Prescribing Information | VELCADE® (Bortezomib)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Phase II Study of the Novel Proteasome Inhibitor Bortezomib In
Memorial Sloan-Kettering Cance r Center IRB Protocol IRB#: 05-103 A(14) A Phase II Study of the Novel Proteas ome Inhibitor Bortezomib in Combination with Rituximab, Cyclophosphamide and Prednisone in Patients with Relapsed/Refractory I Indolent B-cell Lymphoproliferative Disorders and Mantle Cell Lymphoma (MCL) MSKCC THERAPEUTIC/DIAGNOSTIC PROTOCOL Principal Investigator: John Gerecitano, M.D., Ph.D. Co-Principal Carol Portlock, M.D. Investigator(s): IFormerly: A Phase I/II Study of the Nove l Proteasome Inhibitor Bortezomib in Combinati on with Rituximab, Cyclophosphamide and Prednisone in Patients with Relapsed/Refractory Indolent B-cell Lymphoproliferative Disorders and Mantle Cell Lymphoma (MCL) Amended: 07/25/12 Memorial Sloan-Kettering Cance r Center IRB Protocol IRB#: 05-103 A(14) Investigator(s): Paul Hamlin, M.D. Commack, NY Steven B. Horwitz, M.D. Philip Schulman, M.D. Alison Moskowitz, M.D. Stuart Lichtman, M.D Craig H. Moskowitz, M.D. Stefan Berger, M.D. Ariela Noy, M.D. Julie Fasano, M.D. M. Lia Palomba, M.D., Ph.D. John Fiore, M.D. Jonathan Schatz, M.D. Steven Sugarman, M.D David Straus, M.D. Frank Y. Tsai, M.D. Andrew D. Zelenetz, M.D., Ph.D. Matthew Matasar, M.D Rockville Center, NY Mark L. Heaney, M.D., Ph.D. Pamela Drullinksy, M.D Nicole Lamanna, M.D. Arlyn Apollo, M.D. Zoe Goldberg, M.D. Radiology Kenneth Ng, M.D. Otilia Dumitrescu, M.D. Tiffany Troso-Sandoval, M.D. Andrei Holodny, M.D. Sleepy Hollow, NY Nuclear Medicine Philip Caron, M.D. Heiko Schoder, M.D. Michelle Boyar, M.D. -

Treatment of Localized Extranodal NK/T Cell Lymphoma, Nasal Type: a Systematic Review Seok Jin Kim†, Sang Eun Yoon† and Won Seog Kim*
Kim et al. Journal of Hematology & Oncology (2018) 11:140 https://doi.org/10.1186/s13045-018-0687-0 REVIEW Open Access Treatment of localized extranodal NK/T cell lymphoma, nasal type: a systematic review Seok Jin Kim†, Sang Eun Yoon† and Won Seog Kim* Abstract Extranodal natural killer/T cell lymphoma (ENKTL), nasal type, presents predominantly as a localized disease involving the nasal cavity and adjacent sites, and the treatment of localized nasal ENKTL is a major issue. However, given its rarity, there is no standard therapy based on randomized controlled trials and therefore a lack of consensus on the treatment of localized nasal ENKTL. Currently recommended treatments are based mainly on the results of phase II studies and retrospective analyses. Because the previous outcomes of anthracycline-containing chemotherapy were poor, non- anthracycline-based chemotherapy regimens, including etoposide and L-asparaginase, have been used mainly for patients with localized nasal ENKTL. Radiotherapy also has been used as a main component of treatment because it can produce a rapid response. Accordingly, the combined approach of non-anthracycline-based chemotherapy with radiotherapy is currently recommended as a first-line treatment for localized nasal ENKTL. This review summarizes the different approaches for the use of non-anthracycline-based chemotherapy with radiotherapy including concurrent, sequential, and sandwich chemoradiotherapy, which have been proposed as a first-line treatment for newly diagnosed patients with localized nasal ENKTL. Keywords: Extranodal NK/T cell lymphoma, Chemoradiotherapy, Localized disease Background Treatment for newly diagnosed patients with localized Extranodal natural killer/T cell lymphoma (ENKTL), nasal nasal ENKTL type, is a rare subtype of non-Hodgkin lymphoma [1]. -
VELCADE® (Bortezomib) for Injection
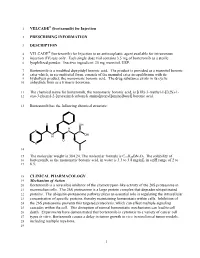
1 VELCADE® (bortezomib) for Injection 2 PRESCRIBING INFORMATION 3 DESCRIPTION 4 VELCADE® (bortezomib) for Injection is an antineoplastic agent available for intravenous 5 injection (IV) use only. Each single dose vial contains 3.5 mg of bortezomib as a sterile 6 lyophilized powder. Inactive ingredient: 35 mg mannitol, USP. 7 Bortezomib is a modified dipeptidyl boronic acid. The product is provided as a mannitol boronic 8 ester which, in reconstituted form, consists of the mannitol ester in equilibrium with its 9 hydrolysis product, the monomeric boronic acid. The drug substance exists in its cyclic 10 anhydride form as a trimeric boroxine. 11 The chemical name for bortezomib, the monomeric boronic acid, is [(1R)-3-methyl-1-[[(2S)-1- 12 oxo-3-phenyl-2-[(pyrazinylcarbonyl) amino]propyl]amino]butyl] boronic acid. 13 Bortezomib has the following chemical structure: O OH H N N B N OH H O N 14 15 The molecular weight is 384.24. The molecular formula is C19H25BN4O4. The solubility of 16 bortezomib, as the monomeric boronic acid, in water is 3.3 to 3.8 mg/mL in a pH range of 2 to 17 6.5. 18 CLINICAL PHARMACOLOGY 19 Mechanism of Action 20 Bortezomib is a reversible inhibitor of the chymotrypsin-like activity of the 26S proteasome in 21 mammalian cells. The 26S proteasome is a large protein complex that degrades ubiquitinated 22 proteins. The ubiquitin-proteasome pathway plays an essential role in regulating the intracellular 23 concentration of specific proteins, thereby maintaining homeostasis within cells. Inhibition of 24 the 26S proteasome prevents this targeted proteolysis, which can affect multiple signaling 25 cascades within the cell. -

PPE Requirements Hazardous Drug Handling
This document’s purpose is only to provide general guidance. It is not a definitive interpretation for how to comply with DOSH requirements. Consult the actual NIOSH hazardous drugs list and program regulations in entirety to understand all specific compliance requirements. Minimum PPE Required Minimum PPE Required Universal (Green) - handling and disposed of using normal precautions. PPE Requirements High (Red) - double gloves, gown, eye and face protection in Low (Yellow) - handle at all times with gloves and appropriate engineering Hazardous Drug Handling addition to any necessary controls. engineering controls. Moderate (Orange) -handle at all times with gloves, gown, eye and face protection (with splash potential) and appropirate engineering controls. Tablet Open Capsule Handling only - Contained Crush/Split No alteration Crush/Split Dispensed/Common Drug Name Other Drug Name Additional Information (Formulation) and (NIOSH CATEGORY #) Minimum PPE Minimum PPE Minimum PPE Minimum PPE Required required required required abacavir (susp) (2) ziagen/epzicom/trizivir Low abacavir (tablet) (2) ziagen/epzicom/trizivir Universal Low Moderate acitretin (capsule) (3) soriatane Universal Moderate anastrazole (tablet) (1) arimidex Low Moderate High android (capsule) (3) methyltestosterone Universal Moderate apomorphine (inj sq) (2) apomorphine Moderate arthotec/cytotec (tablet) (3) diclofenac/misoprostol Universal Low Moderate astagraf XL (capsule) (2) tacrolimus Universal do not open avordart (capsule) (3) dutasteride Universal Moderate azathioprine -

Handling of Hazardous Drugs Risk Prevention by Personal Protective Equipment Handling of Hazardous Drugs
HANDLING OF HAZARDOUS DRUGS RISK PREVENTION BY PERSONAL PROTECTIVE EQUIPMENT HANDLING OF HAZARDOUS DRUGS INTRODUCTION CONTENT The expression “antineoplastic drug” (ANPD) is often used synonymously together with “cytostatics” or Introduction 2 “chemotherapeutics”, however, these terms normally Definition of Risks 4 describe an overarching category to which other drug- classes belong. These types of drugs belong to drug- Causes for Risks 10 specialties summarized under the term “Hazardous Consequences 14 Drugs”, according to the CDC’s (Centers for Disease Control and Prevention) NIOSH4 alert in 2004. The Preventive Strategies 16 term ANPD describes in general the activity of these Risk Prevention 26 drugs against a neoplasm, characterizing an abnormal growth of tissue. In a recent systematic review and Literature 28 meta-analysis of the literature5 the expression “ANPD” Mandatory Information 31 is used in a general manner, therefore it is applied in this review, too. INTRODUCTION Antineoplastic drugs (ANPD) have been introduced ANPDs represent a broad and non-homogenous group for cancer treatment since the 1940s. More than of chemicals with a variety of structures, origins, ac- 12 million patients are treated with ANPDs each tivities and effects at the cellular level. They are cate- year. Nowadays the number of cancer diagnoses gorized according to their specific potential of toxicity is continuously increasing. or to their mechanisms of action, described in more detail in the chapter “Definition of risks”. Currently, the This brochure addresses the hazardous effects of anti- list encompassing ANPDs used in daily clinical practice neoplastic drugs, the importance of risk assessment contains more than 115 special drugs1. and standard precautions of personal protection as recommended by the 2004-NIOSH (National Institute During the 1970’s first concerns with respect to toxic for Occupational Safety and Health)-Alert and corre- side effects were raised further to cases that had been 1, 2, 3 sponding updates in 2010 / 2012 and 2016. -

Ciera L. Patzke, Alison P. Duffy, Vu H. Duong, Firas El Chaer 4, James A
Journal of Clinical Medicine Article Comparison of High-Dose Cytarabine, Mitoxantrone, and Pegaspargase (HAM-pegA) to High-Dose Cytarabine, Mitoxantrone, Cladribine, and Filgrastim (CLAG-M) as First-Line Salvage Cytotoxic Chemotherapy for Relapsed/Refractory Acute Myeloid Leukemia Ciera L. Patzke 1, Alison P. Duffy 1,2, Vu H. Duong 1,3, Firas El Chaer 4, James A. Trovato 2, Maria R. Baer 1,3, Søren M. Bentzen 1,3 and Ashkan Emadi 1,3,* 1 Greenebaum Comprehensive Cancer Center, University of Maryland, Baltimore, MD 21201, USA; [email protected] (C.L.P.); aduff[email protected] (A.P.D.); [email protected] (V.H.D.); [email protected] (M.R.B.); [email protected] (S.M.B.) 2 School of Pharmacy, University of Maryland, Baltimore, MD 21201, USA; [email protected] 3 School of Medicine, University of Maryland, Baltimore, MD 21201, USA 4 School of Medicine, University of Virginia, Charlottesville, VA 22908, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-410-328-2596 Received: 10 January 2020; Accepted: 13 February 2020; Published: 16 February 2020 Abstract: Currently, no standard of care exists for the treatment of relapsed or refractory acute myeloid leukemia (AML). We present our institutional experience with using either CLAG-M or HAM-pegA, a novel regimen that includes pegaspargase. This is a retrospective comparison of 34 patients receiving CLAG-M and 10 receiving HAM-pegA as first salvage cytotoxic chemotherapy in the relapsed or refractory setting. Composite complete response rates were 47.1% for CLAG-M and 90% for HAM-pegA (p = 0.027). -

Characterization and Separation of Platinum-Based Antineoplastic
separations Article Characterization and Separation of Platinum-Based Antineoplastic Drugs by Zwitterionic Hydrophilic Interaction Liquid Chromatography (HILIC)–Tandem Mass Spectrometry, and Its Application in Surface Wipe Sampling Stefano Dugheri 1,* , Nicola Mucci 2 , Enrico Mini 3, Donato Squillaci 2 , Giorgio Marrubini 4 , Gianluca Bartolucci 5 , Elisabetta Bucaletti 2, Giovanni Cappelli 2, Lucia Trevisani 2 and Giulio Arcangeli 2 1 Industrial Hygiene and Toxicology Laboratory, Occupational Medicine Unit, Careggi University Hospital, 50134 Florence, Italy 2 Department of Experimental and Clinical Medicine, University of Florence, 50134 Florence, Italy; nicola.mucci@unifi.it (N.M.); donato.squillaci@unifi.it (D.S.); elisabetta.bucaletti@unifi.it (E.B.); giovanni.cappelli@unifi.it (G.C.); lucia.trevisani@unifi.it (L.T.); giulio.arcangeli@unifi.it (G.A.) 3 Department of Health Sciences, University of Florence, 50134 Florence, Italy; enrico.mini@unifi.it 4 Department of Drug Sciences, University of Pavia, Via Taramelli 12, 27100 Pavia, Italy; [email protected] 5 Department of Neurosciences, Psychology, Drug Research and Child Health, University of Florence, 50019 Sesto Fiorentino, Italy; gianluca.bartolucci@unifi.it Citation: Dugheri, S.; Mucci, N.; * Correspondence: stefano.dugheri@unifi.it Mini, E.; Squillaci, D.; Marrubini, G.; Bartolucci, G.; Bucaletti, E.; Cappelli, Abstract: Platinum-based antineoplastic drugs (PtADs) are among the most important and used G.; Trevisani, L.; Arcangeli, G. families of chemotherapy drugs, which, -

Combining Milatuzumab with Bortezomib, Doxorubicin, Or Dexamethasone Improves Responses in Multiple Myeloma Cell Lines Rhona Stein,1Mitchell R
CancerTherapy: Preclinical Combining Milatuzumab with Bortezomib, Doxorubicin, or Dexamethasone Improves Responses in Multiple Myeloma Cell Lines Rhona Stein,1Mitchell R. Smith,2 Susan Chen,1Maria Zalath,1and David M. Goldenberg1 Abstract Purpose: The humanized anti-CD74 monoclonal antibody, milatuzumab, is in clinical evaluation for the therapy of multiple myeloma (MM). The ability of milatuzumab to increase the efficacy of bortezomib, doxorubicin, and dexamethasone was examined in three human CD74+ MM cell lines, CAG, KMS11, KMS12-PE, and one CD74-MM cell line, OPM-2. Experimental Design: Activity of milatuzumab as a monotherapy and combined with the drugs was evaluated by studying in vitro cytotoxicity, signaling and apoptotic pathways, and in vivo therapeutic activity in severe combined immunodeficient (SCID) mouse models of MM. Results: Given as a monotherapy, cross-linked milatuzumab, but not milatuzumab alone, yielded sig- nificant antiproliferative effects in CD74+ cells.The combination of cross-linked milatuzumab with bortezomib, doxorubicin, or dexamethasone caused more growth inhibition than either cross-linked milatuzumab or drug alone, producing significant reductions in the IC50 of the drugs when combined. Efficacy of combined treatments was accompanied by increased levels of apoptosis measured by increases of activated caspase-3 and hypodiploid DNA. Both milatuzumab and bortezomib affect the nuclear factor-nB pathwayinCAGMMcells. In CAG-or KMS11-SCIDxenograftmodels ofdisseminated MM, milatuzumab more than doubled median survival time, compared withup to a 33% increase in median survival withbortezomib but no significant benefit with doxorubicin. Moreover, combining milatuzumabandbortezomibincreasedsurvivalsignificantlycomparedwitheither treatmentalone. Conclusions:The therapeutic efficacies of bortezomib, doxorubicin, and dexamethasone are en- hanced in MM cell lines when given in combination with milatuzumab, suggesting testing these combinations clinically. -

ASHP Guidelines on Handling Hazardous Drugs
132 Drug Distribution and Control: Preparation and Handling–Guidelines ASHP Guidelines on Handling Hazardous Drugs ASHP published its first guidance on hazardous drugs (HDs) Because newer studies have shown that contamination in 1983 as part of the 1983–84 ASHP Practice Spotlight: Safe is widespread in healthcare settings and that more workers Handling of Cytotoxic Drugs.1,2 This was followed by tech- than previously thought are exposed, these guidelines should nical assistance bulletins in 1985 and 1990 and the ASHP be implemented wherever HDs are received, stored, pre- Guidelines on Handling Hazardous Drugs in 2006.3-5 The pared, transported, administered, or disposed.8-11 2006 guidelines were created to harmonize with the National Comprehensive reviews of the literature covering an- Institute for Occupational Safety and Health (NIOSH) Alert: ecdotal and case reports of surface contamination, worker ex- 6,9,12 Preventing Occupational Exposure to Antineoplastic and posure, and risk assessment are available from NIOSH, Other Hazardous Drugs in Health Care Settings issued in the Occupational Safety and Health Administration 13,14 15-20 2004.6 The ASHP 2006 HD guidelines were current to 2005. (OSHA), and individual authors. The primary goal In 2007, the United States Pharmacopeial Convention of this document is to provide recommendations for the safe revised United States Pharmacopeia (USP) chapter 797 handling of HDs. These guidelines represent the research (Pharmaceutical Compounding—Sterile Preparations)7 to and recommendations of many groups and individuals who harmonize with the NIOSH 2004 Alert. It became effective have worked tirelessly over decades to reduce the potential May 1, 2008, establishing many of the NIOSH recommenda harmful effects of HDs on healthcare workers. -

Targeted Therapies and Immunotherapy: General Principles (Oncology) – CE
Targeted Therapies and Immunotherapy: General Principles (Oncology) – CE ALERT Don appropriate personal protective equipment (PPE) based on the patient’s signs and symptoms and indications for isolation precautions. Refer to Oncology Nursing Society (ONS) interim guidelines for PPE recommendations during an emergent shortage of PPE (e.g., pandemic).13 Hypersensitivity reactions, such as anaphylaxis, may occur with targeted therapy and immunotherapy; therefore, frequent assessments and monitoring are required. Only qualified physicians, physician assistants, advanced practice registered nurses (APRNs), or nurses with demonstrated competency administer antineoplastic therapies. Refer to the professional’s regulatory scope of practice and the organization’s practice. Take steps to eliminate interruptions and distractions during medication preparation. OVERVIEW Normal cell reproduction, growth, and apoptosis are controlled by complex signaling pathways at the extracellular and intracellular levels. Malfunctioning of these pathways occurs in malignancies, leading to increased proliferation, tissue invasion, metastases, and apoptosis inhibition.18 Development of targeted therapies overcame the lack of selectivity associated with conventional antineoplastic therapy by targeting specific protein pathways.5 Although these pathways can be present in normal tissue, they are overexpressed or mutated in cancerous tissue.1 Cancer immunotherapy represents precision medicine, which helps the immune system fight cancer and offers a type of targeted or personalized therapy.4,11 In comparison, traditional cytotoxic chemotherapy attacks both malignant and nonmalignant cells, causing disruption of the cell cycle and other cell functions. Targeted therapy may not be more or less effective than traditional antineoplastic therapies, but it offers a unique approach to the treatment of cancer and other diseases and has toxicities different from those of traditional antineoplastic therapy. -

BC Cancer Benefit Drug List September 2021
Page 1 of 65 BC Cancer Benefit Drug List September 2021 DEFINITIONS Class I Reimbursed for active cancer or approved treatment or approved indication only. Reimbursed for approved indications only. Completion of the BC Cancer Compassionate Access Program Application (formerly Undesignated Indication Form) is necessary to Restricted Funding (R) provide the appropriate clinical information for each patient. NOTES 1. BC Cancer will reimburse, to the Communities Oncology Network hospital pharmacy, the actual acquisition cost of a Benefit Drug, up to the maximum price as determined by BC Cancer, based on the current brand and contract price. Please contact the OSCAR Hotline at 1-888-355-0355 if more information is required. 2. Not Otherwise Specified (NOS) code only applicable to Class I drugs where indicated. 3. Intrahepatic use of chemotherapy drugs is not reimbursable unless specified. 4. For queries regarding other indications not specified, please contact the BC Cancer Compassionate Access Program Office at 604.877.6000 x 6277 or [email protected] DOSAGE TUMOUR PROTOCOL DRUG APPROVED INDICATIONS CLASS NOTES FORM SITE CODES Therapy for Metastatic Castration-Sensitive Prostate Cancer using abiraterone tablet Genitourinary UGUMCSPABI* R Abiraterone and Prednisone Palliative Therapy for Metastatic Castration Resistant Prostate Cancer abiraterone tablet Genitourinary UGUPABI R Using Abiraterone and prednisone acitretin capsule Lymphoma reversal of early dysplastic and neoplastic stem changes LYNOS I first-line treatment of epidermal -

Australian Public Assessment Report for Pegaspargase
Australian Public Assessment Report for pegaspargase Proprietary Product Name: Oncaspar Sponsor: Baxalta Australia September 2018 Therapeutic Goods Administration About the Therapeutic Goods Administration (TGA) • The Therapeutic Goods Administration (TGA) is part of the Australian Government Department of Health and is responsible for regulating medicines and medical devices. • The TGA administers the Therapeutic Goods Act 1989 (the Act), applying a risk management approach designed to ensure therapeutic goods supplied in Australia meet acceptable standards of quality, safety and efficacy (performance) when necessary. • The work of the TGA is based on applying scientific and clinical expertise to decision- making, to ensure that the benefits to consumers outweigh any risks associated with the use of medicines and medical devices. • The TGA relies on the public, healthcare professionals and industry to report problems with medicines or medical devices. TGA investigates reports received by it to determine any necessary regulatory action. • To report a problem with a medicine or medical device, please see the information on the TGA website < https://www.tga.gov.au>. About AusPARs • An Australian Public Assessment Report (AusPAR) provides information about the evaluation of a prescription medicine and the considerations that led the TGA to approve or not approve a prescription medicine submission. • AusPARs are prepared and published by the TGA. • An AusPAR is prepared for submissions that relate to new chemical entities, generic medicines, major variations and extensions of indications. • An AusPAR is a static document; it provides information that relates to a submission at a particular point in time. • A new AusPAR will be developed to reflect changes to indications and/or major variations to a prescription medicine subject to evaluation by the TGA.