Laser Information and Safety
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
An Application of the Theory of Laser to Nitrogen Laser Pumped Dye Laser
SD9900039 AN APPLICATION OF THE THEORY OF LASER TO NITROGEN LASER PUMPED DYE LASER FATIMA AHMED OSMAN A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Physics. UNIVERSITY OF KHARTOUM FACULTY OF SCIENCE DEPARTMENT OF PHYSICS MARCH 1998 \ 3 0-44 In this thesis we gave a general discussion on lasers, reviewing some of are properties, types and applications. We also conducted an experiment where we obtained a dye laser pumped by nitrogen laser with a wave length of 337.1 nm and a power of 5 Mw. It was noticed that the produced radiation possesses ^ characteristic^ different from those of other types of laser. This' characteristics determine^ the tunability i.e. the possibility of choosing the appropriately required wave-length of radiation for various applications. DEDICATION TO MY BELOVED PARENTS AND MY SISTER NADI A ACKNOWLEDGEMENTS I would like to express my deep gratitude to my supervisor Dr. AH El Tahir Sharaf El-Din, for his continuous support and guidance. I am also grateful to Dr. Maui Hammed Shaded, for encouragement, and advice in using the computer. Thanks also go to Ustaz Akram Yousif Ibrahim for helping me while conducting the experimental part of the thesis, and to Ustaz Abaker Ali Abdalla, for advising me in several respects. I also thank my teachers in the Physics Department, of the Faculty of Science, University of Khartoum and my colleagues and co- workers at laser laboratory whose support and encouragement me created the right atmosphere of research for me. Finally I would like to thank my brother Salah Ahmed Osman, Mr. -

‰M‰Mwm Cixþvi Cék² I Dîi
gBs‡iwRƒj eBGqi 1g cÎ AwZwiÚ Ask 275 ‰m‰mwm cixÞvi cÉk² I Dîi 1. Dhaka Board-2015 English (Compulsory) 1st Paper Read the passage. Then answer the questions below. The National Memorial at Savar is a symbol of the nation's respect for the martyrs of the War of Liberation. It is built with concrete, but made of blood. It stands 150 feet tall, but every martyr it stands for stands so much taller. It is an achievement the dimension of which can be measured, but it stands for an achievement, which is immeasurable. It stands upright for the millions of martyrs who laid down their lives so that we may stand upright, in honour and dignity, amongst the nations of the world. Most prominently visible is the 150 feet tower that stands on a base measuring 130 feet wide. There are actually a series of 7 towers that rise by stages to a height of 150 feet. The foundation was laid on the first anniversary of the Victory Day. There is actually a plan to build a huge complex in several phases. The entire complex will cover an area of 126 acres. The plan of this complex includes a mosque, a library and a museum. The relics of the Liberation War will be kept in the museum. They will ever remind our countrymen and all who would come to visit museum of the valiant struggle and supreme sacrifices of a freedom loving people. Here also will be a clear warning to all oppressors that the weapons of freedom need not be very big, and that oppression will always be defeated. -

Self Amplified Lock of a Ultra-Narrow Linewidth Optical Cavity
Self Amplified Lock of a Ultra-narrow Linewidth Optical Cavity Kiwamu Izumi,1, ∗ Daniel Sigg,1 and Lisa Barsotti2 1LIGO Hanford Observatory, PO Box 159 Richland, Washington 99354, USA 2LIGO laboratory, Massachusetts Institute of Technology, Cambridge, Massachussetts 02139, USA compiled: January 8, 2016 High finesse optical cavities are an essential tool in modern precision laser interferometry. The incident laser field is often controlled and stabilized with an active feedback system such that the field resonates in the cavity. The Pound-Drever-Hall reflection locking technique is a convenient way to derive a suitable error signal. However, it only gives a strong signal within the cavity linewidth. This poses a problem for locking a ultra-narrow linewidth cavity. We present a novel technique for acquiring lock by utilizing an additional weak control signal, but with a much larger capture range. We numerically show that this technique can be applied to the laser frequency stabilization system used in the Laser Interferometric Gravitational-wave Observatory (LIGO) which has a linewidth of 0.8 Hz. This new technique will allow us to robustly and repeatedly lock the LIGO laser frequency to the common mode of the interferometer. OCIS codes: (140.3425), (140.3410) http://dx.doi.org/10.1364/XX.99.099999 High finesse optical cavities have been an indispens- nonlinear response [8, 9] dominant and thus hinder the able tool for precision interferometry to conduct rela- linear controller. tivistic experiments such as gravitational wave detection Gravitational wave observatories deploy kilometer [1{3] and optical clocks [4]. The use of a high finesse cav- scale interferometers with extremely narrow linewidth. -

Thesis Rests with Its Author
University of Bath PHD New vacuum solutions for quadratic metric–affine gravity Pasic, Vedad Award date: 2009 Awarding institution: University of Bath Link to publication Alternative formats If you require this document in an alternative format, please contact: [email protected] General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 23. Sep. 2021 New Vacuum Solutions for Quadratic Metric–affine Gravity submitted by Vedad Pasiˇ c´ for the degree of Doctor of Philosophy of the University of Bath Department of Mathematical Sciences February 2009 COPYRIGHT Attention is drawn to the fact that copyright of this thesis rests with its author. This copy of the thesis has been supplied on the condition that anyone who consults it is understood to recognise that its copyright rests with its author and that no quotation from the thesis and no information derived from it may be published without the prior written consent of the author. -
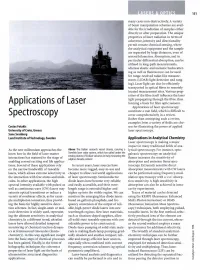
Applications of Laser Spectroscopy Constitute a Vast Field, Which Is Difficult to Spectroscopy Cover Comprehensively in a Review
LASERS & OPTICS 151 many cases non-destructively. A variety of beam manipulation schemes are avail able for the irradiation of samples either directly or after preparation. The unique properties of laser radiation in terms of coherence, intensity and directionality permit remote chemical sensing, where the analytical equipment and the sample are separated by large distances, even of several kilometres. Absorption, and in particular differential absorption, can be utilised in long-path measurements, whereas elastic and inelastic backscatter- ing as well as fluorescence can be used for range-resolved radar-like measure ments (LIDAR: light detection and rang ing). Laser light can also be efficiently transported in optical fibres to remotely located measurement sites. Various prop erties of the fibre itself influence the laser light propagating through the fibre, thus Applications of Laser forming a basis for fibre optic sensors. Applications of laser spectroscopy constitute a vast field, which is difficult to Spectroscopy cover comprehensively in a review. Rather than attempting such a review, examples from a variety of fields are cho Costas Fotakis sen for illustrating the power of applied University of Crete, Greece laser spectroscopy. Sune Svanberg Lund Institute of Technology, Sweden Applications in Analytical Chemistry Laser spectroscopy is making a major impact in many traditional fields of ana As the new millennium approaches the Above The Italian research vessel Urania, carrying a lytical spectroscopy. For instance, opto- know how in the field of laser-matter Swedish laser radar system, which has sailed under the galvanic spectroscopy on analytical smoky plumes of Sicilian volcanos in Italy measuring the interactions has matured to the stage of sulphur dioxide content flames increases the sensitivity of enabling several exciting real life applica absorption and emission flame spec tions. -

HD DVD: Manufacturing Was Developed.This Recorder Is Equipped with a 257Nm Gas Laser (Frequency Doubled Ar+ Laser)
paper r& white d Six years ago, the LDM 3692 DUV recorder HD DVD: Manufacturing was developed.This recorder is equipped with a 257nm gas laser (frequency doubled Ar+ laser). All options with regards to future for- mats were still open at that time.The recorder features two recording spots, with a wobble The New Format option on both. This recorder is an adequate R&D tool to record HD DVD. BY DR. DICK VERHAART, from 740nm to 400nm. To read these smaller For HD DVD stamper manufacturing, a Singulus Mastering information structures, it is necessary to use recorder with a 266nm solid state laser was PETER KNIPS, blue diode lasers with a wavelength of 405nm developed. This system contains a stable and Singulus EMould instead of the 650nm red lasers used for CD easy to operate solid state laser, with a much DIETER WAGNER, and DVD. longer lifetime than the gas laser. As all pro- Singulus Technologies AG An advanced copy protection system will posed next-generation formats require only The third generation of optical disc formats is give better protection than what was avail- one spot, the system has a single recording set to arrive on the market by the end of this able for CD and DVD with mandatory serializ- spot. Spot deflection, required to create the year.As with Blu-ray Disc, the HD DVD format ing of each single HD DVD. The serialization groove wobble in the recordable and was developed to tremendously increase the will take place on the aluminum covered layer rewritable formats, is available as an option. -

Platinum Sponsor
We like to thank the Department of Biotechnology (Government of India) for financial support. We like to thank our sponsors for financial support: Platinum Sponsor: Gold Sponsor: Silver Sponsors: And Program Date Venue Timings Title OF MUSIC, MATH AND MEASUREMENT LH1 6pm M.W. Linscheid, Humbold Universitaet Berlin, Germany Dining Mixer 23/08 7pm Complex Concert by Ananth Menon Quartet Dining 8pm Dinner Complex LH1 9:00am Tutorial I MASS SPECTROMETRIC ESSENTIALS IN OMICS RESEARCH D.Schwudke LH1 9:30am Session I / Proteomics (Chair D. Schwud ke) MASS SPECTROMETRIC IDENTIFICATION OF A NOVEL TRANS- SPLICING EVENT IN GIARDIA LAMBLIA HEAT SHOCK PROTEIN 90 U.S. Tatu, IISC Bangalore, India REVISITING PROTEOMICS OF GLIOMAS: DIFFERENTIAL MEMBRANE PROTEINS AND MOLECULAR INSIGHTS R. Sirdeshmukh, IOB Bangalore, India NEW HIGH SELECTIVITY WORKFLOWS FOR TARGETED QUANTITATIVE PROTEOMICS 24/08 M. Cafazzo, AB Sciex, US Break ABSOLUTE QUANTIFICATION OF PROTEINS AND PEPTIDES - USE OF METAL CODING AND LC/MS WITH ICP AND ELECTROSPRAY M.W. Linscheid, Humbold Universitaet Berlin, Germany MATERNAL VITAMIN B12 DEFICIENCY INDUCED ALTERATION IN PROTEIN EXPRESSION IN RAT OFFSPRING S. Sengupta, IGIB New Dehli, India CLINICAL PROTEOMICS OF EYE DISEASES K. Dharmalingam, Madurai Kamaraj University, India Dining 1pm Lunch Complex Ope n 2pm Poster Session I Deck Date Venue Timings Title LH1 4pm Session II / Lipidomics (Chair S. Hebbar ) TOWARDS THE COMPLETE STRUCTURE ELUCIDATION OF COMPLEX LIPIDS BY MASS SPECTROMETRY: NOVEL APPROACHES TO ION ACTIVATION S. Blanksby et al., University of Wollongong, Australia LIPIDOMICS AT THE HIGH MASS RESOLUTION A. Shevchenko, MPI-CBG Dresden, Germany STRATEGIES FOR IMAGING BIOMOLECULES BY TOF-SIMS AND MALDI-TOF/TOF MASS SPECTROMETRY O. -

From Theory to the First Working Laser Laser History—Part I
I feature_ laser history From theory to the first working laser Laser history—Part I Author_Ingmar Ingenegeren, Germany _The principle of both maser (microwave am- 19 US patents) using a ruby laser. Both were nom- plification by stimulated emission of radiation) inated for the Nobel Prize. Gábor received the 1971 and laser (light amplification by stimulated emis- Nobel Prize in Physics for the invention and devel- sion of radiation) were first described in 1917 by opment of the holographic method. To a friend he Albert Einstein (Fig.1) in “Zur Quantentheorie der wrote that he was ashamed to get this prize for Strahlung”, as the so called ‘stimulated emission’, such a simple invention. He was the owner of more based on Niels Bohr’s quantum theory, postulated than a hundred patents. in 1913, which explains the actions of electrons in- side atoms. Einstein (born in Germany, 14 March In 1954 at the Columbia University in New York, 1879–18 April 1955) received the Nobel Prize for Charles Townes (born in the USA, 28 July 1915–to- physics in 1921, and Bohr (born in Denmark, 7 Oc- day, Fig. 2) and Arthur Schawlow (born in the USA, tober 1885–18 November 1962) in 1922. 5 Mai 1921–28 April 1999, Fig. 3) invented the maser, using ammonia gas and microwaves which In 1947 Dennis Gábor (born in Hungarian, 5 led to the granting of a patent on March 24, 1959. June 1900–8 February 1972) developed the theory The maser was used to amplify radio signals and as of holography, which requires laser light for its re- an ultra sensitive detector for space research. -

Power Build-Up Cavity Coupled to a Laser Diode
I POWER BUILD-UP CAVITY COUPLED I TO A LASER DIODE Daniel J. Evans I Center of Excellence for Raman Technology University of Utah I Abstract combination of these elements will emit photons at different frequencies. The ends of these semiconductor In many Raman applications there is a need to devices are cleaved to form mirrors that bounce the I detect gases in the low ppb range. The desired photons back and forth within the cavity. The photons sensitivity can be achieved by using a high power laser excite more electrons, which form more photons source in the range of tens of watts. A system (referred to as optical pumping). 2 A certain portion of I combining a build-up cavity to enhance the power and the photons emit through the front and back cleaved an external cavity laser diode setup to narrow the surfaces of the laser diode. The amount of photons that bandwidth can give the needed power to the Raman get through the cleaved surfaces can be adjusted by I spectroscopy system. coating the surface or installing other mirrors. Introduction to Laser Diodes The planar cleaved surfaces of the laser diode form a Fabry-Perot cavity with set resonance frequencies I An important characteristic of all lasers is the (vp).3 The typical laser diode has a spacing of 150 f.1I11 mode structure. The mode structure refers to both the with an index of refraction of 3.5, yielding a resonance lasing frequency and the spatial characteristics of the frequency of 285 GHz. The wavelength spacing (~A.) I laser. -
Chapter 2 HISTORY and DEVELOPMENT of MILITARY LASERS
History and Development of Military Lasers Chapter 2 HISTORY AND DEVELOPMENT OF MILITARY LASERS JACK B. KELLER, JR* INTRODUCTION INVENTING THE LASER MILITARIZING THE LASER SEARCHING FOR HIGH-ENERGY LASER WEAPONS SEARCHING FOR LOW-ENERGY LASER WEAPONS RETURNING TO HIGHER ENERGIES SUMMARY *Lieutenant Colonel, US Army (Retired); formerly, Foreign Science Information Officer, US Army Medical Research Detachment-Walter Reed Army Institute of Research, 7965 Dave Erwin Drive, Brooks City-Base, Texas 78235 25 Biomedical Implications of Military Laser Exposure INTRODUCTION This chapter will examine the history of the laser, Military advantage is greatest when details are con- from theory to demonstration, for its impact upon the US cealed from real or potential adversaries (eg, through military. In the field of military science, there was early classification). Classification can remain in place long recognition that lasers can be visually and cutaneously after a program is aborted, if warranted to conceal hazardous to military personnel—hazards documented technological details or pathways not obvious or easily in detail elsewhere in this volume—and that such hazards deduced but that may be relevant to future develop- must be mitigated to ensure military personnel safety ments. Thus, many details regarding developmental and mission success. At odds with this recognition was military laser systems cannot be made public; their the desire to harness the laser’s potential application to a descriptions here are necessarily vague. wide spectrum of military tasks. This chapter focuses on Once fielded, system details usually, but not always, the history and development of laser systems that, when become public. Laser systems identified here represent used, necessitate highly specialized biomedical research various evolutionary states of the art in laser technol- as described throughout this volume. -

Main Types of Lasers Used for Manufacturing- Key Properties and Key Applications
Main Types of Lasers Used for Manufacturing- Key Properties and Key Applications Tom Kugler Fiber Systems Mgr. Laser Mechanisms, Inc. www.lasermech.com LME 2011 Topics • Laser Output Wavelengths • Laser Average Power • Laser Output Waveforms (Pulsing) • Laser Peak Power • Laser Beam Quality (Focusability) • Key Properties • Key Applications • Beam Delivery Styles 2 Tom Kugler- Laser Mechanisms Compared to standard light sources… • Laser Light is Collimated- the light rays are parallel to and diverge very slowly- they stay concentrated over long distances- that is a “laser beam” • Laser Light has high Power Density- parallel laser light has a power density in watts/cm2 that is over 1000 times that of ordinary incandescent light • Laser Light is Monochromatic- one color (wavelength) so optics are simplified and perform better • Laser light is highly Focusable- low divergence, small diameter beams, and monochromatic light mean the laser can be focused to a small focal point producing power densities at focus 1,000,000,000 times more than ordinary light. 3 Tom Kugler- Laser Mechanisms Laser Light • 100W of laser light focused to a diameter of 100um produces a power density of 1,270,000 Watts per square centimeter! 4 Tom Kugler- Laser Mechanisms Examples of Laser Types • Gas Lasers: Electrical Discharge in a Gas Mixture Excites Laser Action: – Carbon Dioxide (CO2) – Excimer (XeCl, KrF, ArF, XeF) • Light Pumped Solid State Lasers: Light from Lamps or Diodes Excites Ions in a Host Crystal or Glass: – Nd:YAG (Neodymium doped Yttrium Aluminum -
FABRICATION of TRANSPARENT CERAMIC LASER MEDIA for HIGH ENERGY LASER APPLICATIONS Karn Serivalsatit Clemson University, [email protected]
Clemson University TigerPrints All Dissertations Dissertations 5-2010 FABRICATION OF TRANSPARENT CERAMIC LASER MEDIA FOR HIGH ENERGY LASER APPLICATIONS Karn Serivalsatit Clemson University, [email protected] Follow this and additional works at: https://tigerprints.clemson.edu/all_dissertations Part of the Materials Science and Engineering Commons Recommended Citation Serivalsatit, Karn, "FABRICATION OF TRANSPARENT CERAMIC LASER MEDIA FOR HIGH ENERGY LASER APPLICATIONS" (2010). All Dissertations. 525. https://tigerprints.clemson.edu/all_dissertations/525 This Dissertation is brought to you for free and open access by the Dissertations at TigerPrints. It has been accepted for inclusion in All Dissertations by an authorized administrator of TigerPrints. For more information, please contact [email protected]. FABRICATION OF TRANSPARENT CERAMIC LASER MEDIA FOR HIGH ENERGY LASER APPLICATIONS A Dissertation Presented to the Graduate School of Clemson University In Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy Materials Science and Engineering by Karn Serivalsatit May 2010 Accepted by: Dr. John Ballato, Committee Chair Dr. Stephen Foulger Dr. Jian Luo Dr. Eric Skaar i ABSTRACT Sesquioxides of yttrium, scandium, and lutetium, i.e., Y2O3, Sc 2O3, and Lu 2O3, have received a great deal of recent attention as potential high power solid state laser hosts. These oxides are receptive to lanthanide doping, including trivalent Er, Ho and Tm which have well known emissions at eye-safe wavelengths that can be excited using commercial diode lasers. These sesquioxides are considered superior to the more conventional yttrium aluminum garnet (YAG) due to their higher thermal conductivity, which is critical for high power laser system. Unfortunately, these oxides possess high melting temperatures, which make the growth of high purity and quality crystals using melt techniques difficult.