Emerging Problems in Public Health, Nursing and Social Work in Tropical Regions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
(12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub
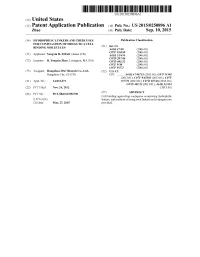
US 20150250896A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub. Date: Sep. 10, 2015 (54) HYDROPHILIC LINKERS AND THEIR USES Publication Classification FOR CONUGATION OF DRUGS TO A CELL (51) Int. Cl BNDING MOLECULES A647/48 (2006.01) (71) Applicant: Yongxin R. ZHAO, Henan (CN) Ek E. 30.8 C07D 207/216 (2006.01) (72) Inventor: R. Yongxin Zhao, Lexington, MA (US) C07D 40/12 (2006.01) C07F 9/30 (2006.01) C07F 9/572 (2006.01) (73) Assignee: Hangzhou DAC Biotech Co., Ltd., (52) U.S. Cl. Hangzhou City, ZJ (CN) CPC ........... A61K47/48715 (2013.01); C07F 9/301 (2013.01); C07F 9/65583 (2013.01); C07F (21) Appl. No.: 14/432,073 9/5721 (2013.01); C07D 207/46 (2013.01); C07D 401/12 (2013.01); A61 K3I/454 (22) PCT Filed: Nov. 24, 2012 (2013.01) (86). PCT No.: PCT/B2O12/0567OO Cell(57) binding- agent-drugABSTRACT conjugates comprising hydrophilic- S371 (c)(1), linkers, and methods of using Such linkers and conjugates are (2) Date: Mar. 27, 2015 provided. Patent Application Publication Sep. 10, 2015 Sheet 1 of 23 US 2015/0250896 A1 O HMDS OSiMe 2n O Br H-B-H HPC 3 2 COOEt essiop-\5. E B to NH 120 °C, 2h OsiMe3 J 50 °C, 2h eSiO OEt 120 oC, sh 1 2 3. 42% from 1 Bra-11a1'oet - Brn 11-1 or a 1-1 or ÓH 140 °C ÓEt ÓEt 4 5 6 - --Messio. 8 B1a-Br aus 20 cc, hP-1}^-'ot Br1-Y. -

Anew Drug Design Strategy in the Liht of Molecular Hybridization Concept
www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 12 December 2020 | ISSN: 2320-2882 “Drug Design strategy and chemical process maximization in the light of Molecular Hybridization Concept.” Subhasis Basu, Ph D Registration No: VB 1198 of 2018-2019. Department Of Chemistry, Visva-Bharati University A Draft Thesis is submitted for the partial fulfilment of PhD in Chemistry Thesis/Degree proceeding. DECLARATION I Certify that a. The Work contained in this thesis is original and has been done by me under the guidance of my supervisor. b. The work has not been submitted to any other Institute for any degree or diploma. c. I have followed the guidelines provided by the Institute in preparing the thesis. d. I have conformed to the norms and guidelines given in the Ethical Code of Conduct of the Institute. e. Whenever I have used materials (data, theoretical analysis, figures and text) from other sources, I have given due credit to them by citing them in the text of the thesis and giving their details in the references. Further, I have taken permission from the copyright owners of the sources, whenever necessary. IJCRT2012039 International Journal of Creative Research Thoughts (IJCRT) www.ijcrt.org 284 www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 12 December 2020 | ISSN: 2320-2882 f. Whenever I have quoted written materials from other sources I have put them under quotation marks and given due credit to the sources by citing them and giving required details in the references. (Subhasis Basu) ACKNOWLEDGEMENT This preface is to extend an appreciation to all those individuals who with their generous co- operation guided us in every aspect to make this design and drawing successful. -

Use of the 4-Hydroxy-Triazole Moiety As a Bioisosteric Tool in the Development of Selective Ligands for Subtypes AMPA Receptor
AperTO - Archivio Istituzionale Open Access dell'Università di Torino Use of the 4-hydroxy-triazole moiety as a bioisosteric tool in the development of selective ligands for subtypes AMPA receptor This is the author's manuscript Original Citation: Availability: This version is available http://hdl.handle.net/2318/1721210 since 2020-01-03T11:23:39Z Terms of use: Open Access Anyone can freely access the full text of works made available as "Open Access". Works made available under a Creative Commons license can be used according to the terms and conditions of said license. Use of all other works requires consent of the right holder (author or publisher) if not exempted from copyright protection by the applicable law. (Article begins on next page) 09 October 2021 6th EFMC Young Medicinal Chemist Symposium September 5-6, 2019 | Athens, Greece Book of Abstracts YMCS19-BoA-Cover.indd 1 30/07/19 09:13 Organising Committees Chairman Dr Emmanouil FOUSTERIS (University of Patras, Patras, Greece) Members Dr David ALKER (David Alker Associates, Birchington, United Kingdom) Prof. Dennis GILLINGHAM (University of Basel, Basel, Switzerland) Dr Kristina GONCHARENKO (SpiroChem AG, Basel, Switzerland) Dr Cassandra LEE FLEMING (University of Gothenburg, Gothenburg, Sweden) Mr Brieuc MATAGNE (LD Organisation, Louvain-la-Neuve, Belgium) Dr Eleni PONTIKI (Aristotele University of Thessaloniki, Thessaloniki, Greece) Dr Matthew TOZER (Consultant, Cambridge, United Kingdom) Prof. Grigorios ZOIDIS (University of Athens, Athens, Greece) Content Welcome 2 Sponsors 3 Programme 5 Keynote Lectures 13 Oral Communications 19 Flash Poster Presentations 39 Posters Presentations 41 List of abstracts 153 List of participants 161 1 Welcome Dear participant, On behalf of the European Federation for Medicinal Chemistry (EFMC) and the Organising Committee, we warmly welcome you to Athens for the 6th edition of the EFMC Young Medicinal Chemist Symposium (EFMC-YMCS). -

Informe Mensual De Producción Científica Del
Instituto de Investigación Sanitaria Gregorio Marañón Listado de publicaciones por áreas y grupos de investigación JUNIO 2021 Nº FI ÁREA 1: INGENIERÍA BIOMÉDICA 1.01 Aplicaciones tecnológicas avanzadas y salud humana 2 5,016 1.02 Tratamiento de la señal 1 3,036 ÁREA 2: ENFERMEDADES CARDIOVASCULARES 2.01 Historia natural de la enfermedad cardiaca 11 57,049 2.03 Electrofisiología cardiaca celular 1 4,642 2.05 Cardiología y trasplante cardiaco infantil 3 8,838 2.06 Lípidos sanguíneos y riesgo cardiovascular 4 11,127 2.07 Enfermedad cerebrovascular aguda. Ictus 2 4,981 ÁREA 3: NEUROCIENCIA Y SALUD MENTAL 3.01 Bases neurobiológicas y psicológicas de los trastornos mentales. Trastornos del neurodesarrollo 8 71,342 3.03B Enfermedades Neurológicas 7 18,402 ÁREA 4: MICROBIOLOGÍA CLÍNICA, ENFERMEDADES INFECCIOSAS Y SIDA 4.01 Enfermedades infecciosas 8 45,759 4.02 Aspectos clínicos y epidemiológicos del VIH y condiciones asociadas 6 41,777 ÁREA 5: PATALOGÍA DEL SISTEMA INMUNE 5.01 Fisiopatología e investigación clínica de las enfermedades de base inmunológica e inflamatoria crónicas 4 11,686 5.02 Biología molecular del VIH 2 9,993 5.03 Enfermedades sistémicas de base autoinmune 4 16,730 5.05 Patogenia de la respuesta inmunoalérgica 1 7,574 5.06 Regulación y Homeostasis Inmune en Patologías relacionadas con el Sistema Inmunológico 1 4,717 5.07 Infecciones en la población pediátrica 6 16,314 ÁREA 6: ONCOLOGÍA TRASLACIONAL 6.01 Oncología interdisciplinar y bio-tecnológica 2 7,608 6.02 Oncología médica traslacional y terapia individualizada del cáncer 7 116,801 6.03 Genética y clínica de las neoplasias hematológicas y el trasplante hematopoyético 8 55,097 6.04 Oncología quirúrgica 1 1,354 ÁREA 7: PATALOGÍA DE GRANDES SISTEMAS Y TRASPLANTE DE ÓRGANOS 7.01 Inflamación y daño vascular en la Enfermedad Renal Crónica, Diálisis y Trasplante Renal. -

Patent Application Publication Oo) Pub. No.: US 2015/0284416 Al Zhao (43) Pub
US 20150284416A1 US 20150284416A1 (19) United States (12) Patent Application Publication oo) Pub. No.: US 2015/0284416 Al Zhao (43) Pub. Date: Oct. 8,2015 (54) NOVEL LINKERS LOR CONJUGATION OL A61K47/48 (2006.01) CELL-BINDING MOLECULES C07K16/32 (2006.01) C07F 9/572 (2006.01) (71) Applicant: Robert Yongxin Zhao, Lexington, MA (US) A61K 31/537 (2006.01) (52) U.S. Cl. (72) Inventor: Robert Yongxin Zhao, Lexington, MA CPC ...........C07F 9/65583 (2013.01); C07F 9/5721 (US) (2013.01); A61K31/537 (2013.01); A61K (73) Assignee: SUZHOU M-CONJ BIOTECH CO., 47/48715 (2013.01); C07K16/32 (2013.01); LTD, Suzhou City (CN) A61K 47/48561 (2013.01 ),A61K 38/05 (2013.01) (21) Appl. No.: 14/740,403 (22) Filed: Jun. 16, 2015 (57) ABSTRACT Publication Classiflcation (51) Int. Cl. Cell binding agent-drug conjugates comprising hydrophilic C07F 9/6558 (2006.01) linkers, and methods of using such linkers and conjugates are A61K38/05 (2006.01) provided. PatentApplication Publication Oct. 8, 2015 Sheet I of 18 US 2015/0284416 Al FIGURES p 0 ° Λ O=PG3 H M /v. A N-VNH2 (Tjn-Vn-II-Ci ho^^nh, (f\-vΝ-Ρ-N ν^'ίOH -78°C, THF 1 H C' Cl --------2—W THO 4 O I Et3N η O O Q NllSZEDtC jf^N -P-NyVjlS0^ N^S I). Drug-SH DMA V HO “ . 2). mAb— (NH2)11 O OPCi3^ I n-vnh2 HO NH2 C' -78°C, THF I). Drug-SH 2). UiAb-(NH2)n 0. KJ kj ■Nj1^—1 Drug-NH2 (T\'VN'v^'"(LNn^-A>SzuV" Dri|8 dr & “V- P Figure I. -

September 5-6, 2019 | Athens, Greece Book of Abstracts
6th EFMC Young Medicinal Chemist Symposium September 5-6, 2019 | Athens, Greece Book of Abstracts YMCS19-BoA-Cover.indd 1 30/07/19 09:13 Organising Committees Chairman Dr Emmanouil FOUSTERIS (University of Patras, Patras, Greece) Members Dr David ALKER (David Alker Associates, Birchington, United Kingdom) Prof. Dennis GILLINGHAM (University of Basel, Basel, Switzerland) Dr Kristina GONCHARENKO (SpiroChem AG, Basel, Switzerland) Dr Cassandra LEE FLEMING (University of Gothenburg, Gothenburg, Sweden) Mr Brieuc MATAGNE (LD Organisation, Louvain-la-Neuve, Belgium) Dr Eleni PONTIKI (Aristotele University of Thessaloniki, Thessaloniki, Greece) Dr Matthew TOZER (Consultant, Cambridge, United Kingdom) Prof. Grigorios ZOIDIS (University of Athens, Athens, Greece) Content Welcome 2 Sponsors 3 Programme 5 Keynote Lectures 13 Oral Communications 19 Flash Poster Presentations 39 Posters Presentations 41 List of abstracts 153 List of participants 161 1 Welcome Dear participant, On behalf of the European Federation for Medicinal Chemistry (EFMC) and the Organising Committee, we warmly welcome you to Athens for the 6th edition of the EFMC Young Medicinal Chemist Symposium (EFMC-YMCS). Since the first edition of the EFMC-YMCS in 2014, the symposium has gone from strength to strength with increased participation from EFMC-National Adhering Organisations, and it is now firmly established as the premier forum in Europe for young Medicinal Chemistry and Chemical Biology researchers to promote their science. Our principal aims are: • Creating a network of young European investigators in Medicinal Chemistry and Chemical Biology • Stimulating young European investigators to share their scientific work with peers, and inspiring them to become leaders in their field • Creating competition, excellence and European Champions in Medicinal Chemistry and Chemical Biology This year, more than 170 scientists from 30 nations will gather in Athens for the latest edition. -
Download the 2017-18 Annual Report
Molecular Biology Institute ANNUAL REPORT 2017-2018 (310) 825-1018 mbi.ucla.edu UCLA Boyer Hall [email protected] MOLECULAR BIOLOGY INSTITUTE REMEMBERING PAUL BOYER MBI DIRECTOR’S REPORT 1 MBI COMMITTEES 3 MBI ADMINISTRATIVE SUPPORT STAFF ACTIVITIES Administrative Services 4 Building Management 5 MBI PROGRAMS & EVENTS The David S. Sigman Memorial Lectureship & Symposium 7 The Audree Fowler Fellows in Protein Science 8 The Jules Brenner Achievement Fellowship in Molecular Biology 9 Boyer/Parvin Postdoctoral Research Awards 10 Thursday Seminar Series 11 MBI Interdisciplinary Faculty Seminars 14 MBI Annual Retreat & Research Conference 18 Biotechnology Edge Workshop 16 Focus on Imaging Workshop 17 Mouse Genome Informatics Workshop 18 MBI FACULTY RESEARCH & PROFESSIONAL ACTIVITIES Newly Appointed Members 19 Honors & Professional Awards 22 Service on UCLA Committees 23 Service on External Committees 27 Patents Issued 32 Visiting Faculty & Scholars 33 MBI PARTNERS IN BOYER HALL Institute for Quantitative & Computational Biology (QCBio) 35 The QCBio Collaboratory 35 UCLA-DOE Institute 35 Fermentation Core Facility 36 GRADUATE PROGRAMS Molecular Biology Interdepartmental Ph.D. Program (MBIDP) 37 Whitcome Pre-doctoral Training Program 54 MEMBER PUBLICATIONS MBI Faculty Publications 55 PAUL D. BOYER 1918 - 2018 REMEMBERING WITH GRATITUDE PAUL D. BOYER 1918 - 2018 Dear Colleagues, This year will be forever memorable in the history of our Institute because it marks the passing of our beloved Paul Boyer. His many scientific and academic accomplishments have been highlighted in several journals and it has been wonderful to hear so many colleagues speak about how much Dr. Boyer meant to them. We are grateful for his vision, his collegiality, his commitment to scientific excellence and his optimistic spirit, all of which became part of the culture of our institute. -

WO 2013/167743 Al 14 November 2013 (14.11.2013) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization I International Bureau (10) International Publication Number (43) International Publication Date WO 2013/167743 Al 14 November 2013 (14.11.2013) P O P C T (51) International Patent Classification: AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, A61K 31/18 (2006.01) A61K 31/708 (2006.01) BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, A61K 31/522 (2006.01) A61K 45/06 (2006.01) DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, A61K 31/675 (2006.01) A61P 29/00 (2006.01) HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, A61K 31/7068 (2006.01) KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, (21) International Application Number: NO, NZ, OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, PCT/EP2013/059752 RW, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, (22) International Filing Date: TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, 10 May 2013 (10.05.2013) ZM, ZW. (25) Filing Language: English (84) Designated States (unless otherwise indicated, for every kind of regional protection available): ARIPO (BW, GH, (26) Publication Language: English GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, (30) Priority Data: UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, 12167771 .0 11 May 2012 ( 11.05.2012) EP TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, LV, (71) Applicant: AKRON MOLECULES GMBH [AT/AT]; MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, SM, Helmut-Qualtinger-Gasse 2, A-1030 Vienna (AT). -
(12) Patent Application Publication (10) Pub. No.: US 2016/0346380 A1 Stenler Et Al
US 2016.0346.380A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2016/0346380 A1 Stenler et al. (43) Pub. Date: Dec. 1, 2016 (54) T20 CONSTRUCTS FOR ANTI-HIV (HUMAN (52) U.S. Cl. IMMUNODEFICIENCY VIRUS) THERAPY CPC ............... A61K 39/21 (2013.01); A61K 45/06 AND/OR VACCINES (2013.01); A61K 39/42 (2013.01); A61 K (71) Applicant: Immunomedics, Inc., Morris Plains, NJ 2039/53 (2013.01) (US) (57) ABSTRACT (72) Inventors: Sofia Stenler, Stockholm (SE); Britta Wahren, Stockholm (SE): Chien-Hsing The present invention concerns methods and compositions SS SSA S.sid for treatment of HIV infection using a T20 expression 9, s vector, such as that shown in SEQ ID NO:1 or SEQ ID (21) Appl. No.: 15/164,437 NO:3. The T20 expression vector may be used in a variety of therapeutic applications, such as ex vivo transfection of (22) Filed: May 25, 2016 dendritic cells to induce a host immune response to HIV. Related U.S. Application Data localized transfection in vivo in a gene therapy approach to (60) Provisional application No. 62/167,404, filed on May provide longer term delivery of T20, or in vitro production 28, 2015 s w is of T20 peptide. The T20 may be secreted into the circulation s to act as a fusion inhibitor of HIV infection, or may induce Publication Classification an endogenous immune response to HIV or HIV-infected (51) Int. Cl cells. Alternatively, a DDD peptide may be incorporated in A. iK 39/21 (2006.01) a fusion protein comprising T20 or another antigenic protein A6 IK 39/42 (2006.01) or peptide to enhance the immune response to the protein or A6 IK 45/06 (2006.01) peptide. -

Abstracts Bialystok 2019
BOOK OF ABSTRACTS BIALYSTOK 2019 14th Bialystok International Medical Congress for Young Scientists Book of Abstracts Białystok 2019 1 BIALYSTOK 2019 © Copyright by Students’ Scientific Society of the Medical University of Bialystok, 2019 Wszystkie prawa zastrzeżone. Przedruk i reprodukcja w jakiejkolwiek postaci całości bądź części książki bez pisemnej zgody wydawcy są zabronione. Redaktor: Małgorzata Kowalska, Monika Oleksiuk, Bogumiła Szewczak, Sylwia Bajko Korekta: Anna Krętowska, Aleksandra Basaj Grafika: Marta Śleszyńska ISBN: 978-83-952075-0-1 Za treść i format poszczególnych streszczeń odpowiadają ich autorzy. STN UMB nie odpowiada za informacje podane w formularzach zgłoszeniowych (błędy w nazwiskach, tytułach etc.) 2 BIALYSTOK 2019 Dear Colleagues, It is a great pleasure for me to welcome the participants of the 14th Bialystok International Medical Congress (BIMC) from Poland, Lithuania, Belarus, Ukraine and Latvia who came to Bialystok in order to exchange scientific experience and have a good time for a few days in one of the most enjoyable cities of Poland. We are truly happy and privileged to welcome you at Medical University of Bialystok. This is thank to your continuous interest and kindness that BIMC has become one of the most vibrant congresses gathering hundreds of young scientists from different European countries. I wish to thank warmly the Organizing Committee of the 14th BIMC for their enormous dedication, contagious energy and numberless efforts they put into making this event so unique. Let me extend special thanks to all members of faculty of the Medical University of Bialystok who agreed to sacrifice their time in order to share their experience and scientific advice during numerous scientific sessions. -

WO 2015/151078 A4 8 October 2015 (08.10.2015) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2015/151078 A4 8 October 2015 (08.10.2015) P O P C T (51) International Patent Classification: (84) Designated States (unless otherwise indicated, for every C07F 9/6558 (2006.01) C07K 16/32 (2006.01) kind of regional protection available): ARIPO (BW, GH, A61K 38/05 (2006.01) C07F 9/572 (2006.01) GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, A61K 47/48 (2006.01) A61K 31/537 (2006.01) TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, (21) Number: International Application DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, PCT/IB20 15/054521 LV, MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, (22) International Filing Date: SM, TR), OAPI (BF, BJ, CF, CG, CI, CM, GA, GN, GQ, 15 June 2015 (15.06.2015) GW, KM, ML, MR, NE, SN, TD, TG). (25) Filing Language: English Declarations under Rule 4.17 : (26) Publication Language: English — as to the identity of the inventor (Rule 4.1 7(Ϊ)) — as to applicant's entitlement to apply for and be granted a (71) Applicant: HANGZHOU DAC BIOTECH CO., LTD patent (Rule 4.1 7(H)) [CN/CN]; Room B2001-B2019, Building 2, No. 452 Six Street, Heda, Hangzhou City, Zhejiang Province, 310018 — of inventorship (Rule 4.17(iv)) (CN). -

Table of Contents
OCTOBER 2015 • VOLUME 59 • NO. 10 TABLE OF CONTENTS MINIREVIEWS Carbapenemase-Producing Klebsiella pneumoniae, a Key Johann D. D. Pitout, Patrice 5873–5884 Pathogen Set for Global Nosocomial Dominance Nordmann, Laurent Poirel Potential Targets for Antifungal Drug Discovery Based on Xiuyun Li, Yinglong Hou, Longtao Yue, 5885–5891 Growth and Virulence in Candida albicans Shuyuan Liu, Juan Du, Shujuan Sun Addressing Therapeutic Options for Ebola Virus Infection in Azizul Haque, Didier Hober, Joel 5892–5902 Current and Future Outbreaks Blondiaux CHALLENGING CLINICAL CASES IN ANTIMICROBIAL RESISTANCE Successful Treatment of Carbapenemase-Producing Pandrug- Jose F. Camargo, Jacques Simkins, 5903–5908 Resistant Klebsiella pneumoniae Bacteremia Thiago Beduschi, Akin Tekin, Laura Aragon, Armando Pérez-Cardona, Clara E. Prado, Michele I. Morris, Lilian M. Abbo, Rafael Cantón (Commentator) MECHANISMS OF ACTION: PHYSIOLOGICAL EFFECTS Garcinia xanthochymus Benzophenones Promote Hyphal Desmond N. Jackson, Lin Yang, 6032–6038 Apoptosis and Potentiate Activity of Fluconazole against ShiBiao Wu, Edward J. Kennelly, Candida albicans Biofilms Peter N. Lipke Differential Effects of Penicillin Binding Protein Deletion on the George Sakoulas, Monika 6132–6139 Susceptibility of Enterococcus faecium to Cationic Peptide Kumaraswamy, Poochit Nonejuie, Antibiotics Brian J. Werth, Micahel J. Rybak, Joseph Pogliano, Louis B. Rice, Victor Nizet Subinhibitory Doses of Aminoglycoside Antibiotics Induce Sheng-Hui Tsai, Hsin-Chih Lai, 6161–6169 Changes in the Phenotype of Mycobacterium abscessus Shiau-Ting Hu New Insights Regarding Yeast Survival following Exposure to Rita Teixeira-Santos, Elisabete Ricardo, 6181–6187 Liposomal Amphotericin B Susana Gomes Guerreiro, Sofia Costa-de-Oliveira, Acácio Gonçalves Rodrigues, Cidália Pina-Vaz The Glucose Transporter PfHT1 Is an Antimalarial Target of the Thomas E.