Caring for Patients Receiving Vasopressors and Inotropes in the ICU
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nitric Oxide, the Biological Mediator of the Decade: Fact Or Fiction?
Eur Respir J 1997; 10: 699–707 Copyright ERS Journals Ltd 1997 DOI: 10.1183/09031936.97.10030699 European Respiratory Journal Printed in UK - all rights reserved ISSN 0903 - 1936 SERIES 'CLINICAL PHYSIOLOGY IN RESPIRATORY INTENSIVE CARE' Edited by A. Rossi and C. Roussos Number 14 in this Series Nitric oxide, the biological mediator of the decade: fact or fiction? S. Singh, T.W. Evans Nitric oxide, the biological mediator of the decade: fact or fiction? S. Singh, T.W. Evans. Unit of Critical Care, National Heart & ERS Journals Ltd 1997. Lung Institute, Royal Brompton Hospital, ABSTRACT: Nitric oxide (NO), an atmospheric gas and free radical, is also an London, UK. important biological mediator in animals and humans. Its enzymatic synthesis by constitutive (c) and inducible (i) isoforms of NO synthase (NOS) and its reactions Correspondence: T.W. Evans with other biological molecules such as reactive oxygen species are well charac- Royal Brompton Hospital Sydney Street terized. NO modulates pulmonary and systemic vascular tone through its vasodila- London SW3 6NP tor property. It has antithrombotic functions and mediates some consequences of UK the innate and acute inflammatory responses; cytokines and bacterial toxins induce widespread expression of iNOS associated with microvascular and haemodynam- Keywords: Acute respiratory distress syn- ic changes in sepsis. drome Within the lungs, a diminution of NO production is implicated in pathological hypoxic pulmonary vasoconstriction states associated with pulmonary hypertension, such as acute respiratory distress nitric oxide syndrome: inhaled NO is a selective pulmonary vasodilator and can improve ven- nitric oxide synthase tilation-perfusion mismatch. However, it may have deleterious effects through mod- pulmonary hypertension ulating hypoxic pulmonary vasoconstriction. -

Medicare National Coverage Determinations Manual, Part 1
Medicare National Coverage Determinations Manual Chapter 1, Part 1 (Sections 10 – 80.12) Coverage Determinations Table of Contents (Rev. 10838, 06-08-21) Transmittals for Chapter 1, Part 1 Foreword - Purpose for National Coverage Determinations (NCD) Manual 10 - Anesthesia and Pain Management 10.1 - Use of Visual Tests Prior to and General Anesthesia During Cataract Surgery 10.2 - Transcutaneous Electrical Nerve Stimulation (TENS) for Acute Post- Operative Pain 10.3 - Inpatient Hospital Pain Rehabilitation Programs 10.4 - Outpatient Hospital Pain Rehabilitation Programs 10.5 - Autogenous Epidural Blood Graft 10.6 - Anesthesia in Cardiac Pacemaker Surgery 20 - Cardiovascular System 20.1 - Vertebral Artery Surgery 20.2 - Extracranial - Intracranial (EC-IC) Arterial Bypass Surgery 20.3 - Thoracic Duct Drainage (TDD) in Renal Transplants 20.4 – Implantable Cardioverter Defibrillators (ICDs) 20.5 - Extracorporeal Immunoadsorption (ECI) Using Protein A Columns 20.6 - Transmyocardial Revascularization (TMR) 20.7 - Percutaneous Transluminal Angioplasty (PTA) (Various Effective Dates Below) 20.8 - Cardiac Pacemakers (Various Effective Dates Below) 20.8.1 - Cardiac Pacemaker Evaluation Services 20.8.1.1 - Transtelephonic Monitoring of Cardiac Pacemakers 20.8.2 - Self-Contained Pacemaker Monitors 20.8.3 – Single Chamber and Dual Chamber Permanent Cardiac Pacemakers 20.8.4 Leadless Pacemakers 20.9 - Artificial Hearts And Related Devices – (Various Effective Dates Below) 20.9.1 - Ventricular Assist Devices (Various Effective Dates Below) 20.10 - Cardiac -

Inorganic Nitrate As a Treatment for Acute Heart Failure
Falls et al. J Transl Med (2017) 15:172 DOI 10.1186/s12967-017-1271-z Journal of Translational Medicine PROTOCOL Open Access Inorganic nitrate as a treatment for acute heart failure: a protocol for a single center, randomized, double‑blind, placebo‑controlled pilot and feasibility study Roman Falls1,2, Michael Seman1,2, Sabine Braat2,4, Joshua Sortino1, Jason D. Allen1,3 and Christopher J. Neil1,2,3,5* Abstract Background: Acute heart failure (AHF) is a frequent reason for hospitalization worldwide and efective treatment options are limited. It is known that AHF is a condition characterized by impaired vasorelaxation, together with reduced nitric oxide (NO) bioavailability, an endogenous vasodilatory compound. Supplementation of inorganic sodium nitrate (NaNO3) is an indirect dietary source of NO, through bioconversion. It is proposed that oral sodium nitrate will favorably afect levels of circulating NO precursors (nitrate and nitrite) in AHF patients, resulting in reduced systemic vascular resistance, without signifcant hypotension. Methods and outcomes: We propose a single center, randomized, double-blind, placebo-controlled pilot trial, evaluating the feasibility of sodium nitrate as a treatment for AHF. The primary hypothesis that sodium nitrate treat- ment will result in increased systemic levels of nitric oxide pre-cursors (nitrate and nitrite) in plasma, in parallel with improved vasorelaxation, as assessed by non-invasively derived systemic vascular resistance index. Additional sur- rogate measures relevant to the known pathophysiology of AHF will be obtained in order to assess clinical efect on dyspnea and renal function. Discussion: The results of this study will provide evidence of the feasibility of this novel approach and will be of inter- est to the heart failure community. -

What Inotrope and Why?
What Inotrope and Why? a,b, a,b Nilkant Phad, MD, FRACP *, Koert de Waal, PhD KEYWORDS Hypotension Cardiovascular compromise Inotrope Newborn KEY POINTS There are significant gaps in the knowledge about diagnostic thresholds and choices of therapeutic interventions that can improve morbidity and mortality in neonates with car- diovascular compromise. Current use of inotropes in neonates is largely based on the pathophysiology of cardiovas- cular impairment and anticipated actions of inotropes because of limited outcome data from randomized controlled trials. Research studies of alternative study design unraveling the linkage of cardiovascular impairment and use of inotropes with important clinical outcomes are needed for future progress. INTRODUCTION The primary function of the cardiovascular system is to meet oxygen and nutritional demands of organs under various physiologic and pathologic conditions.1 To achieve this, the heart contracts against vascular resistance and drives blood to the lungs for oxygenation and into the systemic circulation for organ perfusion. The force of cardiac contraction, ventricular end-diastolic blood volume, and perfusion pressure are the main determinants of cardiovascular performance through an interplay between car- diac output (CO), vascular resistance, and neuroendocrine mechanisms.2 In neonates, the physiology of blood circulation can get disrupted in many clinical conditions, resulting in impaired organ perfusion and hypoxia. Persistent circulatory compromise can lead to derangement of metabolism, -

Inotropes, Vasopressors, and Chronotropes OH MY! a Review For
Inotropes, Vasopressors, and Chronotropes OH MY! A Review for the Young and the Seasoned MATT RUBERTUS, PHARMD CLINICAL PHARMACY SPECIALIST – CARDIOTHORACIC SURGERY/CRITICAL CARE EMORY UNIVERSITY HOSPITAL ATLANTA, GA Disclosure I have nothing to disclose pertaining to this presentation http://oz.wikia.com Objectives Review the mechanism of action for vasopressors and inotropes Recognize common side effects of different vasopressors and inotropes Review data for the use of alternative agents to treat vasoplegia Describe where angiotensin II fits into therapy Clinical Scenarios Shock Cardiogenic Vasodilatory Sepsis Cardiac Surgery Valve Disease Decompensated Heart Failure http://thefilmspectrum.com Hypotension Hypotension Baroreceptor Decreased Renal Activation Perfusion Increased RASS Activation Sympathetic Activity Cardiac Stimulation Vasoconstriction Volume Expansion Increased HR and Increased Preload Contractility Increased Cardiac Increased Systemic Increased Cardiac Output Vascular Resistance Output Increased Blood Pressure Hemodynamics The ultimate goal of cardiac function is perfusion Must deliver adequate oxygen to meet metabolic demand of end organs Oxygen delivery is affected by multiple factors Hemoglobin Oxygen saturation Cardiac output Cardiac Output (CO) = Heart Rate (HR) x Stroke Volume (SV) Hemodynamics Stroke Heart Rate CO = X Volume Rate Rhythm Preload Contractility Afterload CVP MAP Vasopressors http://thefilmspectrum.com Alpha Receptors Alpha1 Located in vascular smooth muscle Cause vasoconstriction -

Combination Therapy with Beta Blocker and Inotrope In
HEART RESEARCH ISSN 2377-164X http://dx.doi.org/10.17140/HROJ-4-136 Open Journal Case Report Combination Therapy With Beta Blocker *Corresponding author and Inotrope in Decompensated Heart Abhishek Jaiswal, MD Tulane University Heart and Vascular Institute Failure: A Clinical Observation Tulane School of Medicine 1430 Tulane Avenue, SL#48 New Orleans * LA 70112, USA Abhishek Jaiswal, MD ; Vinh Q. Nguyen, MD; Brendan Carry, MD; Thierry H. Le Jemtel, Tel. 1-504-988-1612 MD Fax: 1-504-988-4237 E-mail: [email protected] Tulane University Heart and Vascular Institute, Tulane School of Medicine, 1430 Tulane Avenue, SL#48, New Orleans, LA 70112, USA Volume 4 : Issue 1 Article Ref. #: 1000HROJ4136 INTRODUCTION Article History Inotropic support is contemplated in the presence of ongoing end-organ hypoperfusion or Received: January 3rd, 2017 refractory symptoms in decompensated heart failure (DHF). However, inotropic agents may Accepted: January 24th, 2017 cause tachycardia leading to increased myocardial oxygen demand and arrhythmogenesis.1 Published: January 24th, 2017 Introduction of beta blocker (BB) therapy in DHF patients requiring inotrope support is discouraged due to the negative hemodynamic impact of acute BB therapy.2-5 On the other hand, reduction in heart rate by BB therapy results in decreased myocardial oxygen demand Citation and increased ventricular diastolic filling.6,7 Additionally, early introduction of BB therapy Jaiswal A, Nguyen VQ, Carry B, Le improves outcome in heart failure.2-5,8 Jemtel TH. Combination therapy with beta blocker and inotrope in decom- pensated heart failure: A clinical ob- We describe our clinical experience in two DHF patients with end-organ hypoperfusion servation. -

Inotropes Are Linked to Increased Mortality in Heart Failure
The VAD Journal: The journal of mechanical assisted circulation and heart failure Review Inotropes are linked to Increased Mortality in Heart Failure M Chadi Alraies 1, Bill Tran 1 and Sirtaz Adatya 2* 1 Department of Medicine, Division of Cardiovascular Medicine, University of Minnesota, Minneapolis, Minnesota, USA 2 Department of Medicine, Division of Cardiovascular Medicine, University of Chicago, Chicago Illinois. * Corresponding author: [email protected] Keywords Citation: Alrais, M. et al. (2015). Inotropes are linked to Increased Inotropes; Heart failure; ventricular assist device Mortality. VAD Journal , 1. doi:: http://dx.doi.org/10.13023/VAD.2 015.08 Introduction Editor-in-Chief: Maya Guglin, University of Kentucky With the advancement of technology and availability of mechanical Received: June 17, 2015 circulatory support (MCS) devices for the treatment of acute decompensated systolic HF in the 21 st century, the role of inotropes is becoming obsolete. Accepted: June 25, 2015 Medical therapy for acute decompensated heart failure (HF) has not changed Published: June 29, 2015 , 2015 since 1960’s, we still use supplemental oxygen, diuretics, vasodilators and © 2015 The Author(s). This is an inotropes to improve congestion, cardiac output, end organ perfusion and 1 open access article published symptoms related to elevate filling pressures . Despite demonstrated under the terms of the Creative improvements in hemodynamics, the uses of inotropes have not demonstrated Commons Attribution- NonCommercial 4.0 International any improvements in mortality. Mechanical circulatory support (MCS) use is License growing rapidly in the USA, in patients with stage D HF both as destination (https://creativecommons.org/lice nses/by-nc/4.0/ ), which permits therapy and as a bridge to cardiac transplantation. -
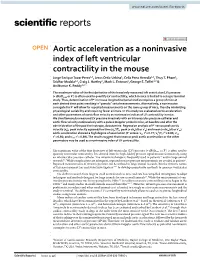
Aortic Acceleration As a Noninvasive Index of Left Ventricular Contractility in the Mouse
www.nature.com/scientificreports OPEN Aortic acceleration as a noninvasive index of left ventricular contractility in the mouse Jorge Enrique Tovar Perez1,3, Jesus Ortiz‑Urbina1, Celia Pena Heredia1,2, Thuy T. Pham1, Sridhar Madala1,4, Craig J. Hartley1, Mark L. Entman1, George E. Tafet1,2 & Anilkumar K. Reddy1,4* The maximum value of the frst derivative of the invasively measured left ventricular (LV) pressure (+ dP/dtmax or P′) is often used to quantify LV contractility, which in mice is limited to a single terminal study. Thus, determination of P′ in mouse longitudinal/serial studies requires a group of mice at each desired time point resulting in “pseudo” serial measurements. Alternatively, a noninvasive surrogate for P′ will allow for repeated measurements on the same group of mice, thereby minimizing physiological variability and requiring fewer animals. In this study we evaluated aortic acceleration and other parameters of aortic fow velocity as noninvasive indices of LV contractility in mice. We simultaneously measured LV pressure invasively with an intravascular pressure catheter and aortic fow velocity noninvasively with a pulsed Doppler probe in mice, at baseline and after the administration of the positive inotrope, dobutamine. Regression analysis of P′ versus peak aortic 2 velocity (vp), peak velocity squared/rise time (vp /T), peak (+ dvp/dt or v′p) and mean (+ dvm/dt or v′m) 2 2 2 aortic acceleration showed a high degree of association (P′ versus: vp, r = 0.77; vp /T, r = 0.86; v′p, 2 2 r = 0.80; and v′m, r = 0.89). The results suggest that mean or peak aortic acceleration or the other parameters may be used as a noninvasive index of LV contractility. -

Drugs in Cardiology
Drugs in Cardiology Fozia Ahmed Consultant Cardiologist Manchester Heart Centre What do you need to know about pharmacology for BHRS exam • Cardiac action potential • Vaughn William’s classification • Effects of drugs on pacing thresholds and DFTs • Indications for different drugs • Side effects of drugs – QT interval – Toxicity – contraindications • Drugs for heart failure Phase 4 (Cardiomyocyte AP) • Phase 4= Resting membrane potential – Horizontal line (non-pacemaker cells) – -90mV • In phase 4 membrane most permeable to K+ ions – Fast Na+ channels and slow Ca 2+ channels are closed • Stable vs. unstable phase 4 Phase 0 (depolarisation) • Phase 0=rapid depolarisation – Electrical stimulation of cell by adjacent cell undergoing depolarisation – The K+ channels are closed during phase 0 – Opening of Fast Na+ channels – Influx of Na+ – Increase in membrane potential • Potential inside the cell rises to +10mV Phase 1 (initial repolarisation) • Phase 1 represents initial repolarisation • Closure of fast Na+ channels • Net outflow of K+ – caused by opening of transient + outward K channel (Kto) – hyperpolarising outward K+ current(iKto) Phase 2 (plateau phase) • Phase 2 represents the “plateau phase” • Sustained by: – Inward movement of calcium through Slow (L-type) calcium channels – Slow outward movement of K+ thru the slow delayed rectifier K+ channel • Phase 2 differentiates cardiomyocyte action potentials from those of pacemaker cells, skeletal muscle and nerves Phase 3 (rapid repolarisation phase) • During phase 3, L-type Ca2+ channels -

Inotrope Use in Critically Ill Patients: Prevalence and Effects on Mortality Prasad Sonawane*, Biswajit L Jagtap**, Suprakash Chaudhury***
Pravara Medical Review, December 2016, 8(4) 4-11 [ISSN P : 0975- 0533 , ISSN E : 0976- 0164 ] Original article: Inotrope use in critically ill patients: Prevalence and effects on mortality Prasad Sonawane*, Biswajit L Jagtap**, Suprakash Chaudhury*** *Consultant Physician &specialist in Critical Care Medicine, Mumbai ** Asst. Professor *** Professor & Head, Dept of Psychiatry, RMC, PIMS (DU), Loni Corresponding author: Dr. Biswajit L Jagtap, Asst Professor, Dept of Psychiatry, RMC, PIMS (DU), Loni Abstract: Clinical Profile of critically ill patients needing inotropes in medical intensive care unit (MICU) of a tertiary care centre revealed that out of 399 patients admitted during study period, 54 (13.53%) needed inotropes. These 54 patients were suffering from septic shock (n=29), CVT/ GBS/ Infective meningitis (n=8), Acute febrile illness(n=6), fulminant hepatic failure(n=4), malaria(n=4), pulmonary thromboembolism(n=2), and dengue(n=1). The inotropes used included noradrenaline in 45 (83.33%), dopamine in 42 (77.78%) and dobutamine in 5 (9.26%) patients. Of critically ill patients requiring inotropes, 8 (12.96%) needed inotropes for 24 hours, 21(38.89%) needed inotropes for 48 hours and 25(46.30%) needed inotropes for>48 hours duration. There was no association amongst different type of inotropes used and outcome of patients.(p=0.336) Out of 54 needing inotropes, 11( 20.37%) survived and 43 (79.62%) expired while out of 345 patients not needing inotropes, 221 (64.05%) survived and 124 (35.94%) expired. Need of inotropes was associated with significantly increased risk of death. Key Words : inotropes; intensive care unit; adverse effects; mortality INTRODUCTION Sepsis is often a contributory factor for Inotropic drugs enhance myocardial mortality in critically ill patients. -
INDE 221 Spring 2010 Syllabus Part 2
Human Health & Disease Mondays, Tuesdays, Thursdays and Fridays 9:00 - 11:50 AM Lectures: Room M-112, Labs: Fleischmann IINNDDEE 222211 SSpprriinngg 22001100 Syllabus SSyyllllaabbuuss PPaarrtt 22 (2010) Year's Last Syllabus (2010) Year's Last Human Health & Disease Inde 221 Spring 2010 Table of Contents CARDIOVASCULAR BLOCK SYLLABUS SCHEDULE 7 SYLLABUS PREFACE 11 CARDIAC MUSCLE AND FHC 15 EXCITATION-CONTRACTION COUPLING Syllabus27 NERNST POTENTIAL AND OSMOSIS 43 EXCITABILITY AND CONDUCTION 51 CIRCULATORY VESSEL HISTOLOGY LAB 63 CARDIAC ACTION POTENTIAL 71 CONTROL OF HEART RHYTHM (2010) 85 AUTONOMIC DRUGS OVERVIEW I 97 ELECTROCARDIOGRAM (ECG) 99 LESIONS OF BLOOD VESSELS 109 THROMBOEMBOLIC DISEASE 117 CARDIAC REFLEXESYear's 123 AUTONOMIC DRUGS OVERVIEW II 141 ECG SMALL GROUPS 143 LastAUTONOMIC DRUGS: CHOLINERGICS 147 CARDIAC MUSCLE MECHANICS 149 AUTONOMIC DRUGS: ANTICHOLINERGICS 175 ARRHYTHMIAS 177 AUTONOMIC DRUGS: SYMPATHOMIMETICS I 203 VENTRICULAR PHYSIOLOGY 205 AUTONOMIC DRUGS: SYMPATHOMIMETICS II 235 STARLING CURVE AND VENOUS RETURN 237 CARDIAC OUTPUT AND CATHETERIZATION 245 AUTONOMIC DRUGS: ADRENOCEPTOR BLOCKERS 267 PHYSICS OF CIRCULATION Syllabus269 CASE DISCUSSIONS: AUTONOMIC DRUGS 289 SMOOTH MUSCLE 291 ISCHEMIC AND VALVULAR HEART DISEASE 303 RENAL CIRCULATION (2010) 323 HYPERTENSION 333 CARDIOMYOPATHY, MYOCARDITIS AND ATRIAL MYXOMA 351 ENDOTHELIUM AND CORONARY CIRCULATION 369 ANGINA PECTORIS 389 DRUGS USEDYear's IN HYPERTENSION 397 SHOCK 399 ADULT CARDIAC LAB 413 CARDIAC ANESTHESIA & BYPASS 421 LastEXERCISE PHYSIOLOGY 431 ISCHEMIC -

ICTSCD Chapter 3
CHAPTER 3 - HEART FAILURE INTRODUCTORY COMMENT The primary aim of this chapter is to discuss the pathophysiology of cardiac failure. I do this in the hope of giving a simple view of it, to facilitate understanding of why different signs and symptoms occur, and so be in a position to best use clinical information in building up clinical diagnoses and treating individual patients. Some normal values Cardiac output - normally approx. 5 l/min. Stroke volume (SV) - approx. 70 ml. Heart rate - approx. 70 beats per minute End Diastolic Volume (EDV) - approx. 120 ml. Systolic ejection fraction = SV/EDV = approx. 67%. Mean JVP - 0-2 cms. above manubriosternal angle. End diastolic pressure - up to 10 mmHg before "a" wave. No more than 15 mmHg at "a" wave peak Know your "pressure volume loops", and the Frank-Starling curves. DEFINITION This is not as easy as it sounds. An elevated venous pressure may reflect right heart failure, but it may also reflect overfilling of the circulation as in over-transfusion, or in sodium and water retention from renal impairment. Therefore, the most generally accepted definition of heart failure is that state when the volume output of the heart fails to keep pace with the metabolic demands of the tissues. By this, heart failure may occur in absolute terms when the pump itself fails, or when there is a higher demand than it can meet, as in severe thyrotoxicosis. TYPES OF CARDIAC FAILURE The above definition gives us our first subdivision of heart failure into high output and low output types. The former are relatively rare, but include such conditions as thyrotoxicosis, high fever, beri- beri heart disease (Vitamin B1 deficiency), anaemia, pregnancy, arterio-venous fistulae and intra- cardiac left to right shunts, Paget's disease of bone, prolonged severe tachycardia of any cause (e.g.