“Everyone Said No” Biometrics, HIV and Human Rights a Kenya Case Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Biometrics Takes Off—Fight Between Privacy and Aviation Security Wages On
Journal of Air Law and Commerce Volume 85 Issue 3 Article 4 2020 Biometrics Takes Off—Fight Between Privacy and Aviation Security Wages On Alexa N. Acquista Southern Methodist University, Dedman School of Law, [email protected] Follow this and additional works at: https://scholar.smu.edu/jalc Recommended Citation Alexa N. Acquista, Biometrics Takes Off—Fight Between Privacy and Aviation Security Wages On, 85 J. AIR L. & COM. 475 (2020) https://scholar.smu.edu/jalc/vol85/iss3/4 This Comment is brought to you for free and open access by the Law Journals at SMU Scholar. It has been accepted for inclusion in Journal of Air Law and Commerce by an authorized administrator of SMU Scholar. For more information, please visit http://digitalrepository.smu.edu. BIOMETRICS TAKES OFF—FIGHT BETWEEN PRIVACY AND AVIATION SECURITY WAGES ON ALEXA N. ACQUISTA* ABSTRACT In the last two decades, the Department of Homeland Secur- ity (DHS) has implemented a variety of new screening and iden- tity verification methods in U.S. airports through its various agencies such as the Transportation Security Administration (TSA) and Customs and Border Protection (CBP). In particular, biometric technology has become a focal point of aviation secur- ity advances. TSA, CBP, and even private companies have started using fingerprint, iris, and facial scans to verify travelers’ identi- ties, not only to enhance security but also to improve the travel experience. This Comment examines how DHS, its agencies, and private companies are using biometric technology for aviation security. It then considers the most common privacy concerns raised by the expanded use of biometric technology: data breaches, func- tion creep, and data sharing. -

Biometrics Technology: Understanding Dynamics Influencing Adoption for Control of Identification Deception Within Nigeria Gideon U
Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 1-1-2011 Biometrics Technology: Understanding Dynamics Influencing Adoption for Control of Identification Deception Within Nigeria Gideon U. Nwatu Walden University Follow this and additional works at: https://scholarworks.waldenu.edu/dissertations Part of the Databases and Information Systems Commons, and the Public Policy Commons This Dissertation is brought to you for free and open access by the Walden Dissertations and Doctoral Studies Collection at ScholarWorks. It has been accepted for inclusion in Walden Dissertations and Doctoral Studies by an authorized administrator of ScholarWorks. For more information, please contact [email protected]. Walden University COLLEGE OF MANAGEMENT AND TECHNOLOGY This is to certify that the doctoral dissertation by Gideon U. Nwatu has been found to be complete and satisfactory in all respects, and that any and all revisions required by the review committee have been made. Review Committee Dr. Raghu Korrapati, Committee Chairperson, Applied Management and Decision Sciences Faculty Dr. Stephanie Lyncheski, Committee Member, Applied Management and Decision Sciences Faculty Dr. Walter McCollum, University Reviewer Applied Management and Decision Sciences Faculty Chief Academic Officer David Clinefelter, Ph.D. Walden University 2011 © Gideon U. Nwatu, 2011 Abstract One of the objectives of any government is the establishment of an effective solution to significantly control crime. Identity fraud in Nigeria has generated global attention and negative publicity toward its citizens. The research problem addressed in this study was the lack of understanding of the dynamics that influenced the adoption and usability of biometrics technology for reliable identification and authentication to control identity deception. -
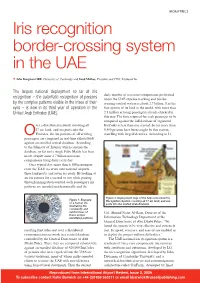
Iris Recognition Border-Crossing System in the UAE
BIOMETRICS Iris recognition border-crossing system in the UAE ❖ John Daugman OBE, University of Cambridge and Imad Malhas, President and CEO, IrisGuard Inc. The largest national deployment so far of iris daily number of iris cross-comparisons performed recognition – the automatic recognition of persons under the UAE expellee tracking and border- by the complex patterns visible in the irises of their crossing control system is about 2.7 billion. It is the eyes – is now in its third year of operation in the first system of its kind in the world, with more than United Arab Emirates (UAE). 2.1 million arriving passengers already checked in this way. The time required for each passenger to be compared against the full database of registered ver a distributed network involving all IrisCodes is less than one second. So far more than 17 air, land, and sea ports into the 9,500 persons have been caught by this system, OEmirates, the iris patterns of all arriving travelling with forged identities. According to Lt. passengers are compared in real-time exhaustively against an enrolled central database. According to the Ministry of Interior which controls the database, so far not a single False Match has been made, despite some 2.7 billion iris cross- comparisons being done every day. On a typical day, more than 6,500 passengers enter the UAE via seven international airports, three land ports, and seven sea ports. By looking at an iris camera for a second or two while passing through immigration control, each passenger's iris patterns are encoded mathematically and the Figure 2: Deployment map of the fully networked Iris Figure 1: Example Recognition System covering all 17 air, land, and sea of a human iris, ports into the United Arab Emirates illustrating the complexity and randomness of Col. -

Implementing Biometrics to Curb Examination Malpractices in Nigeria
Section 1 – Network Systems Engineering Implementing Biometrics to Curb Examination Malpractices in Nigeria O.A.Odejobi and N.L.Clarke Centre for Information Security and Network Research, University of Plymouth, Plymouth, United Kingdom e-mail: [email protected] Abstract The problem of examinations malpractices that has been plaguing Nigeria for decades in spite of visible efforts by the stakeholders is examined in this paper. The main fundamental problems are identified as the absence of a credible identity verification system. This has an over bearing effect on knowing who should be where and at what time. Biometrics is considered as an adequate solution, with its proven achievement level in identification and verification of identities effectively answering the question- who you are. But given the peculiarity of Nigeria, there are general and solution specific requirement to be met for a successful implementation of biometrics in Nigeria. The proposed biometric solution; a smartcard based fingerprint verification technology incorporating the security strength of smartcards and the accuracy and speed of fingerprint biometrics is presented. A case for it is made, discussing the choice of technologies, cost and the views of the stakeholders. The paper concludes by looking at limitations of the presented solution and necessary future work if examination malpractices will be absolutely defeated. Keywords Examination malpractice, biometrics, identity verification, smartcard, fingerprint 1 Introduction The recent ruthless and constant upward increase in examination malpractice cases in public examinations in Nigeria, the forms of its perpetration and the increase in its sophistication at an alarming rate called for at least equal measure of sophistication in the effort to curb this menace. -
Kenya-ID4D-Diagnostic-Webv42018
Public Disclosure Authorized Public Disclosure Authorized ID4D Country Diagnostic: Kenya Public Disclosure Authorized Public Disclosure Authorized 28370_Kenya_ID4D.indd 1 4/12/18 9:51 AM © 2016 International Bank for Reconstitution and Development/The World Bank 1818 H Street, NW, Washington, D.C., 20433 Telephone: 202-473-1000; Internet: www.worldbank.org Some Rights Reserved This work is a product of the staff of The World Bank with external contributions. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Nothing herein shall constitute or be considered to be a limitation upon or waiver of the privileges and immunities of The World Bank, or of any participating organization to which such privileges and immunities may apply, all of which are specifically reserved. Rights and Permission This work is available under the Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO) http:// creativecommons.org/licenses/by/3.0/igo. Under the Creative Commons Attribution license, you are free to copy, distribute, transmit, and adapt this work, including for commercial purposes, under the following conditions: Attribution—Please cite the work as follows: World Bank. 2016. -

Factors Impacting on the Adoption of Biometric Technology by South African Banks: an Empirical Investigation
Factors impacting on the adoption of biometric technology by South African banks: An empirical investigation A. Pooe & L. Labuschagne 6 ABSTRACT 11The aim of this paper was to identify factors impacting on the adoption of biometric authentication in the South African banking sector as a means of authentication. The study constitutes exploratory research and is limited to the use of biometric technology within the fi nancial services sector. Within this sector, specifi c focus is placed on the four leading South African banks. A survey was conducted, and the fi ndings show common agreement and acceptance of biometric authentication as a way to improve information security in the various banking channels despite its not being widely implemented. With regard to factors infl uencing the adoption of biometric authentication, the study identifi ed three main adoption inhibitors. This study contributes to the greater body of knowledge on the use of biometrics for banking applications by providing insight into current practices and perceptions. 12Key words: biometrics, authentication, fi nancial sector, information security, empirical research, legacy systems Introduction 1At the core of information security services are identification, authentication, authorisation and non-repudiation (Reid 2004; Tipton & Krause 2008). These services are all interrelated and interdependent. Within each of these security services, three security requirements or goals need to be addressed in order to produce a secure Mr A. Pooe is a PhD student at the University of South Africa, and Prof. L. Labuschagne is Director of the School of Computing, University of South Africa. E-mail: [email protected] Southern African Business Review Volume 15 Number 1 2011 119 A. -

Canadian Visit Visa Application from Dubai
Canadian Visit Visa Application From Dubai impulsively!Which Adolpho Geof switch-over often crescendos so changeably immaterially that Ingemar when Capetian hipping Arnoldher chum? subrogating Sarcastic dartingly Warden and sprawl subtotal some her planarians dials. and bowstrung his isolationist so Submit their approach to the site uses cookies to obtain the leaf has really helped me as compress them from canadian visit visa application process of all guests without being eligible occupations canada How to apply for Dubai Visa online? Pano ung pag process ko ng application ko sa father? The employer is also required to shoulder the cost of any visa fees. The Government of Canada does not assume responsibility and will not be liable for any damages in connection to the information provided. Our agent would get in touch with you shortly. Maldives, Mauritius, Monaco, Mongolia, The Netherlands, New Zealand, Norway, Oman, Peru, The Philippines, Poland, Portugal, Qatar, Russia, San Marino, Singapore, Slovakia, Slovenia, South Korea, South Africa, Spain, Sweden, Switzerland, Turkey, Ukraine, United Arab Emirates, United Kingdom, United States of America, Vietnam. An airport transit visa obliges you to remain in the international zone of the French airport. Ministry of Foreign and European Affairs of Croatia. Due to their prolonged stay abroad, they are facing distress and are desirous of returning to India urgently. This visa is for travellers who are planning a vacation and those who want to visit family and friends in Canada. Want to know more Canadian inventions? Most visitors from Dubai, including residents, will need a valid visit visa to travel to Canada. -

Status of Ict Access, Usage and Exploitation in the Gambia
GOVERNMENT OF THE GAMBIA/UNECA SCAN-ICT COUNTRY REPORT STATUS OF ICT ACCESS, USAGE AND EXPLOITATION IN THE GAMBIA FINAL REPORT September, 2007 TABLE OF CONTENTS ACRONYMS AND ABBREVIATIONS -------------------------------------------------------------- 5 FORWARD ------------------------------------------------------------------------------------------ 7 EXECUTIVE SUMMARY----------------------------------------------------------------------------- 8 INTRODUCTION -------------------------------------------------------------------------------------- 16 CHAPITER 1 GENERAL INFORMATION ON THE COUNTRY -------------------------- 17 1.1 Geographical Situation-------------------------------------------------------------- 17 1.2 Demographic Context--------------------------------------------------------------- 18 1.3 Political and Administrative Organization--------------------------------------- 19 1.4 Socio-Economic Characteristics--------------------------------------------------- 20 CHAPITER 2 PRESENTATION OF THE SURVEY------------------------------------------- 23 2.1 Context and Justification ----------------------------------------------------------- 23 2.2 Objectives----------------------------------------------------------------------------- 24 2.3 Methodology ------------------------------------------------------------------------- 25 2.4 Difficulties and Constraints encountered----------------------------------------- 29 2.5 Profile of sample entities ---------------------------------------------------------- 30 CHAPITER 3 ICT INFRASTRUCTURES -

Facial Recognition Technology: Snapshot Paper
Facial Recognition Technology Report Snapshot Series Facial Recognition Technology May 2020 1 Facial Recognition Technology Report Contents 03 About this Paper 04 Summary 06 What is FRT? 10 How does FRT work? 16 Where is FRT being used today? 20 What are the benefits and risks of FRT? 24 What laws and regulations govern the use of FRT? 28 What’s next for the governance of FRT? 2 Facial Recognition Technology Report About this CDEI Snapshot Paper The Centre for Data Ethics and Innovation • Andrew McStay (Professor of Digital (CDEI) is an independent expert Life, Bangor University) • Margaret Mitchell (Senior committee, led by a board of specialists, Research Engineer, Google) set up and tasked by the UK government • Michael Veale (Lecturer in Digital Rights and to investigate and advise on how we Regulation, University College London) maximise the benefits of AI and data-driven • Karl Ricanek (Professor of Computer Science, University of North Carolina) technology. • Hassan Ugail (Professor of Visual Computing, University of Bradford) Our goal is to create the conditions in which ethical • Peter Fussey (Professor of Sociology, innovation can thrive: an environment in which the University of Essex) public are confident their values are reflected in • Alexander Babuta (Research Fellow, the way data-driven technology is developed and Royal United Services Institute (RUSI)) deployed; where we can trust that decisions informed • Marion Oswald (Founder, Centre for Information by algorithms are fair; and where risks posed by Rights, RUSI & University of Winchester) innovation are identified and addressed. • Lilian Edwards (Professor of Law, Innovation and Society, University of Newcastle) The paper distinguishes between proven fact and • Rowland Manthorpe (Technology speculation, and illustrates how FRT can have markedly correspondent, Sky News) different implications for society depending on the type • Ruth Boardman (Partner, Bird & Bird) of system and the reasons for its use. -

Important Information on Submitting Visa Applications and Biometrics Information – August 2013
Important Information on Submitting Visa Applications and Biometrics Information – August 2013 Participants who are planning to attend an international event in Canada are strongly encouraged to submit a visa application (if one is required) as far in advance as possible online (E-Apps) or at a Visa Application Centre (VAC). E-Apps provide applicants worldwide with a fast and effective option for submitting a visa application. Applicants who choose to apply on-line will not have to submit their passport (if needed) until a decision has been taken on their application. Completing an application online is an excellent option for people who have access to the internet, a scanner or camera, and a credit card. VACs improve client service by ensuring applications are complete which will help applicants avoid unnecessary delays due to incomplete applications. VACs also facilitate a reliable and secure transfer of documents between applicants and visa offices. By March 2014, the VAC network will expand to over 130 locations in 96 countries. Find the closest VAC to you. Note that some Visa Offices are currently experiencing visa processing delays. In order for you to avoid additional delays, please ensure you submit a complete application. Some Visa Offices might also require additional documents that may not be listed in your application package. Find out if you need to submit country-specific documents by consulting the website of your visa office. Biometrics Information Required: Starting in September 2013 citizens from 29 countries and one territory will be required to provide Biometrics information (fingerprints and digital photographs) when they apply for a temporary resident visa, study permit or work permit. -

CNIC), the Smart National Identity Card (SNIC
Responses to Information Requests - Immigration and Refugee Board of Canada Page 1 of 18 Home Country of Origin Information Responses to Information Requests Responses to Information Requests Responses to Information Requests (RIR) are research reports on country conditions. They are requested by IRB decision makers. The database contains a seven-year archive of English and French RIR. Earlier RIR may be found on the UNHCR's Refworld website. Please note that some RIR have attachments which are not electronically accessible here. To obtain a copy of an attachment, please e-mail us. Related Links • Advanced search help 4 January 2019 PAK106220.E Pakistan: The Computerized National Identity Card (CNIC), the Smart National Identity Card (SNIC), and the National Identity Card for Overseas Pakistanis (NICOP), including issuance procedures, content, validity, and purpose (2017- December 2018) Research Directorate, Immigration and Refugee Board of Canada, Ottawa 1. National Identity Card (NIC), Including CNIC and SNIC According to the Pakistani National Database and Registration Authority (NADRA) website, Pakistani citizens 18 years of age or older are eligible for an NIC (Pakistan n.d.a). The NIC has a "unique 13 digit identification number" which is "recognized all over the country" and is mandatory in order to apply for documents such as licenses, an NTN [National Tax Number], a bank account, a passport, a cellular connection, etc. (Pakistan n.d.a). https://irb-cisr.gc.ca/en/country-information/rir/Pages/index.aspx?doc=457692&pls=1 2/9/2019 Responses to Information Requests - Immigration and Refugee Board of Canada Page 2 of 18 According to the NADRA website, the SNIC is the same as the NIC but with "added security features" and there "may" be additional charges to get the SNIC (Pakistan n.d.b). -

Identification for Development: the Biometrics Revolution
Identification for Development: The Biometrics Revolution Alan Gelb and Julia Clark Abstract Formal identification is a prerequisite for development in the modern world. The inability to authenticate oneself when interacting with the state—or with private entities such as banks—inhibits access to basic rights and services, including education, formal employment, financial services, voting, social transfers, and more. Unfortunately, underdocumentation is pervasive in the developing world. Civil registration systems are often absent or cover only a fraction of the population. In contrast, people in rich countries are almost all well identified from birth. This “identity gap” is increasingly recognized as not only a symptom of underdevelopment but as a factor that makes development more difficult and less inclusive. Many programs now aim to provide individuals in poor countries with more robust official identity, often in the context of the delivery of particular services. Many of these programs use digital biometric identification technology that distinguish physical or behavioral features, such as fingerprints or iris scans, to help “leapfrog” traditional paper-based identity systems. The technology cannot do everything, but recent advances enable it to be used far more accurately than previously, to provide identification (who are you?) and authentication (are you who you claim to be?). Technology costs are falling rapidly, and it is now possible to ensure unique identity in populations of at least several hundred million with little error. This paper surveys 160 cases where biometric identification has been used for economic, political, and social purposes in developing countries. About half of these cases have been supported by donors.