Pictorial Essay
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diapositiva 1
Thoracic Cage and Thoracic Inlet Professor Dr. Mario Edgar Fernández. Parts of the body The Thorax Is the part of the trunk betwen the neck and abdomen. Commonly the term chest is used as a synonym for thorax, but it is incorrect. Consisting of the thoracic cavity, its contents, and the wall that surrounds it. The thoracic cavity is divided into 3 compartments: The central mediastinus. And the right and left pulmonary cavities. Thoracic Cage The thoracic skeleton forms the osteocartilaginous thoracic cage. Anterior view. Thoracic Cage Posterior view. Summary: 1. Bones of thoracic cage: (thoracic vertebrae, ribs, and sternum). 2. Joints of thoracic cage: (intervertebral joints, costovertebral joints, and sternocostal joints) 3. Movements of thoracic wall. 4. Thoracic cage. Thoracic apertures: (superior thoracic aperture or thoracic inlet, and inferior thoracic aperture). Goals of the classes Identify and describe the bones of the thoracic cage. Identify and describe the joints of thoracic cage. Describe de thoracic cage. Describe the thoracic inlet and identify the structures passing through. Vertebral Column or Spine 7 cervical. 12 thoracic. 5 lumbar. 5 sacral 3-4 coccygeal Vertebrae That bones are irregular, 33 in number, and received the names acording to the position which they occupy. The vertebrae in the upper 3 regions of spine are separate throughout the whole of life, but in sacral anda coccygeal regions are in the adult firmly united in 2 differents bones: sacrum and coccyx. Thoracic vertebrae Each vertebrae consist of 2 essential parts: An anterior solid segment: vertebral body. The arch is posterior an formed of 2 pedicles, 2 laminae supporting 7 processes, and surrounding a vertebral foramen. -

Unit 2 Lab 2
Unit 2, Lab 1 PTA/OTA 106 Regional A & P G. Blevins Updated: Fall 2011 SURFACE ANATOMY: VERTEBRAL COLUMN BONES [26] Jugular or suprasternal notch Vertebra (general features) Sternal angle Body Manubrium Neural arch Body of the sternum Pedicles Xiphisternal joint Laminae Costal margin Spinal (or vertebral) foramen Costal arch Transverse processes Anterior median line Spinous process Midclavicular lines Superior articulating processes Intermammary cleft Inferior articulating processes Axillary fossa Intervertebral foramen Anterior axillary line Intervertebral disc Anterior axillary fold Midaxillary line Thoracic vertebrae [12] Posterior axillary line Rib facets or demifacets Posterior median line Scapular lines Lumbar vertebrae [5] Epigastric fossa Lack rib facets and transverse Iliac crest foramina Umbilicus Linea alba Sacrum [1] Rectus abdominis Fused bone consisting of 5 Serratus anterior vertebrae Semilunar line Sacral promontory Sacral foramina (pelvic & dorsal) VERTEBRAL COLUMN- Auricular surface Special Features Coccyx [1] Normal Curves Fused bone consisting of 3-5 Primary: vertebrae Thoracic Sacral THORACIC BONES [25] Secondary: Sternum [1] Cervical Manubrium Lumbar Body (or gladiolus) Abnormal Curves Jugular (or suprasternal) notch Kyphosis Xiphoid process Lordosis Ribs [12 pair] Scoliosis Head Neck Tubercle Body (or shaft) Costal groove Costal cartilages Types of ribs True ribs False ribs Floating ribs PECTORAL (OR SHOULDER) GIRDLE Clavicles [2] Sternal extremity Acromial extremity Conoid tubercle Scapula [2] Borders: Superior -

Epithelia Joitns
NAME LOCATION STRUCTURE FUNCTION MOVEMENT Temporomandibular joint Condylar head of ramus of Synovial Diarthrosis Modified hinge joint mandible and glenoid fossa of Rotation and gliding temporal bone Biaxial Zygapophyseal joint Between articular processes of Synovial Diarthrosis Gliding 2 adjacent vertebrae Non axial Atlanto-Occipital joints Atlas and occipital condyle of Synovial Diarthrosis Ellipsoid occipital bone Biaxial Atlantoaxial joints Atlas and axis Synovial Diarthrosis Pivot Uniaxial Joints of vertebral arches Ligaments Fibrous Amphiarthrosis Syndesmoses Intervertebral symphyseal Intervertebral disk between 2 Cartilaginous Amphiarthrosis joints vertebrae Symphysis Costovertebral Head of ribs and body of Synovial Diarthrosis Gliding thoracic vertebra Non axial Costotrasnverse joints Tubercle of rib and transverse Synovial Diarthrosis Gliding process of thoracic vertebra Non axial Lumbosacral Joint Left and right zygopophyseal Laterally Synovial joint Intervertebral symphyseal joint Symphysis SternoclavicularJoint Clavicular notch articulates Synovial Diarthrosis Gliding with medial ends of clavicle Non Axial Manubriosternal Joint Hyaline cartilage junction Cartilaginous Synarthrosis Sternal Angle between manubrium and body Symphysis Xiphisternal Joint Cartilage between xiphoid Synchondrosis Synarthrosis process and body Synostoses Sternocostal Joint (1st) Costocartilage 1 with sternum Cartilaginous Synchondrosis Synarthrosis NAME Location Section Anterior longitudinal runs down anterior surface of vertebral body Vertebral column ligament Posterior longitudinal in canal, runs down posterior surface of vertebral body ligament Interspinous ligament Connects spinous processes Ligamentum flavum Connects laminae ! Intra-articular Disc Between articulating surface of sternum and clavicle Sternoclavicular Joint Costoclavicular ligament 1st rib to clavicle !. -

1 the Thoracic Wall I
AAA_C01 12/13/05 10:29 Page 8 1 The thoracic wall I Thoracic outlet (inlet) First rib Clavicle Suprasternal notch Manubrium 5 Third rib 1 2 Body of sternum Intercostal 4 space Xiphisternum Scalenus anterior Brachial Cervical Costal cartilage plexus rib Costal margin 3 Subclavian 1 Costochondral joint Floating ribs artery 2 Sternocostal joint Fig.1.3 3 Interchondral joint Bilateral cervical ribs. 4 Xiphisternal joint 5 Manubriosternal joint On the right side the brachial plexus (angle of Louis) is shown arching over the rib and stretching its lowest trunk Fig.1.1 The thoracic cage. The outlet (inlet) of the thorax is outlined Transverse process with facet for rib tubercle Demifacet for head of rib Head Neck Costovertebral T5 joint T6 Facet for Tubercle vertebral body Costotransverse joint Sternocostal joint Shaft 6th Angle rib Costochondral Subcostal groove joint Fig.1.2 Fig.1.4 A typical rib Joints of the thoracic cage 8 The thorax The thoracic wall I AAA_C01 12/13/05 10:29 Page 9 The thoracic cage Costal cartilages The thoracic cage is formed by the sternum and costal cartilages These are bars of hyaline cartilage which connect the upper in front, the vertebral column behind and the ribs and intercostal seven ribs directly to the sternum and the 8th, 9th and 10th ribs spaces laterally. to the cartilage immediately above. It is separated from the abdominal cavity by the diaphragm and communicates superiorly with the root of the neck through Joints of the thoracic cage (Figs 1.1 and 1.4) the thoracic inlet (Fig. -

Displacement of the Temporomandibular Joint Disk: Correlation Between Clinical Findings and MRI Characteristics
Applied RESEA R CH Displacement of the Temporomandibular Joint Disk: Correlation Between Clinical Findings and MRI Characteristics Contact Author Zeev V. Maizlin, MD; Nicoleta Nutiu, MD; Peter B. Dent, MD; Patrick M. Vos, MD; Dr. Maizlin David M. Fenton, MD; John M. Kirby, MBBCh; Parag Vora, MBBS; Email: [email protected] Jean H. Gillies, MD; Jason J. Clement, MD ABSTRACT Background and Objective: Disk displacement frequently causes dysfunction of the temporomandibular joint (TMJ). Magnetic resonance imaging (MRI) of the TMJ is 95% accurate in the assessment of disk position and form. Various restorative procedures are used for treatment of disk displacement. However, several authors have noted a lack of correlation between MRI findings of disk displacement and the extent of pain and dysfunction of the TMJ. The purpose of this study was to evaluate whether MRI findings of various degrees of disk displacement could be correlated with the presence of clinical signs and symptoms in patients with a clinical disorder of the TMJ. Materials and Methods: One hundred and forty-four TMJs (in 72 patients) were imaged. Displacement of the posterior band in relation to the condyle was quantified as mild or significant. Results: Disk displacement was found in 45 (54%) of the 84 symptomatic joints and 13 (22%) of the 60 asymptomatic joints. Among the 84 symptomatic joints, 31 (37%) had disk displacement with reduction and 14 (17%) had disk displacement without reduction. In the latter group, 11 (79%) of the 14 joints had significant displacement of the posterior band (8 or 9 o’clock) and 21% had mild displacement of the posterior band (10 o’clock). -

Dynamic Musculoskeletal Biomechanics in the Human Jaw
DYNAMIC MUSCULOSKELETAL BIOMECHANICS IN THE HUMAN JAW by CHRISTOPHER CHARLES PECK BDS, The University of Sydney, 1988 MSc(Dent), The University of Sydney, 1995 A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY in THE FACULTY OF GRADUATE STUDIES (Department of Oral Biology) We accept this thesis as confonning to the required standard 'THE UNIVERSITY OF BRITISH COLUMBIA NOVEMBER 1999 ® Christopher Charles Peck, 1999 In presenting this thesis in partial fulfilment of the requirements for an advanced degree at the University of British Columbia, I agree that the Library shall make it freely available for reference and study. I further agree that permission for extensive copying of this thesis for scholarly purposes may be granted by the head of my department or by his or her representatives. It is understood that copying or publication of this thesis for financial gain shall not be allowed without my written permission. Department of Q/-«J "fct'ftlo^ ( 0>oJ W^oJfL £cwu,o The University of British Columbia Vancouver, Canada Date 2°V .NW*—\ \^ DE-6 (2/88) ABSTRACT The high prevalence of functional disorders in the human jaw emphasises the need to understand better its dynamic behaviour. In the present studies, dynamic mathematical models based on typical physical properties of the human jaw and skeletal muscles have been developed. In the first three studies, a model of the entire jaw was created and utilised to predict jaw elasticity and viscosity, and to simulate muscle-driven symmetrical and asvmmetrical jaw movements. Specifically these models were constructed without "ligaments" (temporomandibular capsule or other accessory jaw ligaments) to determine whether or not plausible motion could be simulated in their absence. -

Dynamic Weight-Bearing Magnetic Resonance in the Clinical Diagnosis of Internal Temporomandibular Joint Disorders
634 Review Article Dynamic Weight-bearing Magnetic Resonance in the Clinical Diagnosis of Internal Temporomandibular Joint Disorders Silvana Giannini, MD1 Giorgio Chiogna, MD2 Rosario Francesco Balzano, MD3 Giuseppe Guglielmi, MD3 1 Department of Radiology, Casa di Cura Villa Stuart Sports Clinic, Address for correspondence Silvana Giannini, MD, Department of Università degli Studi di Roma “Foro Italico,” Rome, Italy Radiology, Casa di Cura Villa Stuart Sports Clinic, 00135 Rome, Italy 2 Department of Surgical and Dental Sciences, Fondazione Don Carlo (e-mail: [email protected]). Gnocchi, Rome, Italy 3 Department of Clinical and Experimental Medicine, University School of Medicine, Foggia, Italy Semin Musculoskelet Radiol 2019;23:634–642. Abstract Temporomandibular joint (TMJ) disorders can be painful and cause functional limi- tations and bone changes. Deeper clinical knowledge of the pathologies related to the TMJ has always been hindered by the difficult identification of the causes that limit its movement. Weight-bearing magnetic resonance imaging (WBMRI) can reproduce the articular movement in orthostasis and allows the evaluation of joint movement. Keywords WBMRI, compared with other procedures such as double-type condylography and ► temporomandibular real-time dynamic ultrasound, helps to better identify tissue characteristics of the joint articular glenoid-condylar surfaces, articular space, disk position on both the open and ► weight-bearing MRI closed mouth, and the locoregional musculotendinous area. WBMRI also identifies -

The Distal Radioulnar Joint
90 Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):90-6 The Distal Radioulnar Joint Peter C. Tsai, M.D., and Nader Paksima, D.O., M.P.H. Abstract gular fibrocartilage (TFC), the volar and dorsal radioulnar The distal radioulnar joint (DRUJ) acts in concert with the ligaments, the capsule, and the ulnar collateral ligament. proximal radioulnar joint to control forearm rotation. The DRUJ Extrinsic stability is achieved through static and dynamic is stabilized by the triangular fibrocartilage complex (TFCC). forces. The extensor carpi ulnaris (ECU) subsheath and the This complex of fibrocartilage and ligaments support the joint interosseous membrane (IOM) are assisted by the pronator through its arc of rotation, as well as provide a smooth surface quadratus, which actively compresses the ulnar head into for the ulnar side of the carpus. TFCC and DRUJ injuries are the sigmoid notch, and by the flexors and extensors of the part of the common pattern of injuries we see with distal radius forearm, which dynamically compress the DRUJ. fractures. While much attention has been paid to the treatment The bony and ligamentous restraints of the DRUJ en- of the distal radius fractures, many of the poor outcomes are able controlled pronation and supination.1 Though slightly due to untreated or unrecognized injuries to the DRUJ and its asymmetric to the ulnar head, the sigmoid notch has been components. shown to contribute approximately 20% of the stability of the DRUJ.2,3 The larger radius of curvature of the sigmoid he distal radioulnar joint (DRUJ) has been extensively notch results in a shallow concavity in comparison to the studied; however, much debate remains concern- convex ulnar head. -

Muscles Involved in Respiration
Prof. Ahmed Fathalla Ibrahim Professor of Anatomy College of Medicine King Saud University E-mail: [email protected] OBJECTIVES At the end of the lecture, students should: ▪ Describe the components of the thoracic cage and their articulations. ▪ Describe in brief the respiratory movements. ▪ List the muscles involved in inspiration and in expiration. ▪ Describe the attachments of each muscle to the thoracic cage and its nerve supply. ▪ Describe the origin, insertion, nerve supply of diaphragm. THORACIC CAGE Vertebra Rib THORACIC CAGE ❑Conical in shape ❑Has 2 apertures (openings): 1. Superior (thoracic outlet): narrow, open, continuous with neck 2. Inferior: wide, closed by diaphragm ❑ Formed of: 1. Sternum & costal cartilages: anteriorly 2. Twelve pairs of ribs: laterally 3. Twelve thoracic vertebrae: posteriorly ARTICULATIONS Costovertebral Manubriosternal Intervertebral disc Costochondral Sternocostal Xiphisternal ARTICULATIONS Costovertebral Sternocostal Costochondral Interchondral ARTICULATIONS • Secondary cartilaginous: Manubriosternal joint, Xiphisternal joint and Intervertebral discs. • Primary cartilaginous: 1st Sternocostal joint, Costochondral joints and Interchondral joints. • Plane synovial joints: Costovertebral joints and the rest of Sternocostal joints. RESPIRATORY MOVEMENTS A- MOVEMENTS OF DIAPHRAGM Inspiration Contraction (descent) of diaphragm Increase of vertical diameter of thoracic cavity Relaxation (ascent) of diaphragm) Expiration RESPIRATORY MOVEMENTS B- MOVEMENTS OF RIBS PUMP HANDLE MOVEMENT BUCKET HANDLE -

Temporomandibular Joint Pain and Dysfunction
Temporomandibular Joint Pain and Dysfunction Kathleen Herb, DMD, MD, Sung Cho, DMD, and Marlind Alan Stiles, DMD Corresponding author Marlind Alan Stiles, DMD open arthroplasty and toward arthroscopic procedures. Department of Oral and Maxillofacial Surgery, Thomas Jefferson Research continues to look toward biochemical markers University Hospital, 909 Walnut Street, Suite 300, Philadelphia, of disease. The interrelationship between the various dis- PA 19107, USA. orders continues to be explored. E-mail: [email protected] The temporomandibular joint (TMJ) is a compound Current Pain and Headache Reports 2006, 10:408–414 articulation formed from the articular surfaces of the Current Science Inc. ISSN 1531-3433 temporal bone and the mandibular condyle. Both sur- Copyright © 2006 by Current Science Inc. faces are covered by dense articular fibrocartilage. Each condyle articulates with a large surface area of temporal bone consisting of the articular fossa, articular eminence, Pain caused by temporomandibular disorders originates and preglenoid plane. The TMJ functions uniquely in that from either muscular or articular conditions, or both. the condyle both rotates within the fossa and translates Distinguishing the precise source of the pain is a sig- anteriorly along the articular eminence. Because of the nificant diagnostic challenge to clinicians, and effective condyle’s ability to translate, the mandible can have a management hinges on establishing a correct diagnosis. much higher maximal incisal opening than would be pos- This paper examines terminology and regional anatomy sible with rotation alone. The joint is thus referred to as as it pertains to functional and dysfunctional states of “gynglimodiarthrodial”: a combination of the terms gin- the temporomandibular joint and muscles of mastica- glymoid (rotation) and arthroidial (translation) [1]. -
Intervertebral Foramina - Wikipedia Visited on 06/06/2017
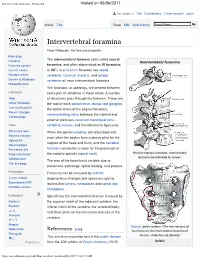
Intervertebral foramina - Wikipedia Visited on 06/06/2017 Not logged in Talk Contributions Create account Log in Article Talk Read Edit View history Intervertebral foramina From Wikipedia, the free encyclopedia Main page The intervertebral foramen (also called neural Contents Intervertebral foramina Featured content foramina, and often abbreviated as IV foramina Current events or IVF), is a foramen between two spinal Random article vertebrae. Cervical, thoracic, and lumbar Donate to Wikipedia vertebrae all have intervertebral foramina. Wikipedia store The foramina, or openings, are present between Interaction every pair of vertebrae in these areas. A number Help of structures pass through the foramen. These are About Wikipedia the root of each spinal nerve, dorsal root ganglion, Community portal the spinal artery of the segmental artery, Recent changes communicating veins between the internal and Contact page external plexuses, recurrent meningeal (sinu- Tools vertebral) nerves, and transforaminal ligaments. What links here When the spinal vertebrae are articulated with Related changes each other the bodies form a strong pillar for the Upload file support of the head and trunk, and the vertebral Special pages Permanent link foramen constitutes a canal for the protection of Page information the medulla spinalis (spinal cord). Peculiar thoracic vertebrae. Intervertebral foramina are indicated by arrows. Wikidata item The size of the foramina is variable due to Cite this page placement, pathology, spinal loading, and posture. Print/export Foramina can be occluded by arthritic Create a book degenerative changes and space-occupying Download as PDF lesions like tumors, metastases and spinal disc Printable version herniations. Languages Specifically the intervertebral foramen is bound by Deutsch the superior notch of the adjacent vertebra, the Español inferior notch of the vertebra, the vertebral body, and facet joints on the transverse process of the فارسی Français vertebra. -

A Functional Analysis of the Temporomandibular Joint in Homosapiens Sapiens and Homo Sapiens Neanderthalensis
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Masters Theses Graduate School 6-1978 A Functional Analysis of the Temporomandibular Joint in Homosapiens sapiens and Homo sapiens neanderthalensis Janice Lynn Foxworthy University of Tennessee, Knoxville Follow this and additional works at: https://trace.tennessee.edu/utk_gradthes Part of the Anthropology Commons Recommended Citation Foxworthy, Janice Lynn, "A Functional Analysis of the Temporomandibular Joint in Homosapiens sapiens and Homo sapiens neanderthalensis. " Master's Thesis, University of Tennessee, 1978. https://trace.tennessee.edu/utk_gradthes/4249 This Thesis is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Masters Theses by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a thesis written by Janice Lynn Foxworthy entitled "A Functional Analysis of the Temporomandibular Joint in Homosapiens sapiens and Homo sapiens neanderthalensis." I have examined the final electronic copy of this thesis for form and content and recommend that it be accepted in partial fulfillment of the equirr ements for the degree of Master of Arts, with a major in Anthropology. Fred H. Smith, Major Professor We have read this thesis and recommend its acceptance: Richard L. Jantz, William M. Bass Accepted for the Council: Carolyn R. Hodges Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) To the Graduate CoWlcil: I am submitting herewith a thesis written by Janice Lynn Foxworthy entitled "A Functional Analysis of the Tempo�omandibular Joint in Homo sapiens sapiens and Homo sapiens neanderthalensis." I recommend that it be accepted in partial fulfillment of the requirements for the degree of Master of Arts, with a major in Anthropology.