South Sudan Covid-19 Addendum
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Warrap State SOUTH SUDAN
COMMUNITY CONSULTATION REPORT Warrap State SOUTH SUDAN Bureau for Community Security South Sudan Peace and Small Arms Control and Reconciliation Commission United Nations Development Programme The Bureau for Community Security and Small Arms Control under the Ministry of Interior is the Gov- ernment agency of South Sudan mandated to address the threats posed by the proliferation of small arms and community insecurity to peace and development. The South Sudan Peace and Reconciliation Commission is mandated to promote peaceful co-existence amongst the people of South Sudan and advise the Government on matters related to peace. The United Nations Development Programme in South Sudan, through the Community Security and Arms Control Project supports the Bureau strengthen its capacity in the area of community security and arms control at the national, state, and county levels. Cover photo: © UNDP/Sun-Ra Lambert Baj COMMUNITY CONSULTATION REPORT Warrap State South Sudan Published by South Sudan Bureau for Community Security and Small Arms Control South Sudan Peace and Reconciliation Commission United Nations Development Programme MAY 2012 JUBA, SOUTH SUDAN CONTENTS Acronyms ........................................................................................................................... i Foreword ........................................................................................................................... .ii Executive Summary ......................................................................................................... -
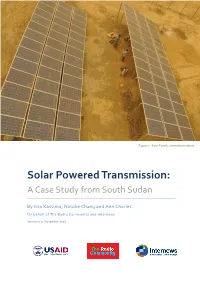
Solar Powered Transmission: a Case Study from South Sudan
Figure 1 – Solar Panels, viewed from above Solar Powered Transmission: A Case Study from South Sudan By Issa Kassimu, Natalie Chang and Ann Charles On behalf of The Radio Community and Internews Version 1.0, November 2016 About The Radio Community The Radio Community (TRC) is a network of community radio stations in South Sudan that reach an estimated 2.1 million potential listeners. These include Mayardit FM in Turalei, Warrap State; Nhomlaau FM in Malualkon, Northern Bahr el Ghazal State; Singaita FM in Kapoeta, Eastern Equatoria State; Mingkaman FM in Awerial County, Lakes State; and Nile FM in Malakal, Upper Nile State (operated in partnership with Internews’ Humanitarian Information Services). Stations in Leer and Nasir are currently off-air due to conflict. About Internews Internews is an international non-profit organization whose mission is to empower local media worldwide to give people the news and information they need, the ability to connect and the means to make their voices heard. Internews provides communities the resources to produce local news and information with integrity and independence. With global expertise and reach, Internews trains both media professionals and citizen journalists, introduces innovative media solutions, increases coverage of vital issues and helps establish policies needed for open access to information. Internews operates internationally, with administrative centers in California, Washington DC, and London, as well as regional hubs in Bangkok and Nairobi. Formed in 1982, Internews has worked in more than 90 countries, and currently has offices in Africa, Asia, Europe, the Middle East, Latin America and North America. Internews Network is registered as a 501(c)3 organization in California, EIN 94-302-7961. -

1 AU Commission of Inquiry on South Sudan Addis Ababa, Ethiopia P. O
AU Commission of Inquiry on South Sudan Addis Ababa, Ethiopia P. O. Box 3243 Telephone: +251 11 551 7700 / +251 11 518 25 58/ Ext 2558 Website: http://www.au.int/en/auciss Original: English FINAL REPORT OF THE AFRICAN UNION COMMISSION OF INQUIRY ON SOUTH SUDAN ADDIS ABABA 15 OCTOBER 2014 1 Table of Contents ACKNOWLEDGEMENTS ............................................................................................... 3 ABBREVIATIONS ........................................................................................................... 5 CHAPTER I ..................................................................................................................... 7 INTRODUCTION ............................................................................................................. 8 CHAPTER II .................................................................................................................. 34 INSTITUTIONS IN SOUTH SUDAN .............................................................................. 34 CHAPTER III ............................................................................................................... 110 EXAMINATION OF HUMAN RIGHTS VIOLATIONS AND OTHER ABUSES DURING THE CONFLICT: ACCOUNTABILITY ......................................................................... 111 CHAPTER IV ............................................................................................................... 233 ISSUES ON HEALING AND RECONCILIATION ....................................................... -

Village Assessment Survey Twic County
Village Assessment Survey COUNTY ATLAS 2013 Twic County Warrap State Village Assessment Survey The Village Assessment Survey (VAS) has been used by IOM since 2007 and is a comprehensive data source for South Sudan that provides detailed information on access to basic services, infra- structure and other key indicators essential to informing the development of efficient reintegra- tion programmes. The most recent VAS represents IOM’s largest effort to date encompassing 30 priority counties comprising of 871 bomas, 197 payams, 468 health facilities, and 1,277 primary schools. There was a particular emphasis on assessing payams outside state capitals, where com- paratively fewer comprehensive assessments have been carried out. IOM conducted the assess- ment in priority counties where an estimated 72% of the returnee population (based on esti- mates as of 2012) has resettled. The county atlas provides spatial data at the boma level and should be used in conjunction with the VAS county profile. Four (4) Counties Assessed Planning Map and Dashboard..…………Page 1 WASH Section…………..………...Page 14 - 20 General Section…………...……...Page 2 - 5 Natural Source of Water……...……….…..Page 14 Main Ethnicities and Languages.………...Page 2 Water Point and Physical Accessibility….…Page 15 Infrastructure and Services……...............Page 3 Water Management & Conflict....….………Page 16 Land Ownership and Settlement Type ….Page 4 WASH Education...….……………….…….Page 17 Returnee Land Allocation Status..……...Page 5 Latrine Type and Use...………....………….Page 18 Livelihood Section…………..…...Page -
Boating on the Nile
United Nations Mission September 2010 InSUDAN Boating on the Nile Published by UNMIS Public Information Office INSIDE 8 August: Meeting with Minister of Humanitarian Affairs Mutrif Siddiq, Joint Special Representative for Darfur 3 Special Focus: Transport Ibrahim Gambari expressed regrets on behalf of the • On every corner Diary African Union-UN Mission in Darfur (UNAMID) over • Boating on the Nile recent events in Kalma and Hamadiya internally displaced persons (IDP) camps in • Once a lifeline South Darfur and their possible negative impacts on the future of the peace process. • Keeping roads open • Filling southern skies 9 August: Blue Nile State members of the Sudan People’s Liberation Movement (SPLM) and National Congress Party (NCP) formed a six-member parliamentary committee charged with raising awareness about popular consultations on Comprehensive Peace Agreement 10 Photo gallery implementation in the state. The Sufi way 10 August: The SPLM and NCP began pre-referendum talks on wealth and power-sharing, 12 Profile demarcating the border, defining citizenship and sharing the Nile waters in preparation for the Knowledge as food southern self-determination vote, scheduled for 9 January 2011. 14 August: Two Jordanian police advisors with UNAMID were abducted in Nyala, Southern Darfur, 13 Environment as they were walking to a UNAMID transport dispatch point 100 meters from their residence. Reclaiming the trees Three days later the two police advisors were released unharmed in Kass, Southern Darfur. 14 Communications 16 August: Members of the Southern Sudan Human Rights Commission elected a nine-member The voice of Miraya steering committee to oversee its activities as the region approaches the self-determination referendum three days later the two police advisor were released unharmed in Kass, Southern Darfur. -

Initial Rapid Needs Assessment Report Internally Displaced Persons in Twic County Warrap from Unity State 3 January 2014
IRNA Report Twic IDPs from Unity State 3 Jan 2014 Initial Rapid Needs Assessment Report Internally Displaced Persons in Twic County Warrap from Unity State 3 January 2014 Important: - IRNA Report should include secondary data collected by all stakeholders and jointly analyzed - IRNA Report should also include community level assessment analysis by clusters and then jointly analyzed by all stakeholders - Report should adequately cover the de-briefing analysis of assessment team leaders - This report should be produced within two days after the IRNA taking place 1 IRNA Report Twic IDPs from Unity State 3 Jan 2014 Situation Overview (use the secondary information as well as the information gathered under the ‘Generalist’ section of the IRNA questionnaire. Map Drivers of Crisis and underlying factors Place map of affected area if available Conflict has spread across South Sudan following an alleged coup attempt three weeks ago in Juba. Among the states directly affected by the crisis is Unity State which neighbours Warrap State to the East. An influx of Internally Displaced People (IDPs) into Warrap’s Twic County has steadily increased since the last week of December Affected population: 2013. Most of those IDPs have been directly attacked or been caught (appox. Male/female and boys/girls) up in the cross fire during the fighting that has ensued in Unity State, while some have run out of seer fear. Displaced population: (appox. Male/female and boys/girls) Scope of crisis and humanitarian profile Most of the displaced are from Mayom County in Unity State, while 3,215 individuals some have been displaced from as far as Bentiu town the Unity State with possible increase in coming days capital itself, in Rubkona County. -

HEALTH CLUSTER BULLETIN # 9 30 September 2018 South Sudan
HEALTH CLUSTER BULLETIN # 9 30 September 2018 A vaccinator administering TT vaccine to a woman of child bearing age in Old Fangak. Photo: CMA. South Sudan Emergency type: Complex Emergency Reporting period: 1 – 30 September 2018 5.1 MILLION PEOPLE 2.4 MILLION 1.96 MILLION 2.1 MILLION IN HEALTH NEED TARGETED DISPLACED REFUGEES HIGHLIGHTS HEALTH SECTOR HEALTH CLUSTER PARTNERS . Following the Ebola virus Disease outbreak in the Democratic 43 EARMARKED IN HRP TO Republic of Congo, the Health Cluster highly involved in IMPLEMENT HEALTH RESPONSE coordinating partners working in high-risk areas. MEDICINES DELIVERED TO HEALTH . Six partners (IOM, CORDAID, CUAMM, SCI, WHO and World FACILITIES/PARTNERS Vision South Sudan, AAHI ) are working in 14 screening sites in ASSORTED EMERGENCY MEDICAL the Yei River, Torit, Maridi, Jubek, Wau, Tambura and Gbude 349 States. KITS (CORE PIPELINE) HEALTH CLUSTER ACTIVITIES . CUAMM, Cordaid, World Vision, IMC and AAH are earmarked to respond in seven isolation facilities located in Yei River, Torit, Maridi, Jubek, Wau, Tambura and Gbude States. Health Link 435 731 OPD CONSULTATIONS South Sudan is coordinating the Ebola presparedness activities in Jubek State. VACCINATION . The Health and Logistics clusters secured funds from the South CHILDREN (6-59 MONTHS) Sudan Humanitarian Fund Reserve allocation to support case 1 950 955 VACCINATED AGAINST management, infection prevention and control, surveillance and MEASLES laboratory capacity. EARLY WARNING ALERT AND RESPONSE NETWORK . Samaritan Purse and Alima are working out modalities to support training of partners on isolation centres and case . management. 41 EWARN SENTINEL SITES FUNDING $US 130 M REQUESTED 34.9* FUNDED GAP 95.1 M Key Context Update . -
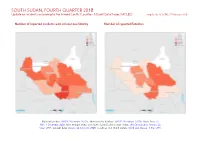
SOUTH SUDAN, FOURTH QUARTER 2018: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 25 February 2020
SOUTH SUDAN, FOURTH QUARTER 2018: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 25 February 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; Abyei Area: SS- NBS, 1 December 2008; Ilemi triangle status and South Sudan/Sudan border status: UN Cartographic Section, Oc- tober 2011; incident data: ACLED, 22 February 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 SOUTH SUDAN, FOURTH QUARTER 2018: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 FEBRUARY 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Violence against civilians 120 48 142 Conflict incidents by category 2 Battles 84 49 156 Development of conflict incidents from December 2016 to December 2018 2 Strategic developments 18 0 0 Protests 6 0 0 Methodology 3 Explosions / Remote 2 1 2 Conflict incidents per province 4 violence Riots 2 0 0 Localization of conflict incidents 4 Total 232 98 300 Disclaimer 5 This table is based on data from ACLED (datasets used: ACLED, 22 February 2020). Development of conflict incidents from December 2016 to December 2018 This graph is based on data from ACLED (datasets used: ACLED, 22 February 2020). 2 SOUTH SUDAN, FOURTH QUARTER 2018: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 FEBRUARY 2020 Methodology sources if necessary. -

SUDAN • ABYEI Crisis Situation Report No
SUDAN • ABYEI crisis Situation Report No. 12 09/06/2011 This report is produced by OCHA in collaboration with humanitarian partners. It covers the period from 7 to 9 June. The next report will be issued on 16 June. I. HIGHLIGHTS/KEY PRIORITIES Humanitarian partners estimate that more than 100,000 people may have been displaced from the Abyei area in the last three weeks. Partners continue to monitor population movements as the situation remains fluid. With more people returning to Agok, the humanitarian presence and activities in the area have also increased. The shortage of fuel for operations and the impact of the rainy season on access to affected locations remain pressing logistic concerns in the ongoing response. II. Situation Overview The situation in Abyei continues to be calm but unpredictable, with sporadic shooting by Sudan Armed Forces (SAF) in Abyei town. The UN has continued to work on negotiating the release of 20-23 civilians in custody of the SAF. This includes 13-14 people held at the time of last reporting, as well as additional 9-10 individuals newly recovered by SAF search teams. The threat of unexploded ordnances in the Abyei area is a cause for concern. UNMIS reported the sighting of unexploded ordnances (UXO) on the southern side of Abyei town, as well as the likelihood of UXOs in Todach village, located close to Abyei town. IOM and the Southern Sudan Relief and Rehab- ilitation Commission continue to monitor population movements of those displaced by the crisis. As of 8 June, the total estimated reported number of persons displaced stood at approximately 101,800. -

South Sudan 2021 Humanitarian Response Plan
HUMANITARIAN HUMANITARIAN PROGRAMME CYCLE 2021 RESPONSE PLAN ISSUED MARCH 2021 SOUTH SUDAN 01 About This document is consolidated by OCHA on behalf of the Humanitarian Country Team and partners. The Humanitarian Response Plan is a presentation of the coordinated, strategic response devised by humanitarian agencies in order to meet the acute needs of people affected by the crisis. It is based on, and responds to, evidence of needs described in the Humanitarian Needs Overview. Manyo Renk Renk SUDAN Kaka Melut Melut Maban Fashoda Riangnhom Bunj Oriny UPPER NILE Abyei region Pariang Panyikang Malakal Abiemnhom Tonga Malakal Baliet Aweil East Abiemnom Rubkona Aweil North Guit Baliet Dajo Gok-Machar War-Awar Twic Mayom Atar 2 Longochuk Bentiu Guit Mayom Old Fangak Aweil West Turalei Canal/Pigi Gogrial East Fangak Aweil Gogrial Luakpiny/Nasir Maiwut Aweil West UNITY Yomding Raja NORTHERN South Gogrial Koch Nyirol Nasir Maiwut Raja BAHR EL Bar Mayen Koch Ulang Kuajok WARRAP Leer Lunyaker Ayod GHAAL Tonj North Mayendit Ayod Aweil Centre Waat Mayendit Leer Uror Warrap Romic ETHIOPIA Yuai Tonj East WESTERN BAHR Nyal Duk Fadiat Akobo Wau Maper JONGLEI CENTRAL EL GHAAL Panyijiar Duk Akobo Kuajiena Rumbek North AFRICAN Wau Tonj Pochalla Jur River Cueibet REPUBLIC Tonj Rumbek Kongor Pochala South Cueibet Centre Yirol East Twic East Rumbek Adior Pibor Rumbek East Nagero Wullu Akot Yirol Bor South Tambura Yirol West Nagero LAKES Awerial Pibor Bor Boma Wulu Mvolo Awerial Mvolo Tambura Terekeka Kapoeta International boundary WESTERN Terekeka North Mundri -
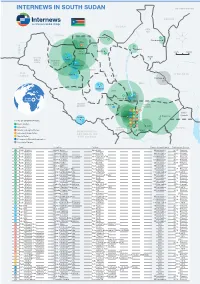
Internews in South Sudan Map Updated May 2020
INTERNEWS IN SOUTH SUDAN MAP UPDATED MAY 2020 SUDAN SUDAN UPPER NILE SUDAN Jamjang 11 3 Gendrassa Abyei 1 2 UNITY 34 Malakal 40 Bentiu 0 km 100 km Turalei 7 SUDAN 4 5 Nasir WESTERN Aweil BAHR EL NORTHERN GHAZAL BAHR EL 32 GHAZAL Kwajok WARRAP D.R. 41 Wau ETHIOPIA CONGO 42 Leer Pochala 36 JONGLEI 37 38 Rumbek LAKES 8 9 10 6 Bor South Awerial Sudan WESTERN Mundri EASTERN EQUATORIA 35 EQUATORIA 12 18 24 30 13 19 25 Ilemi- Kapoeta Dreieck Yambio Juba 14 20 26 15 21 27 31 TYPES OF ORGANIZATIONS 43 16 22 28 Radio Station 17 23 29 Torit Repeaters CENTRAL KENYA Media Training Institution EQUATORIA Magwi DEMOCRATIC 33 Advocacy Organization REPUBLIC OF Media Outlet THE CONGO Community-Based Organization UGANDA Associate Partner Type Location Partner Reach (if applicable) Partnership Active 1 Radio Station Abyei, Agok Abyei FM 60 km radius 2015 - Present 3 Radio Station Jamjang, Unity Jamjang FM 60 km radius 2016 - Pesent 4 Radio Station Aweil, Northern Bahr el Ghazal Akol Yam 91.0FM 150 km radius 2017 - Present 6 Radio Station Awerial, Lakes Mingkaman 100FM 150 km radius 2014 - Present 7 Radio Station Bentiu, Unity Kondial FM 30 km radius 2018 - Present 8 Radio Station Bor, Jonglei Radio Jonglei 50 km radius 2018 11 Radio Station Gendrassa, Upper Nile Radio Salam 30 km radius 2019 - Present 19 Radio Station Juba, Central Equatoria Radio Bakhita 100 km radius 2015-2016 23 Radio Station Juba, Central Equatoria Advance Youth Radio 50 km radius 2019 - Present 26 Radio Station Juba, Central Equatoria Eye Radio 60 km radius 2014 - Present 28 Radio Station -

Small Arms Survey/HSBA: "The Conflict in Unity State"
The Conflict in Unity State Describing events through 29 January 2015 It is now thirteen months since the beginning of the South Sudanese conflict. Both the Sudan People’s Liberation Movement/Army (SPLM/A) and the Sudan People’s Liberation Movement/Army in Opposition (SPLM/A-IO) have spent the rainy season reinforcing their military positions in Unity state—as elsewhere—in anticipation of a dry season military campaign. The beginning of 2015 has already seen clashes just south of Bentiu—the state capital—in Guit county, and around the oil fields of Rubkona and Pariang counties. As of January 2015, the SPLA maintains control of the northern and western counties of Pariang and Abiemnom, as well as of Bentiu. The SPLA-IO controls Unity’s southern counties, and much of Guit and Rubkona. Mayom, a strategically important county that contains the road from Warrap state— along which SPLA reinforcements could travel—is largely under the control of the SPLA. As dry season begins, the frontlines are just south of Bentiu, in Guit and Rubkona, and just north and west of the oil fields in Rubkona and Pariang: both the oil fields and the state capital will be important SPLA-IO strategic targets in the coming months. Peace negotiations, which continued during the rainy season, have failed to overcome the substantial divergences between the two sides’ positions. An intra-SPLM dialogue recently took place in Arusha, Tanzania, and resulted in an agreement signed on 21 January by the SPLM, SPLM-IO, and the representative of the SPLM detainees, Deng Alor.