Orthodontic Treatment of Class Three Malocclusion Using Clear Aligners
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Class III Malocclusion Treated Non-Surgically with Invisalign, Mandibular Fixed Appliances and Mandibular Tads by Randy J
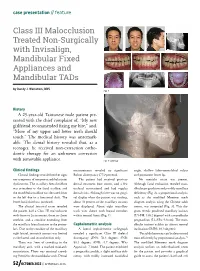
case presentation // feature Class III Malocclusion Treated Non-Surgically with Invisalign, Mandibular Fixed Appliances and Mandibular TADs by Randy J. Weinstein, DDS Fig. 1 History A 25-year-old Taiwanese male patient pre- sented with the chief complaint of, “My new girlfriend recommended fixing my bite,” and, “More of my upper and lower teeth should touch.” The medical history was unremark- able. The dental history revealed that, as a teenager, he received non-extraction ortho- dontic therapy for an unknown correction with removable appliance. Fig. 2: Overlay Clinical findings measurements revealed no significant angle, shallow labio-mentolabial sulcus Clinical findings revealed neither signs Bolton discrepancy (77.9 percent). and prominent lower lip. nor symptoms of temporomandibular joint The patient had received previous No mentalis strain was present. dysfunction. The maxillary dental midline dental treatment (one crown, and a few Although facial evaluation revealed man- was coincident to the facial midline, and occlusal restorations) and had regular dibular prognathism and possibly maxillary the mandibular midline was deviated 2mm dental visits. Although there was no gingi- deficiency (Fig. 2), a proportional analysis, to the left due to a functional shift. The val display when the patient was smiling, such as the modified Moorrees mesh lower facial third was increased. about 70 percent of the maxillary incisors diagram analysis using the Chinese adult The clinical intraoral exam revealed were displayed. About eight maxillary norms, was computed (Fig. 3). This dia- the patient had a Class III malocclusion teeth were shown with buccal corridors gram reveals proclined maxillary incisors with 0mm to 2mm overjet, 0mm to -2mm within normal limits (Fig. -

An Overview on Interproximal Enamel Reduction
DENTISTRY ISSN 2377-1623 http://dx.doi.org/10.17140/DOJ-1-104 Open Journal Review An Overview on Interproximal Enamel *Corresponding author Reduction Yanqi Yang Assistant Professor in Orthodontics Faculty of Dentistry, the University of Deborah Chee#, Chong Ren# and Yanqi Yang* Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Sai Ying #equally contributed Pun, Hong Kong, China Tel. +852-28590252 Orthodontics, Faculty of Dentistry, the University of Hong Kong, 34 Hospital Road, Hong Kong Fax: +852-25593803 SAR, China E-mail: [email protected] Volume 1 : Issue 1 ABSTRACT Article Ref. #: 1000DOJ1104 Ever since its first introduction seven decades ago, there has been continuous advance- ment of the concept and technique of Interproximal enamel reduction (IPR). It’s demonstrated Article History that with correct case selection and clinical performance, IPR is safe and effective for alleviat- Received: October 28th, 2014 ing crowding, improving dental and gingival aesthetics as well as facilitating post-treatment Accepted: December 5th, 2014 stability. The fulfilment of treatment outcomes depends on careful pre-treatment examination Published: December 8th, 2014 and planning, appropriate clinical procedures and effective post-treatment protection. This re- view aims to provide a general introduction to IPR in terms of its history background, risks and Citation benefits and clinical performance. Chee D, Ren C, Yang Y. An overview on interproximal enamel reduction. Dent Open J. 2014; 1(1): 14-18. doi: KEYWORDS: Interproximal enamel reduction; Orthodontic treatment; Crowding; Tooth re- 10.17140/DOJ-1-104 contouring. INTRODUCTION Interproximal enamel reduction (IPR) also described as “stripping”, “reproximation” and “slenderizing” has been applied in clinical orthodontics for almost seven decades.1,2 By removing part of the enamel tissue from the interproximal contact area, this technique has been proved to be effective in improving dental alignment, stability and aesthetics. -

Enhancing the Predictability of Clear Aligners
Enhancing Predictability of Clear Aligners Bowman DRASTIC PLASTIC: ENHANCING THE PREDICTABILITY OF CLEAR ALIGNERS S. Jay Bowman ABSTRACT Once limitations of clear aligner treatments were identified, conceptualizing techniques to improve the predictability in producing desired results was the next logical step. A variety of concepts, methods, and adjuncts have subsequently been introduced to enhance the efficiency and effectiveness of clear aligners. As a consequence, the scope of biomechanics and type of malocclusions that can be more predictably treated has increased. As one example, the inclusion of miniscrew temporary skeletal anchorage has permitted the addition of direct and indirect anchorage to support and control more predictable programmed tooth movements with aligners. After reviewing the reported shortcomings of plastic aligners, this chapter explores possibilities for improving predictability of aligner therapy. KEY WORDS: Clear Aligners, Miniscrews, Bootstrap Elastic, Attachments, Bonded Buttons INTRODUCTION It has been 20 years since the introduction of a commercialized clear aligner product to the orthodontic marketplace. Based on suggestion by Harold D. Kesling over 50 years earlier, Invisalign and later, increasingly numerous propriety alternatives have come to pass; including the exponential growth of so-called direct-to-consumer (DTC or DIY) offerings [1]. From the original questions of whether even “acceptable” results could be obtained from a sequence of aligners, these queries have now evolved into: Is an orthodontist even needed to be interjected between the manufacturer’s plastic and their “customers?” So, the idea of moving teeth with plastic was nothing new, but the use of software to attempt to predict desired tooth movement and the associated 3D representations of individual tooth position were innovative. -
Motion 3D Q&A
THE SAGITTAL FIRST REVOLUTION CARRIERE® MOTION 3D™ Q&A Join the REVOLUTION! #TheHappinessRevolution CLINICAL ADVICE PROVIDED BY: Dr. Carrière received his dental degree from the University of Complutense in Madrid, in 1991. He then attended the University of Barcelona where Dr. Carrière completed his Orthodontic training and received his Master of Science in Orthodontics in 1994. In 2006, he received his Doctorate in Orthodontics, Cum Laude, from the University of Barcelona. Dr. Carrière was the Winner of the prestigious “Joseph E. Johnson Award” and the International Design Award Delta Gold ADI-FAD 2009 for the “Carriere Distalizer MB”. Dr. Carrière is also a Member of the Editorial Review Board for the American Journal of Orthodontics and Dentofacial Orthopedics. As an invited professor of several Orthodontic departments throughout the world, Dr. Carrière lectures internationally when he is not treating patients in his private practice in Barcelona, Spain. Dr. Luis Carrière Dr. Paquette received his dental degree from UNC School of Dentistry in 1979 and a Master’s in Pediatric Dentistry from UNC in 1983. His Master’s thesis won a national research award that same year. He is board certified by the American Board of Pediatric Dentistry. He obtained his Master’s degree and specialty certificate in orthodontics from the St. Louis University in 1990. Dr. Paquette’s Master’s thesis in orthodontics won the coveted Milo Hellman award in 1991. He is an active member of the Schulman Group. Dr. Paquette is passionate about advancing the art and science of orthodontics. He has published numerous articles and lectures nationally and internationally. -

Orthodontics & Esthetic Dentistry
SCIENTIFIC SESSION TORONTO 2016 ORTHODONTICS & ESTHETIC DENTISTRY: MISSION POSSIBLE! A Broader Approach to Interdisciplinary Esthetic Treatment David M. Sarver, DMD, MS AACD 2016 TORONTO: THURSDAY MORNING “TRIPLE PLAY!” One Session. One Theme. Three Big Hitters. Dr. David M. Sarver, along with Dr. J. William Robbins and Dr. Jeffrey Rouse, will “cover the bases” on diagnosis, decision making, and treatment planning. These three “big hitters” will be presenting sequentially in the same room on Thursday, April 28, 2016. Dr. Sarver will present “Orthodontics— How it Has Changed and What You Really Want to Know!” This article discusses how orthodontics is incorporating smile design principles into its overall functional and esthetic treatment goals. Abstract For decades, dentistry has been evolving into a Patients seeking esthetic profession that is extremely multifaceted and varied in its approach to both smile and facial esthetics. treatment today wish to The coordination of macro esthetics (the face), mini enhance their appearance esthetics (the smile), and micro esthetics (the dental for improved self-esteem esthetic component) offers a complete approach to esthetic planning. This article presents an expanded and quality of life. vision of esthetic treatment designed to take readers to another level of facial, smile, and dental esthetic planning that can elevate patient outcomes. Key Words: macro esthetics, mini esthetics, micro esthetics, orthodontics, smile design 14 Winter 2016 • Volume 31 • Number 4 Sarver Figure 1: In both multidisciplinary and orthodontic diagnosis, three esthetic divisions are advocated: macro esthetics (the face), mini esthetics (the smile), and micro esthetics (the teeth). …there are principles of cosmetic dentistry that orthodontists can use to enhance their work to provide a superior esthetic outcome. -

TITLE PAGE Treatment Outcome with Orthodontic Aligners and Fixed
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2020 Treatment outcome with orthodontic aligners and fixed appliances: a systematic review with meta-analyses Papageorgiou, Spyridon N ; Koletsi, Despina ; Iliadi, Anna ; Peltomaki, Timo ; Eliades, Theodore Abstract: Background: The use of orthodontic aligners to treat a variety of malocclusions has seen considerable increase in the last years, yet evidence about their efficacy and adverse effects relative to conventional fixed orthodontic appliances remains unclear. Objective: This systematic review assesses the efficacy of aligners and fixed appliances for comprehensive orthodontic treatment. Search methods: Eight databases were searched without limitations in April 2019. Selection criteria: Randomized or matched non-randomized studies. Data collection and analysis: Study selection, data extraction, and risk of bias assessment was done independently in triplicate. Random-effects meta-analyses of mean differences (MDs) or relative risks (RRs) with their 95% confidence intervals (CIs) were conducted, followed by sensitivity analyses, and the GRADE analysis of the evidence quality.Results: A total of 11 studies (4 randomized/7 non-randomized) were included comparing aligners with braces (887 patients; mean age 28.0 years; 33% male). Moderate quality evidence indicated that treatment with orthodontic aligners is associated with worse occlusal outcome with the American Board of Orthodontics Objective Grading System (3 studies; MD = 9.9; 95% CI = 3.6-16.2) and more patients with unacceptable results (3 studies; RR = 1.6; 95% CI = 1.2-2.0). No significant differences were seen for treatment duration. The main limitations of existing evidence pertained to risk of bias, inconsistency, and imprecision of included studies. -

An Overview on Interproximal Enamel Reduction Review
DENTISTRY ISSN 2377-1623 http://dx.doi.org/10.17140/DOJ-1-104 Open Journal Review An Overview on Interproximal Enamel *Corresponding author Reduction Yanqi Yang Assistant Professor in Orthodontics Faculty of Dentistry, the University of Deborah Chee#, Chong Ren# and Yanqi Yang* Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Sai Ying #equally contributed Pun, Hong Kong, China Tel. +852-28590252 Orthodontics, Faculty of Dentistry, the University of Hong Kong, 34 Hospital Road, Hong Kong Fax: +852-25593803 SAR, China E-mail: [email protected] Volume 1 : Issue 1 ABSTRACT Article Ref. #: 1000DOJ1104 Ever since its first introduction seven decades ago, there has been continuous advance- ment of the concept and technique of Interproximal enamel reduction (IPR). It’s demonstrated Article History that with correct case selection and clinical performance, IPR is safe and effective for alleviat- Received: October 28th, 2014 ing crowding, improving dental and gingival aesthetics as well as facilitating post-treatment Accepted: December 5th, 2014 stability. The fulfilment of treatment outcomes depends on careful pre-treatment examination Published: December 8th, 2014 and planning, appropriate clinical procedures and effective post-treatment protection. This re- view aims to provide a general introduction to IPR in terms of its history background, risks and Citation benefits and clinical performance. Chee D, Ren C, Yang Y. An overview on interproximal enamel reduction. Dent Open J. 2014; 1(1): 14-18. doi: KEYWORDS: Interproximal enamel reduction; Orthodontic treatment; Crowding; Tooth re- 10.17140/DOJ-1-104 contouring. INTRODUCTION Interproximal enamel reduction (IPR) also described as “stripping”, “reproximation” and “slenderizing” has been applied in clinical orthodontics for almost seven decades.1,2 By removing part of the enamel tissue from the interproximal contact area, this technique has been proved to be effective in improving dental alignment, stability and aesthetics. -
Important Message
WE INTERRUPT YOUR REGULARLY SCHEDULED PROGRAM FOR AN IMPORTANT MESSAGE Q1 2018 inside this Disrupted: edition... New Rules for a New Type of Customer By Angela Weber, CMO OrthoSynetics Page 34 BUSINESS PRACTICE & DEVELOPMENT TRAVEL & LEISURE CLINICAL CORNER 18 15 37 From the Rear View Mirror Pro Travel Tips High Frequency Vibration Can BY DR. COURTNEY DUNN BY PROORTHO STAFF Reduce or Eliminate Pain During Aligner Treatment 30 20 BY DR. JONATHAN L. NICOZISIS Traveling to the Greek Islands New Gaidge CEO BY DR. DANIELA LOEBL INTERVIEW WITH RYAN MOYNIHAN 32 OFFICE LOGISTICS 34 Traveling to Peru Disrupted: New Rules for a New BY DR. DAVID WALKER 56 Type of Customer Beyond Reminders: BY ANGELA WEBER, CMO ORTHOSYNETICS 40 Tapping the Potential of Texting Traveling to Spain BY DR. KEITH DRESSLER 44 BY DR. DAVID MAJERONI What Would You Do If an Aligner 46 Store Opened Down the Street? ORTHOPUNDIT.COM BY DR. JENNIFER EISENHUTH Traveling to Europe BY DR. BEN BURRIS & BRIDGET BURRIS 09 MARKETING/ H.R. INSIGHT Don't Piss Momma Off! SOCIAL MEDIA BY DR. BEN BURRIS 05 28 24 Go High or Go Low - Just Don't Get Utilize Group Interviews To Made to Measure: Stuck in the Middle Maximize Hiring Success The Dubious Relationship Between BY DR. LEON KLEMPNER AND AMY EPSTEIN, BY BRIDGET BURRIS Eugenics and Orthodontics MBA ANSWERS FROM THE BY DR. MARC ACKERMAN 52 EDGE 59 5 Keys to Capturing the Fastest The Economy Is Booming – Why Growing Referral Source 10 Isn’t Your Practice? BY NICK DUNCAN Interviews with Dr. Jeff Kozlowski BY DR. -

Movingnot Removing Enamel
VOLUME 01 / ISSUE 01 The Academy for Clear Aligner Therapy the AmericanJournal Academy of Cosmetic Orthodontics MOVING not removing ENAMEL. PEER-REVIEWED SOLUTIONS that will make Clear Aligner Treatment THAT MUCH EASIER. Like this Journal? start receiving your quarterly issue today! The official academy for Clear Aligner Therapy. Become a member TODAY! www.aacortho.com AACO Board Members Dr. David Galler: President the Dr. Mark Hodge: Vice President Dr. Perry Jones: Director of Education Dr. Jeffrey Galler: Editor AmericanJournal Academy of Cosmetic Orthodontics Dr. Len Tau: Director of Media Relations Dr. Bruce McFarlane: Orthodontist, Advisory Board Article is Peer Reviewed Article offers CE Credit at www.aacortho.com Dr. David Harrnick: Orthodontist, Advisory Board Dr. Sandi Bosin: Orthodontist, Editorial Board Case Reports Dr. Peter Rivolli: ClearCorrect Clinical Expert Dr. Yana Shampanksy: Invisalign Expert 2 Upper Lateral Incisor Crossbite with Dr. Lori Trost: MTM Clinical Expert Lower Premolar in Lingual Version by Dr. Cathy Sherry 4 Invisalign Correction of a Teenager’s Class 2 Division 1 Malocclusion by Dr. David J. Harnick 8 Upper Arch Spacing and Lower Editorial Arch Overcrowding I’ve been reading numerous by Dr. David Galler dental journals every Practice Development month for many years, 14 The Economics of Buying vs. but don’t remember ever Renting Your Next Office actually reading an editorial completely, from beginning by Jake Jacklich to end. 16 “Doctor, I’ve been your patient for I resolved that in this, my first 10 years; how come you never editorial for the Journal of the American mentioned orthodontics before?” Academy of Cosmetic Orthodontics, by Gary Kadi I would write an editorial that readers Retention would, in fact, read from the very first to the very last word. -

SMILEDIRECTCLUB, INC. (Exact Name of Registrant As Specified in Its Charter)
UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, D.C. 20549 FORM 10-K ☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the annual period ended December 31, 2019 or ☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the transition period from ________ to________ Commission File Number: 001-39037 SMILEDIRECTCLUB, INC. (Exact name of registrant as specified in its charter) Delaware 83-4505317 (State or other jurisdiction of incorporation or organization) (I.R.S. Employer Identification No.) 414 Union Street Nashville, TN 37219 (Address of principal executive offices) (Zip Code) (800) 848-7566 (Registrant’s telephone number, including area code) Not applicable (Former name, former address and former fiscal year, if changed since last report) Securities registered pursuant to Section 12(b) of the Act: Title of each class Trading Symbol(s) Name of each exchange on which registered Class A common stock, par value $0.0001 per share SDC The NASDAQ Stock Market LLC Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. ☐ Yes ☒ No Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. ☐ Yes ☒ No Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. -
3D Airway Changes Using CBCT in Patients Following Mandibular Setback Surgery ± Maxillary Advancement
Received: 5 December 2018 | Accepted: 7 December 2018 DOI: 10.1111/ocr.12291 SUPPLEMENT ARTICLE 3D Airway changes using CBCT in patients following mandibular setback surgery ± maxillary advancement Andrew G. Havron1 | Sharon Aronovich2 | Anita V. Shelgikar3 | H. Ludia Kim4 | R. Scott Conley5 1Department of Orthodontics and Pediatric Dentistry, University of Michigan, Ann Structured Abstract Arbor, Michigan Introduction: The aim of this study was to determine the 3D airway changes that 2 Department of Oral and Maxillofacial occur following mandibular setback surgery alone vs bimaxillary surgery in patients Surgery, University of Michigan, Ann Arbor, Michigan with similar skeletal start forms. 3Department of Neurology, University of Setting and Sample Population: The University of Michigan School of Dentistry and Michigan, Ann Arbor, Michigan Medical Center. A total of 85 patients undergoing mandibular setback with or with- 4Private Practice, Ann Arbor, Michigan out simultaneous maxillary advancement. 5Department of Orthodontics, University at Buffalo, Buffalo, New York Materials and Methods: A retrospective evaluation of pre- and post- surgical CBCT scans for patients undergoing mandibular setback surgery alone (14) vs bimaxillary Correspondence R. Scott Conley, University at Buffalo School surgery (71) was performed. Cross- sectional evaluation at standardized locations, of Dental Medicine, Buffalo, NY. minimum cross section and volumetric analysis were performed (Dolphin Imaging & Email: [email protected] Management Solutions). Results: Patients who underwent mandibular setback surgery alone showed a statis- tically significant average increase of 47.5 mm2 in minimum axial area. Patients who underwent bimaxillary surgery showed a statistically significant increase in airway volume, minimum axial area, location of minimum axial area, and axial area at the re- tropalatal and retroglossal regions. -

Journal of Cosmetic Dentistry
Journal of Cosmetic Dentistry Rubber Dam First Calin Pop, DDS Analysis with Imaging & Photography Conservative Composite Bonding 2020 VOLUME 36 ISSUE 3 “We asked, they delivered!” Based on AACD members’ feedback, Ivoclar Vivadent developed a NEW Higher Viscocity Veneer Cement. Amanda Seay, DDS, FAACD INTRODUCING Variolink® Esthetic LC HV Higher viscosity light curing cement • Controlled seating GET YOUR FREE REFILL AT • Precise cleanup blog.ivoclarvivadent.us/free-variolink-sample • Ideal for veneers ivoclarvivadent.com For more information, call us at 1-800-533-6825 in the U.S., 1-800-263-8182 in Canada. © 2020 Ivoclar Vivadent, Inc. Ivoclar Vivadent and Variolink are registered trademarks of Ivoclar Vivadent, Inc. 13722_VE LC HV_JCD.indd 1 11/3/20 3:51 PM A PEER-REVIEWED PUBLICATION OF THE AMERICAN ACADEMY OF COSMETIC DENTISTRY EDITORIAL REVIEW BOARD Pinhas Adar, MDT, CDT, Atlanta, GA Irfan Ahmad, BDS, Middlesex, United Kingdom Somkiat Aimplee, DDS, MSc, AAACD, Bangkok, Thailand volume 36 issue 3 Gary Alex, DMD, AAACD, Huntington, NY Journal of Cosmetic Dentistry Edward P. Allen, DDS, PhD, Dallas, TX Chad J. Anderson, DMD, MS, Fresno, CA Elizabeth M. Bakeman, DDS, FAACD, Grand Rapids, MI Lee Ann Brady, DMD, Glendale, AZ Kevin M. Brown, DDS, AAACD, Bellevue, WA Ricardo M. Carvalho, DDS, PhD, Vancouver, BC, Canada EDITOR-IN-CHIEF Edward Lowe, DMD, AAACD Christian Coachman, DDS, CDT, Sáo Paulo, Brazil Vancouver, BC, Canada, [email protected] John C. Cranham, DDS, Chesapeake, VA EXECUTIVE DIRECTOR Barbara J. Kachelski, MBA, CAE, [email protected] Michael W. Davis, DDS, Santa Fe, NM Newton Fahl Jr., DDS, MS, Curitiba-PR, Brazil CHIEF MARKETING OFFICER Mike DiFrisco, CAE, [email protected] Jonathan L.