Medicinal Use of Testosterone and Related Steroids Revisited
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WADA Technical Letter – TL07 ANDARINE
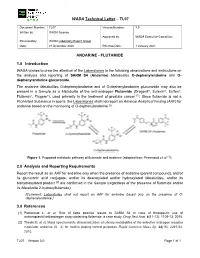
WADA Technical Letter – TL07 Document Number: TL07 Version Number: 3.0 Written by: WADA Science Approved by: WADA Executive Committee Reviewed by: WADA Laboratory Expert Group Date: 21 December 2020 Effective Date: 1 January 2021 ANDARINE - FLUTAMIDE 1.0 Introduction WADA wishes to draw the attention of the Laboratories to the following observations and instructions on the analysis and reporting of SARM S4 (Andarine) Metabolites O-dephenylandarine and O- dephenylandarine glucuronide. The andarine Metabolites O-dephenylandarine and of O-dephenylandarine glucuronide may also be present in a Sample as a Metabolite of the anti-androgen Flutamide (Drogenil®, Eulexin®, Euflex®, Flutamin®, Flugere®), used primarily in the treatment of prostate cancer [1]. Since flutamide is not a Prohibited Substance in sports, the Laboratories shall not report an Adverse Analytical Finding (AAF) for andarine based on the monitoring of O-dephenylandarine [2]. Figure 1. Proposed metabolic pathway of flutamide and andarine (adapted from Perrenoud et al. [1]). 2.0 Analysis and Reporting Requirements Report the result as an AAF for andarine only when the presence of andarine (parent compound), and/or its glucuronic acid conjugate, and/or its deacetylated and/or hydroxylated Metabolites, and/or its bishydroxylated product [2] are confirmed in the Sample (regardless of the presence of flutamide and/or its Metabolite 2-hydroxyflutamide); [Comment: Laboratories shall not report an AAF for andarine based only on the presence of O- dephenylandarine.] 3.0 References [1] Perrenoud L. et al. Risk of false positive results to SARM S4 in case of therapeutic use of antineoplastic/antiandrogen drug containing flutamide: a case study. -

DHEA | Medchemexpress
Inhibitors Product Data Sheet DHEA • Agonists Cat. No.: HY-14650 CAS No.: 53-43-0 Molecular Formula: C₁₉H₂₈O₂ • Molecular Weight: 288.42 Screening Libraries Target: Androgen Receptor; Endogenous Metabolite Pathway: Others; Metabolic Enzyme/Protease Storage: Please store the product under the recommended conditions in the Certificate of Analysis. SOLVENT & SOLUBILITY In Vitro DMSO : 50 mg/mL (173.36 mM; Need ultrasonic) Ethanol : 50 mg/mL (173.36 mM; Need ultrasonic) H2O : 1 mg/mL (3.47 mM; Need ultrasonic) Mass Solvent 1 mg 5 mg 10 mg Concentration Preparing 1 mM 3.4672 mL 17.3358 mL 34.6717 mL Stock Solutions 5 mM 0.6934 mL 3.4672 mL 6.9343 mL 10 mM 0.3467 mL 1.7336 mL 3.4672 mL Please refer to the solubility information to select the appropriate solvent. In Vivo 1. Add each solvent one by one: Cremophor EL Solubility: 14.29 mg/mL (49.55 mM); Clear solution; Need ultrasonic 2. Add each solvent one by one: 10% DMSO >> 40% PEG300 >> 5% Tween-80 >> 45% saline Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 3. Add each solvent one by one: 10% DMSO >> 90% (20% SBE-β-CD in saline) Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 4. Add each solvent one by one: 10% DMSO >> 90% corn oil Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 5. Add each solvent one by one: 10% EtOH >> 90% (20% SBE-β-CD in saline) Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 6. -
(12) United States Patent (10) Patent No.: US 7,871,995 B2 Bunschoten Et Al
US00787 1995 B2 (12) United States Patent (10) Patent No.: US 7,871,995 B2 Bunschoten et al. (45) Date of Patent: *Jan. 18, 2011 (54) DRUG DELIVERY SYSTEM COMPRISINGA (52) U.S. Cl. ....................................... 514/171; 514/182 TETRAHYDROXYLATED ESTROGEN FOR (58) Field of Classification Search ................. 514/171, USE IN HORMONAL CONTRACEPTION 514f182 See application file for complete search history. (75) Inventors: Evert Johannes Bunschoten, Heesch (NL); Herman Jan Tijmen Coelingh (56) References Cited Bennink, Driebergen (NL); Christian U.S. PATENT DOCUMENTS Franz Holinka, New York, NY (US) 3,440,320 A 4, 1969 Sackler et al. O O 3,797.494. A 3, 1974 Zaffaroni (73) Assignee: Pantarhei Bioscience B.V., Al Zeist 4,460.372 A 7/1984 Campbell et al. (NL) 4,573.996 A 3/1986 Kwiatek et al. 4,624,665 A 1 1/1986 Nuwayser (*) Notice: Subject to any disclaimer, the term of this 4,722,941 A 2f1988 Eckert et al. patent is extended or adjusted under 35 4,762,717 A 8/1988 Crowley, Jr. U.S.C. 154(b) by 1233 days. 4.937,238 A 6, 1990 Lemon 5,063,507 A 1 1/1991 Lindsey et al. This patent is Subject to a terminal dis- 5,130,137 A 7/1992 Crowley, Jr. claimer. 5,211,952 A 5/1993 Spicer et al. 5,223,261 A 6/1993 Nelson et al. 5,340,584 A 8/1994 Spicer et al. (21) Appl. No.: 10/478,357 5,340,585 A 8/1994 Pike et al. 1-1. 5,340,586 A 8, 1994 Pike et al. -

The Effects of Androgens and Antiandrogens on Hormone Responsive Human Breast Cancer in Long-Term Tissue Culture1
[CANCER RESEARCH 36, 4610-4618, December 1976] The Effects of Androgens and Antiandrogens on Hormone responsive Human Breast Cancer in Long-Term Tissue Culture1 Marc Lippman, Gail Bolan, and Karen Huff MedicineBranch,NationalCancerInstitute,Bethesda,Maryland20014 SUMMARY Information characterizing the interaction between an drogens and breast cancer would be desirable for several We have examined five human breast cancer call lines in reasons. First, androgens can affect the growth of breast conhinuous tissue culture for andmogan responsiveness. cancer in animals. Pharmacological administration of an One of these cell lines shows a 2- ho 4-fold stimulation of drogens to rats bearing dimathylbenzanthracene-induced thymidina incorporation into DNA, apparent as early as 10 mammary carcinomas is associated wihh objective humor hr following androgen addition to cells incubated in serum regression (h9, 22). Shionogi h15 cells, from a mouse mam free medium. This stimulation is accompanied by an ac many cancer in conhinuous hissue culture, have bean shown celemation in cell replication. Antiandrogens [cyproterona to be shimulatedby physiological concentrations of andro acetate (6-chloro-17a-acelata-1,2a-methylena-4,6-pregna gen (21), thus suggesting that some breast cancer might be diene-3,20-dione) and R2956 (17f3-hydroxy-2,2,1 7a-tnima androgen responsive in addition to being estrogen respon thoxyastra-4,9,1 1-Inane-i -one)] inhibit both protein and siva. DNA synthesis below control levels and block androgen Evidence also indicates that tumor growth in humans may mediahed stimulation. Prolonged incubahion (greahenhhan be significantly altered by androgens. About 20% of pahianhs 72 hn) in antiandrogen is lethal. -

CASODEX (Bicalutamide)
HIGHLIGHTS OF PRESCRIBING INFORMATION • Gynecomastia and breast pain have been reported during treatment with These highlights do not include all the information needed to use CASODEX 150 mg when used as a single agent. (5.3) CASODEX® safely and effectively. See full prescribing information for • CASODEX is used in combination with an LHRH agonist. LHRH CASODEX. agonists have been shown to cause a reduction in glucose tolerance in CASODEX® (bicalutamide) tablet, for oral use males. Consideration should be given to monitoring blood glucose in Initial U.S. Approval: 1995 patients receiving CASODEX in combination with LHRH agonists. (5.4) -------------------------- RECENT MAJOR CHANGES -------------------------- • Monitoring Prostate Specific Antigen (PSA) is recommended. Evaluate Warnings and Precautions (5.2) 10/2017 for clinical progression if PSA increases. (5.5) --------------------------- INDICATIONS AND USAGE -------------------------- ------------------------------ ADVERSE REACTIONS ----------------------------- • CASODEX 50 mg is an androgen receptor inhibitor indicated for use in Adverse reactions that occurred in more than 10% of patients receiving combination therapy with a luteinizing hormone-releasing hormone CASODEX plus an LHRH-A were: hot flashes, pain (including general, back, (LHRH) analog for the treatment of Stage D2 metastatic carcinoma of pelvic and abdominal), asthenia, constipation, infection, nausea, peripheral the prostate. (1) edema, dyspnea, diarrhea, hematuria, nocturia, and anemia. (6.1) • CASODEX 150 mg daily is not approved for use alone or with other treatments. (1) To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca Pharmaceuticals LP at 1-800-236-9933 or FDA at 1-800-FDA-1088 or ---------------------- DOSAGE AND ADMINISTRATION ---------------------- www.fda.gov/medwatch The recommended dose for CASODEX therapy in combination with an LHRH analog is one 50 mg tablet once daily (morning or evening). -

Campro Catalog Stable Isotope
Introduction & Welcome Dear Valued Customer, We are pleased to present to you our Stable Isotopes Catalog which contains more than three thousand (3000) high quality labeled compounds. You will find new additions that are beneficial for your research. Campro Scientific is proud to work together with Isotec, Inc. for the distribution and marketing of their stable isotopes. We have been working with Isotec for more than twenty years and know that their products meet the highest standard. Campro Scientific was founded in 1981 and we provide services to some of the most prestigious universities, research institutes and laboratories throughout Europe. We are a research-oriented company specialized in supporting the requirements of the scientific community. We are the exclusive distributor of some of the world’s leading producers of research chemicals, radioisotopes, stable isotopes and environmental standards. We understand the requirements of our customers, and work every day to fulfill them. In working with us you are guaranteed to receive: - Excellent customer service - High quality products - Dependable service - Efficient distribution The highly educated staff at Campro’s headquarters and sales office is ready to assist you with your questions and product requirements. Feel free to call us at any time. Sincerely, Dr. Ahmad Rajabi General Manager 180/280 = unlabeled 185/285 = 15N labeled 181/281 = double labeled (13C+15N, 13C+D, 15N+18O etc.) 186/286 = 12C labeled 182/282 = d labeled 187/287 = 17O labeled 183/283 = 13C labeleld 188/288 = 18O labeled 184/284 = 16O labeled, 14N labeled 189/289 = Noble Gases Table of Contents Ordering Information.................................................................................................. page 4 - 5 Packaging Information .............................................................................................. -

Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals
Journal of Clinical Medicine Review Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals Carlotta Cocchetti 1, Jiska Ristori 1, Alessia Romani 1, Mario Maggi 2 and Alessandra Daphne Fisher 1,* 1 Andrology, Women’s Endocrinology and Gender Incongruence Unit, Florence University Hospital, 50139 Florence, Italy; [email protected] (C.C); jiska.ristori@unifi.it (J.R.); [email protected] (A.R.) 2 Department of Experimental, Clinical and Biomedical Sciences, Careggi University Hospital, 50139 Florence, Italy; [email protected]fi.it * Correspondence: fi[email protected] Received: 16 April 2020; Accepted: 18 May 2020; Published: 26 May 2020 Abstract: Introduction: To date no standardized hormonal treatment protocols for non-binary transgender individuals have been described in the literature and there is a lack of data regarding their efficacy and safety. Objectives: To suggest possible treatment strategies for non-binary transgender individuals with non-standardized requests and to emphasize the importance of a personalized clinical approach. Methods: A narrative review of pertinent literature on gender-affirming hormonal treatment in transgender persons was performed using PubMed. Results: New hormonal treatment regimens outside those reported in current guidelines should be considered for non-binary transgender individuals, in order to improve psychological well-being and quality of life. In the present review we suggested the use of hormonal and non-hormonal compounds, which—based on their mechanism of action—could be used in these cases depending on clients’ requests. Conclusion: Requests for an individualized hormonal treatment in non-binary transgender individuals represent a future challenge for professionals managing transgender health care. For each case, clinicians should balance the benefits and risks of a personalized non-standardized treatment, actively involving the person in decisions regarding hormonal treatment. -

Mifepristone
1. NAME OF THE MEDICINAL PRODUCT Mifegyne 200 mg tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains 200-mg mifepristone. For the full list of excipients, see section 6.1 3. PHARMACEUTICAL FORM Tablet. Light yellow, cylindrical, bi-convex tablets, with a diameter of 11 mm with “167 B” engraved on one side. 4. CLINICAL PARTICULARS For termination of pregnancy, the anti-progesterone mifepristone and the prostaglandin analogue can only be prescribed and administered in accordance with New Zealand’s abortion laws and regulations. 4.1 Therapeutic indications 1- Medical termination of developing intra-uterine pregnancy. In sequential use with a prostaglandin analogue, up to 63 days of amenorrhea (see section 4.2). 2- Softening and dilatation of the cervix uteri prior to surgical termination of pregnancy during the first trimester. 3- Preparation for the action of prostaglandin analogues in the termination of pregnancy for medical reasons (beyond the first trimester). 4- Labour induction in fetal death in utero. In patients where prostaglandin or oxytocin cannot be used. 4.2 Dose and Method of Administration Dose 1- Medical termination of developing intra-uterine pregnancy The method of administration will be as follows: • Up to 49 days of amenorrhea: 1 Mifepristone is taken as a single 600 mg (i.e. 3 tablets of 200 mg each) oral dose, followed 36 to 48 hours later, by the administration of the prostaglandin analogue: misoprostol 400 µg orally or per vaginum. • Between 50-63 days of amenorrhea Mifepristone is taken as a single 600 mg (i.e. 3 tablets of 200 mg each) oral dose, followed 36 to 48 hours later, by the administration of misoprostol. -

Safety Data Sheet
SAFETY DATA SHEET SECTION 1: PRODUCT IDENTIFICATION PRODUCT NAME DHEA (Prasterone) (Micronized) PRODUCT CODE 0733 SUPPLIER MEDISCA Inc. Tel.: 1.800.932.1039 | Fax.: 1.855.850.5855 661 Route 3, Unit C, Plattsburgh, NY, 12901 3955 W. Mesa Vista Ave., Unit A-10, Las Vegas, NV, 89118 6641 N. Belt Line Road, Suite 130, Irving, TX, 75063 MEDISCA Pharmaceutique Inc. Tel.: 1.800.665.6334 | Fax.: 514.338.1693 4509 Rue Dobrin, St. Laurent, QC, H4R 2L8 21300 Gordon Way, Unit 153/158, Richmond, BC V6W 1M2 MEDISCA Australia PTY LTD Tel.: 1.300.786.392 | Fax.: 61.2.9700.9047 Unit 7, Heritage Business Park 5-9 Ricketty Street, Mascot, NSW 2020 EMERGENCY PHONE CHEMTREC Day or Night Within USA and Canada: 1-800-424-9300 NSW Poisons Information Centre: 131 126 USES Adjuvant; Androgen SECTION 2: HAZARDS IDENTIFICATION GHS CLASSIFICATION Toxic to Reproduction (Category 2) PICTOGRAM SIGNAL WORD Warning HAZARD STATEMENT(S) Reproductive effector, prohormone. Suspected of damaging fertility or the unborn child. May cause harm to breast-fed children. Causes serious eye irritation. Causes skin and respiratory irritation. Very toxic to aquatic life with long lasting effects. AUSTRALIA-ONLY HAZARDS Not Applicable. PRECAUTIONARY STATEMENT(S) Prevention Wash thoroughly after handling. Obtain special instructions before use. Do not handle until all safety precautions have been read and understood. Do not breathe dusts or mists. Do not eat, drink or smoke when using this product. Avoid contact during pregnancy/while nursing. Wear protective gloves, protective clothing, eye protection, face protection. Avoid release to the environment. Response IF ON SKIN (HAIR): Wash with plenty of water. -

Human DHEA ELISA Kit (ARG80949)
Product datasheet [email protected] ARG80949 Package: 96 wells Human DHEA ELISA Kit Store at: 4°C Summary Product Description ARG80949 DHEA ELISA Kit is an Enzyme Immunoassay kit for the quantification of DHEA in human serum and plasma (EDTA). Tested Reactivity Hu Tested Application ELISA Target Name DHEA Sensitivity 0.07 ng/ml Sample Type Serum and plasma (EDTA). Standard Range 0.3 - 30 ng/ml Sample Volume 25 μl Application Instructions Assay Time 1 h (RT/shaker), 30 min (dark) Properties Form 96 well Storage instruction Store the kit at 2-8°C. Keep microplate wells sealed in a dry bag with desiccants. Do not expose test reagents to heat, sun or strong light during storage and usage. Please refer to the product user manual for detail temperatures of the components. Note For laboratory research only, not for drug, diagnostic or other use. Bioinformation Background Dehydroepiandrosterone (DHEA; androstenolone; 3b-hydroxy-5-androsten-17-one) is a C19 steroid produced in the adrenal cortex and, to a lesser extent, gonads. DHEA serves as a precursor in testosterone and estrogen synthesis. Due to the presence of a 17-oxo (rather than hydroxyl) group, DHEA has relatively weak androgenic activity, which has been estimated at ~10% that of testosterone. However in neonates, peripubertal children and in adult women, circulating DHEA levels may be several- fold higher than testosterone concentrations, and rapid peripheral tissue conversion to more potent androgens (androstenedione and testosterone) and estrogens may occur. Moreover, DHEA has relatively low affinity for sex-hormone binding globulin. These factors may enhance the physiologic biopotency of DHEA. -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used -

5Α-Androstane-3Α, 17Β-Diolglucuronide (3 Αdiol
Product Data Sheet: 5α-ANDROSTANE-3α, 17β-DIOL GLUCURONIDE (3α DIOL G) ELISA ENG Catalogue number: RCD007R For research use only! Example Version BioVendor – Laboratorní medicína a.s. Karásek 1767/1, 621 00 Brno, Czech Republic +420 549 124 185 [email protected] [email protected] www.biovendor.com CONTENTS 1. INTENDED USE 3 2. PRINCIPLE OF THE TEST INTRODUCTION 3 3. CLINICAL APPLICATIONS 3 4. PROCEDURAL CAUTIONS AND WARNINGS 4 5. LIMITATIONS 5 6. SAFETY CAUTIONS AND WARNINGS 5 7. SPECIMEN COLLECTION AND STORAGE 5 8. SPECIMEN PRETREATMENT 6 9. REAGENTS AND EQUIPMENT NEEDED BUT NOT PROVIDED ASSAY PROCEDURE 6 10. REAGENTS PROVIDED 6 11. ASSAY PROCEDURE 9 12. CALCULATIONS 10 13. TYPICAL TABULATED DATA 10 14. TYPICAL CALIBRATOR CURVE 11 15. PERFORMANCE CHARACTERISTICS 11 16. EXPECTED NORMAL VALUES 14 17. REFERENCES 14 Example Version ENG.004.A 3 3 1. INTENDED USE For the direct quantitative determination of 3α Diol G by enzyme immunoassay in human serum. 2. PRINCIPLE OF THE TEST INTRODUCTION The principle of the following enzyme immunoassay test follows the typical competitive binding scenario. Competition occurs between an unlabeled antigen (present in standards, control and patient samples) and an enzyme-labelled antigen (conjugate) for a limited number of antibody binding sites on the microplate. The washing and decanting procedures remove unbound materials. After the washing step, the enzyme substrate is added. The enzymatic reaction is terminated by addition of the stopping solution. The absorbance is measured on a microtiter plate reader. The intensity of the colour formed is inversely proportional to the concentration of 3α Diol G in the sample.