GH 8 2 V Announcement
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Long-Term Trends and Survival Analysis of Esophageal and Gastric Cancer in Yangzhong, 1991-2013
RESEARCH ARTICLE Long-term trends and survival analysis of esophageal and gastric cancer in Yangzhong, 1991-2013 Zhaolai Hua1,2☯, Xianzhi Zheng2☯, Hengchuan Xue3, Jianming Wang2,4*, Jun Yao5* 1 Department of Epidemiology, Yangzhong Cancer Research Institute, Yangzhong, China, 2 Department of Epidemiology, School of Public Health, Nanjing Medical University, Nanjing, China, 3 Department of Thoracic Surgery, People's Hospital of Yangzhong, Yangzhong, China, 4 The Innovation Center for Social Risk Governance in Health, School of Public Health, Nanjing Medical University, Nanjing, China, 5 Department of Gastroenterology, Zhenjiang First People's Hospital, Zhenjiang, China a1111111111 a1111111111 ☯ These authors contributed equally to this work. a1111111111 * [email protected] (JW); [email protected] (JY) a1111111111 a1111111111 Abstract Objective OPEN ACCESS Citation: Hua Z, Zheng X, Xue H, Wang J, Yao J To describe the long-term trends of the incidence, mortality and survival of upper digestive (2017) Long-term trends and survival analysis of tract cancers in a high-risk area of China. esophageal and gastric cancer in Yangzhong, 1991-2013. PLoS ONE 12(3): e0173896. https:// doi.org/10.1371/journal.pone.0173896 Methods Editor: Wayne A Phillips, Peter MacCallum Cancer We extracted esophageal and gastric cancer cases diagnosed from 1991 to 2013 through Centre, AUSTRALIA the Yangzhong Cancer Registry and calculated the crude and age-standardized incidence Received: September 29, 2016 and mortality rates. Cancer trends were calculated using the Joinpoint Regression Program and were reported using the annual percentage change (APC). The cancer-specific survival Accepted: February 28, 2017 rates were evaluated and compared between groups using the Kaplan-Meier method and Published: March 13, 2017 log-rank test. -

Produzent Adresse Land Allplast Bangladesh Ltd
Zeitraum - Produzenten mit einem Liefertermin zwischen 01.01.2020 und 31.12.2020 Produzent Adresse Land Allplast Bangladesh Ltd. Mulgaon, Kaliganj, Gazipur, Rfl Industrial Park Rip, Mulgaon, Sandanpara, Kaligonj, Gazipur, Dhaka Bangladesh Bengal Plastics Ltd. (Unit - 3) Yearpur, Zirabo Bazar, Savar, Dhaka Bangladesh Durable Plastic Ltd. Mulgaon, Kaligonj, Gazipur, Dhaka Bangladesh HKD International (Cepz) Ltd. Plot # 49-52, Sector # 8, Cepz, Chittagong Bangladesh Lhotse (Bd) Ltd. Plot No. 60 & 61, Sector -3, Karnaphuli Export Processing Zone, North Potenga, Chittagong Bangladesh Plastoflex Doo Branilaca Grada Bb, Gračanica, Federacija Bosne I H Bosnia-Herz. ASF Sporting Goods Co., Ltd. Km 38.5, National Road No. 3, Thlork Village, Chonrok Commune, Konrrg Pisey, Kampong Spueu Cambodia Powerjet Home Product (Cambodia) Co., Ltd. Manhattan (Svay Rieng) Special Economic Zone, National Road 1, Sangkat Bavet, Krong Bavet, Svaay Rieng Cambodia AJS Electronics Ltd. 1st Floor, No. 3 Road 4, Dawei, Xinqiao, Xinqiao Community, Xinqiao Street, Baoan District, Shenzhen, Guangdong China AP Group (China) Co., Ltd. Ap Industry Garden, Quetang East District, Jinjiang, Fujian China Ability Technology (Dong Guan) Co., Ltd. Songbai Road East, Huanan Industrial Area, Liaobu Town, Donggguan, Guangdong China Anhui Goldmen Industry & Trading Co., Ltd. A-14, Zongyang Industrial Park, Tongling, Anhui China Aold Electronic Ltd. Near The Dahou Viaduct, Tianxin Industrial District, Dahou Village, Xiegang Town, Dongguan, Guangdong China Aurolite Electrical (Panyu Guangzhou) Ltd. Jinsheng Road No. 1, Jinhu Industrial Zone, Hualong, Panyu District, Guangzhou, Guangdong China Avita (Wujiang) Co., Ltd. No. 858, Jiaotong Road, Wujiang Economic Development Zone, Suzhou, Jiangsu China Bada Mechanical & Electrical Co., Ltd. No. 8 Yumeng Road, Ruian Economic Development Zone, Ruian, Zhejiang China Betec Group Ltd. -
SGS-Safeguards 04910- Minimum Wages Increased in Jiangsu -EN-10
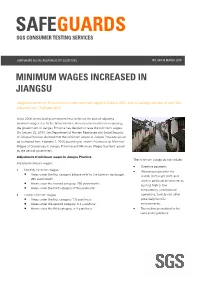
SAFEGUARDS SGS CONSUMER TESTING SERVICES CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 MINIMUM WAGES INCREASED IN JIANGSU Jiangsu becomes the first province to raise minimum wages in China in 2010, with an average increase of over 12% effective from 1 February 2010. Since 2008, many local governments have deferred the plan of adjusting minimum wages due to the financial crisis. As economic results are improving, the government of Jiangsu Province has decided to raise the minimum wages. On January 23, 2010, the Department of Human Resources and Social Security of Jiangsu Province declared that the minimum wages in Jiangsu Province would be increased from February 1, 2010 according to Interim Provisions on Minimum Wages of Enterprises in Jiangsu Province and Minimum Wages Standard issued by the central government. Adjustment of minimum wages in Jiangsu Province The minimum wages do not include: Adjusted minimum wages: • Overtime payment; • Monthly minimum wages: • Allowances given for the Areas under the first category (please refer to the table on next page): middle shift, night shift, and 960 yuan/month; work in particular environments Areas under the second category: 790 yuan/month; such as high or low Areas under the third category: 670 yuan/month temperature, underground • Hourly minimum wages: operations, toxicity and other Areas under the first category: 7.8 yuan/hour; potentially harmful Areas under the second category: 6.4 yuan/hour; environments; Areas under the third category: 5.4 yuan/hour. • The welfare prescribed in the laws and regulations. CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 P.2 Hourly minimum wages are calculated on the basis of the announced monthly minimum wages, taking into account: • The basic pension insurance premiums and the basic medical insurance premiums that shall be paid by the employers. -

Updates on Chinese Port Information During COVID-19 Outbreak - 10.03.2020
Moir Alistair From: Harris Guy Sent: 12 March 2020 15:40 To: Group - IR Subject: FW: Huatai Info-Updates on Chinese Port Information during COVID-19 outbreak - 10.03.2020 Importance: High trProcessed: Sent From: 北京海事 <[email protected]> Sent: 10 March 2020 13:26 To: Chan Connie <[email protected]> Subject: Huatai Info-Updates on Chinese Port Information during COVID-19 outbreak. - Mar 10th, 2020 Dear Sirs/Madams, With the improvement of the epidemic situation, work resumption is taking place across China except for Hubei province, the hardest-hit region. With the increase of overseas COVID-19 cases, ports are becoming the front line of the battle against the epidemic. Most protective measures implemented by port authorities are still in force and we suggest shipowners to keep on following the notice we made in our previous Huatai Info to avoid any problems. Please note that to date our Huatai offices have come back to normal operating condition. Though some of our staff continues to work from home, they can be reached by email and mobile phone as normal. Besides the daily case handling, we shall keep collecting relevant information on COVID-19 related policy as well as latest port situation to protect Club/Members’ best interests. At the end of this Info we hereby provide the updated port information collected from local parties concerned (port authorities, survey firms, etc.) to help Club/Members make the best arrangement when your good vessel facing any potential claims during calling at Chinese ports. We really appreciate all your thoughtfulness and concern about our situation during Covid-19 epidemic. -

Jiangsu(PDF/288KB)
Mizuho Bank China Business Promotion Division Jiangsu Province Overview Abbreviated Name Su Provincial Capital Nanjing Administrative 13 cities and 45 counties Divisions Secretary of the Luo Zhijun; Provincial Party Li Xueyong Committee; Mayor 2 Size 102,600 km Shandong Annual Mean 16.2°C Jiangsu Temperature Anhui Shanghai Annual Precipitation 861.9 mm Zhejiang Official Government www.jiangsu.gov.cn URL Note: Personnel information as of September 2014 [Economic Scale] Unit 2012 2013 National Share (%) Ranking Gross Domestic Product (GDP) 100 Million RMB 54,058 59,162 2 10.4 Per Capita GDP RMB 68,347 74,607 4 - Value-added Industrial Output (enterprises above a designated 100 Million RMB N.A. N.A. N.A. N.A. size) Agriculture, Forestry and Fishery 100 Million RMB 5,809 6,158 3 6.3 Output Total Investment in Fixed Assets 100 Million RMB 30,854 36,373 2 8.2 Fiscal Revenue 100 Million RMB 5,861 6,568 2 5.1 Fiscal Expenditure 100 Million RMB 7,028 7,798 2 5.6 Total Retail Sales of Consumer 100 Million RMB 18,331 20,797 3 8.7 Goods Foreign Currency Revenue from Million USD 6,300 2,380 10 4.6 Inbound Tourism Export Value Million USD 328,524 328,857 2 14.9 Import Value Million USD 219,438 221,987 4 11.4 Export Surplus Million USD 109,086 106,870 3 16.3 Total Import and Export Value Million USD 547,961 550,844 2 13.2 Foreign Direct Investment No. of contracts 4,156 3,453 N.A. -

Area/Temperature Limitation to Application of Vetiver System in China
Adequate Areas in China for the Application of Vetiver System Liyu XU (China Vetiver Network, Nanjing 210008) Abstract: Vetiver System was introduced into China by Mr. Grimshaw from the World Bank in 1988. Beginning from the Fuzhou Symposium in 1997, the system was applied for infrastructure protection in China. Since the Nanchang Symposium in 1999, it was extended quickly countrywide, and in particular, it was extensively applied and extended in South China. On the basis of reviewing successful research cases all over China, this paper deals with adequate areas where vetiver grasses can be planted, and lists related issues that should be further studied in the future. Key words: Vetiver system, Slope protection, Adequate planting area Environment protection is one of the most urgent missions faced by the contemporary world and also one of the basic tasks faced by the Chinese people in their economical construction and social development. Therefore, it should be considered as a basic state policy to be adhered in a long historic period. In its broad sense, environment protection consists of two fields, i.e., soil and water conservation as well as pollution control. To practice environment protection, various measures may be adopted. However, among those measures, bioengineering technology has been becoming favorite one frequently adopted by more and more people in recent years. Vetiver (Vetiveria zizanioides) is characterized by its strong stress tolerance, wide adoptability, quick growing vitality, huge biomass, highly developed root system with fantastic mechanical properties, and powerful soil bounding capacity as well as is to be easily planted and simply managed at very low cost. -

1 RIVERBED EVOLUTION of UPPER PART of YANGTZE ESTUARY and ITS RESPONSE to the HYDRODYNAMIC CHANGES at UPSTREAM Yongping Chen1
RIVERBED EVOLUTION OF UPPER PART OF YANGTZE ESTUARY AND ITS RESPONSE TO THE HYDRODYNAMIC CHANGES AT UPSTREAM Yongping Chen1, Ninglin Jiang 2 and Changkuan Zhang3 The riverbed evolution of upper part of Yangtze estuary, Chengtong reach, is analyzed by comparison of 6 sets of bathymetry data during 1977~2011. The significant changes of water depth profiles along 6 representative cross- sections indicate this reach is still in the process of development. In order to get a better understanding of the effect of river discharge at upstream on the riverbed evolution of Chengtong reach, a series of numerical experiments are implemented by specifying different river discharge conditions at the upper boundary. The corresponding discharge ratios of main and secondary channels at 3 main sub-reaches are compared. The results show that with the increase of river discharge, the discharge ratio in the main channels of Fujiangsha sub-reach and Rugaosha sub-reach increases, but it changes to decrease when the upstream river discharge becomes very large; however, the discharge ratio in the main channel of Tongzhousha sub-reach always decreases with the increase of river discharge at upstream. The discharge ratio of secondary channel has an adverse tendency. Keywords: Yangtze estuary; Chengtong reach; riverbed evolution; numerical modeling; upstream discharge INTRODUCTION Yangtze River is the longest river in China and the third longest river in the world. The estuary of Yangtze River starts from Ebizui of Jiangsu Province and reaches the East China Sea by the city of Shanghai. In recent years, the riverbed of Yangtze estuary has exhibited significant changes under the effects of natural evolution and anthropogenic works (Yang et al, 2006; Liu et al, 2007). -

Inter-Observer Agreement of Computed Tomography and Magnetic Resonance Imaging on Gross Tumor Volume Delineation of Intrahepatic Cholangiocarcinoma: an Initial Study
579 Original Article Inter-observer agreement of computed tomography and magnetic resonance imaging on gross tumor volume delineation of intrahepatic cholangiocarcinoma: an initial study Nan Zhou1#, Anning Hu1#, Zhihao Shi1#, Xiaolu Wang2, Qiongjie Zhu1, Qun Zhou1, Jun Ma3, Feng Zhao4, Weiwei Kong2,5, Jian He1 1Department of Radiology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, China; 2The Comprehensive Cancer Centre of Drum Tower Hospital, Medical School of Nanjing University & Clinical Cancer Institute of Nanjing University, Nanjing, China; 3Department of Mathematics, Nanjing University of Science and Technology, Nanjing, China; 4Department of Radiation Oncology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; 5Department of Oncology of Yizheng Hospital, Nanjing Drum Tower Hospital Group, Yizheng, China #These authors contributed equally to this work. Correspondence to: Jian He, PhD. Department of Radiology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, No. 321 Zhongshan Road, Nanjing 210008, China. Email: [email protected]; Weiwei Kong, MD. The Comprehensive Cancer Centre of Drum Tower Hospital, Medical School of Nanjing University & Clinical Cancer Institute of Nanjing University, Nanjing 210008, China; Department of Oncology of Yizheng Hospital, Nanjing Drum Tower Hospital Group, Yizheng 211400, China. Email: [email protected]. Background: Intrahepatic cholangiocarcinoma (ICC) is the second most common primary liver tumor, and local radiotherapy has a positive effect on patients with an unresectable tumor. Accurate delineation of gross tumor volume (GTV) is crucial to improve the efficacy of radiotherapy. The purpose of this article was to evaluate the consistency of CT, diffusion weighted imaging (DWI) and Gadoxetic acid disodium (Gd- EOB-DTPA)-enhanced MRI on GTV delineation of ICC. -

Habitat Specialisation in the Reed Parrotbill Paradoxornis Heudei Evidence from Its Distribution and Habitat
FORKTAIL 29 (2013): 64–70 Habitat specialisation in the Reed Parrotbill Paradoxornis heudei—evidence from its distribution and habitat use LI-HU XIONG & JIAN-JIAN LU The Reed Parrotbill Paradoxornis heudei is found in habitats dominated by Common Reed Phragmites australis in East Asia. This project was designed to test whether the Reed Parrotbill is a specialist of reed-dominated habitats, using data collected through literature review and field observations. About 87% of academic publications describing Reed Parrotbill habitat report an association with reeds, and the species was recorded in reeds at 92% of sites where it occurred. On Chongming Island, birds were only recorded in transects covered with reeds or transects with scattered reeds close to large reedbeds. At the Chongxi Wetland Research Centre, monthly monitoring over three years also showed that the species was not recorded in habitats without reeds. The density of Reed Parrotbills was higher in reedbeds than mixed vegetation (reeds with planted trees) and small patches of reeds. The species rarely appeared in mixed habitat after reeds disappeared. These results confirm that the species is a reed specialist and highlights that conservation of reed-dominated habitat is a precondition to conserve the Reed Parrotbill. INTRODUCTION METHODS Habitat specialisation results in some species having a close Three sets of information on Reed Parrotbill distribution and relationship with only a few habitat types (Futuyma & Moreno habitat use were used: (1) distribution and habitat use data in the 1988), and habitat specialists have some specific life-history Chinese part of its range, collated from academic publications, web characteristics, for example, they often have weak dispersal abilities news, communication with birdwatchers and personal (Krauss et al. -

Shop Direct Factory List Dec 18
Factory Factory Address Country Sector FTE No. workers % Male % Female ESSENTIAL CLOTHING LTD Akulichala, Sakashhor, Maddha Para, Kaliakor, Gazipur, Bangladesh BANGLADESH Garments 669 55% 45% NANTONG AIKE GARMENTS COMPANY LTD Group 14, Huanchi Village, Jiangan Town, Rugao City, Jaingsu Province, China CHINA Garments 159 22% 78% DEEKAY KNITWEARS LTD SF No. 229, Karaipudhur, Arulpuram, Palladam Road, Tirupur, 641605, Tamil Nadu, India INDIA Garments 129 57% 43% HD4U No. 8, Yijiang Road, Lianhang Economic Development Zone, Haining CHINA Home Textiles 98 45% 55% AIRSPRUNG BEDS LTD Canal Road, Canal Road Industrial Estate, Trowbridge, Wiltshire, BA14 8RQ, United Kingdom UK Furniture 398 83% 17% ASIAN LEATHERS LIMITED Asian House, E. M. Bypass, Kasba, Kolkata, 700017, India INDIA Accessories 978 77% 23% AMAN KNITTINGS LIMITED Nazimnagar, Hemayetpur, Savar, Dhaka, Bangladesh BANGLADESH Garments 1708 60% 30% V K FASHION LTD formerly STYLEWISE LTD Unit 5, 99 Bridge Road, Leicester, LE5 3LD, United Kingdom UK Garments 51 43% 57% AMAN GRAPHIC & DESIGN LTD. Najim Nagar, Hemayetpur, Savar, Dhaka, Bangladesh BANGLADESH Garments 3260 40% 60% WENZHOU SUNRISE INDUSTRIAL CO., LTD. Floor 2, 1 Building Qiangqiang Group, Shanghui Industrial Zone, Louqiao Street, Ouhai, Wenzhou, Zhejiang Province, China CHINA Accessories 716 58% 42% AMAZING EXPORTS CORPORATION - UNIT I Sf No. 105, Valayankadu, P. Vadugapal Ayam Post, Dharapuram Road, Palladam, 541664, India INDIA Garments 490 53% 47% ANDRA JEWELS LTD 7 Clive Avenue, Hastings, East Sussex, TN35 5LD, United Kingdom UK Accessories 68 CAVENDISH UPHOLSTERY LIMITED Mayfield Mill, Briercliffe Road, Chorley Lancashire PR6 0DA, United Kingdom UK Furniture 33 66% 34% FUZHOU BEST ART & CRAFTS CO., LTD No. 3 Building, Lifu Plastic, Nanshanyang Industrial Zone, Baisha Town, Minhou, Fuzhou, China CHINA Homewares 44 41% 59% HUAHONG HOLDING GROUP No. -

Results Announcement for the Year Ended December 31, 2020
(GDR under the symbol "HTSC") RESULTS ANNOUNCEMENT FOR THE YEAR ENDED DECEMBER 31, 2020 The Board of Huatai Securities Co., Ltd. (the "Company") hereby announces the audited results of the Company and its subsidiaries for the year ended December 31, 2020. This announcement contains the full text of the annual results announcement of the Company for 2020. PUBLICATION OF THE ANNUAL RESULTS ANNOUNCEMENT AND THE ANNUAL REPORT This results announcement of the Company will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism), and the website of the Company (www.htsc.com.cn), respectively. The annual report of the Company for 2020 will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of the National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism) and the website of the Company in due course on or before April 30, 2021. DEFINITIONS Unless the context otherwise requires, capitalized terms used in this announcement shall have the same meanings as those defined in the section headed “Definitions” in the annual report of the Company for 2020 as set out in this announcement. By order of the Board Zhang Hui Joint Company Secretary Jiangsu, the PRC, March 23, 2021 CONTENTS Important Notice ........................................................... 3 Definitions ............................................................... 6 CEO’s Letter .............................................................. 11 Company Profile ........................................................... 15 Summary of the Company’s Business ........................................... 27 Management Discussion and Analysis and Report of the Board ....................... 40 Major Events.............................................................. 112 Changes in Ordinary Shares and Shareholders .................................... 149 Directors, Supervisors, Senior Management and Staff.............................. -

Vessel Navigation Safety Analysis and Countermeasures in the Water of Taizhou Yangtze River Bridge
World Maritime University The Maritime Commons: Digital Repository of the World Maritime University Maritime Safety & Environment Management Dissertations Maritime Safety & Environment Management 8-28-2016 Vessel navigation safety analysis and countermeasures in the water of Taizhou Yangtze River Bridge Guojin Han Follow this and additional works at: https://commons.wmu.se/msem_dissertations Part of the Environmental Studies Commons, and the Risk Analysis Commons This Dissertation is brought to you courtesy of Maritime Commons. Open Access items may be downloaded for non-commercial, fair use academic purposes. No items may be hosted on another server or web site without express written permission from the World Maritime University. For more information, please contact [email protected]. 你 WORLD MARITIMEd UNIVERSITY Dalian, China VESSEL NAVIGATION SAFETY ANALYSIS AND COUNTERMEASURES IN THE WATER OF TAIZHOU YANGTZE RIVER BRIDGE By HAN GUOJIN The People’s Republic of China A dissertation submitted to the World Maritime University in partial Fulfillment of the requirements for the award of the degree of MASTER OF SCIENCE (MARITIME SAFETY AND ENVIRONMENTAL MANAGEMENT) 2016 © Copyright Han Guojin, 2016 I DECLARATION I certify that all the materials in this paper that are not my own work have been identified, and that no material is included for which a degree has previously been conferred on me. The contents of this paper reflect my own personal views, and are not necessarily endorsed by the University. Signature: Han Guojin Date: August 5, 2016 Supervised by: Li Tieshan Professor Dalian Maritime University Assessor: Co-assessor: II ACKNOWLEDGEMENTS This paper is developed as an important part of my studies to apply for the master’s degree of Maritime Safety and Environmental Management (MSEM) at World Maritime University (WMU) and Dalian Maritime University (DMU).