in writing. WA Health (Public) Services, must follow the “Complaints Management Policy.” Under this policy, a health service should; • Aim to provide a response to you within 30 working days. If they need more time, they should let you know at 15 day intervals. -

The Wellbeing Guide Collated for Wa Junior Doctors
P M C W A / / J M O F O R U M / / 2 0 2 1 THE WELLBEING GUIDE COLLATED FOR WA JUNIOR DOCTORS BY POSTGRADUATE MEDICAL COUNCIL OF WA WITH ASSISTANCE FROM DR YASMIN SOLIMAN, DR GREER JALLAND, DR AMY KELLIHER AND DR SHANNON MARANTELLI GPO BUILDING, Level 3, 3 Forrest Place, PERTH WA 6000 PO Box 8172 Perth Business Centre WA 6849 T: (08) 6373 2302 E: [email protected] W: www.pmcwa.org.au www.facebook.com/PMCWA For further copies of this document, please visit the PMCWA website Front cover photo submission: Dr Joanna Chua DISCLAIMER The information contained in this document is for general information only. It is not designed to take the place of professional advice based on individual situations. We urge you to seek assistance from your local doctor or one of the listed support groups. A health and wellbeing reference for WA JMOs Page 2 PLAYING GOD BY G.COLQUHOUN (1) Today I do not want to be a doctor. Today I want to be a doctor. Today I do not want to be a doctor. Today I am happy to be a doctor. No one is getting any better. Everyone seems to be getting better. Those who were well are sick again. And those Those who were sick are not so sick. And those who were sick are sicker. who were well are thriving. The dying think that they will live. And the The healthy are grateful to be alive. And the healthy think they are dying. dying are at peace with their dying. -

A Review of Emergency Mental Health Services in North Metropolitan Perth
A Review of Emergency Mental Health Services in North Metropolitan Perth ntal Health Policy Research Geoff Smith Theresa Williams Linley Lefay Western Centre Australian for Me February 2010 Western Australian Centre for Mental Health Policy Research Graylands Hospital Brockway Road Mt Claremont Western Australia 6010 Phone: (08) 9347 6842 Email: graylandsmhpresearcHITHealth.wa.gov.au Suggested Citation: Smith, G, Williams, T and Lefay, L. (2010). A Review of Emergency Mental Health Services in Metropolitan Perth. Department of Health, Perth. This document can be accessed on http://www.health.wa.gov.au/mhpr The opinions expressed in this report are those of the authors and are not necessarily those of the Department of Health. © Department of Health 2010 2 A Review of Emergency Mental Health Services in North Metropolitan Perth February 2010 ACKNOWLEDGEMENTS Many people have participated in this project and the reviewers would like to thank them. We particularly wish to acknowledge the contributions of: Consumers, their carers and service providers who generously gave up their time to be interviewed and to attend the consultation workshops; Reference Group members who provided advice and guidance throughout the project; Mr Tom Pinder and Ms Crystal O’Connor, Health Information Division, Department of Health for providing data; and Ms Leanne Sultan, A/Director of Operations and Dr Willem van Wyk, Clinical Director Adult Mental Health for their leadership and commitment to the Review. A valuable part of the Review was the opportunity to visit two other State jurisdictions to learn from their experience. The reviewers are grateful for the generosity of a number of clinicians in Melbourne and Sydney who allowed us visit to their services and arranged meetings with a wide range of staff.