Whole Transcriptome Targeted Gene Quantification Provides New Insights
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Regulation and Dysregulation of Chromosome Structure in Cancer
Regulation and Dysregulation of Chromosome Structure in Cancer The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Hnisz, Denes et al. “Regulation and Dysregulation of Chromosome Structure in Cancer.” Annual Review of Cancer Biology 2, 1 (March 2018): 21–40 © 2018 Annual Reviews As Published https://doi.org/10.1146/annurev-cancerbio-030617-050134 Version Author's final manuscript Citable link http://hdl.handle.net/1721.1/117286 Terms of Use Creative Commons Attribution-Noncommercial-Share Alike Detailed Terms http://creativecommons.org/licenses/by-nc-sa/4.0/ Regulation and dysregulation of chromosome structure in cancer Denes Hnisz1*, Jurian Schuijers1, Charles H. Li1,2, Richard A. Young1,2* 1 Whitehead Institute for Biomedical Research, 455 Main Street, Cambridge, MA 02142, USA 2 Department of Biology, Massachusetts Institute of Technology, Cambridge, MA 02139, USA * Corresponding authors Corresponding Authors: Denes Hnisz Whitehead Institute for Biomedical Research 455 Main Street Cambridge, MA 02142 Tel: (617) 258-7181 Fax: (617) 258-0376 [email protected] Richard A. Young Whitehead Institute for Biomedical Research 455 Main Street Cambridge, MA 02142 Tel: (617) 258-5218 Fax: (617) 258-0376 [email protected] 1 Summary Cancer arises from genetic alterations that produce dysregulated gene expression programs. Normal gene regulation occurs in the context of chromosome loop structures called insulated neighborhoods, and recent studies have shown that these structures are altered and can contribute to oncogene dysregulation in various cancer cells. We review here the types of genetic and epigenetic alterations that influence neighborhood structures and contribute to gene dysregulation in cancer, present models for insulated neighborhoods associated with the most prominent human oncogenes, and discuss how such models may lead to further advances in cancer diagnosis and therapy. -

Defining Functional Interactions During Biogenesis of Epithelial Junctions
ARTICLE Received 11 Dec 2015 | Accepted 13 Oct 2016 | Published 6 Dec 2016 | Updated 5 Jan 2017 DOI: 10.1038/ncomms13542 OPEN Defining functional interactions during biogenesis of epithelial junctions J.C. Erasmus1,*, S. Bruche1,*,w, L. Pizarro1,2,*, N. Maimari1,3,*, T. Poggioli1,w, C. Tomlinson4,J.Lees5, I. Zalivina1,w, A. Wheeler1,w, A. Alberts6, A. Russo2 & V.M.M. Braga1 In spite of extensive recent progress, a comprehensive understanding of how actin cytoskeleton remodelling supports stable junctions remains to be established. Here we design a platform that integrates actin functions with optimized phenotypic clustering and identify new cytoskeletal proteins, their functional hierarchy and pathways that modulate E-cadherin adhesion. Depletion of EEF1A, an actin bundling protein, increases E-cadherin levels at junctions without a corresponding reinforcement of cell–cell contacts. This unexpected result reflects a more dynamic and mobile junctional actin in EEF1A-depleted cells. A partner for EEF1A in cadherin contact maintenance is the formin DIAPH2, which interacts with EEF1A. In contrast, depletion of either the endocytic regulator TRIP10 or the Rho GTPase activator VAV2 reduces E-cadherin levels at junctions. TRIP10 binds to and requires VAV2 function for its junctional localization. Overall, we present new conceptual insights on junction stabilization, which integrate known and novel pathways with impact for epithelial morphogenesis, homeostasis and diseases. 1 National Heart and Lung Institute, Faculty of Medicine, Imperial College London, London SW7 2AZ, UK. 2 Computing Department, Imperial College London, London SW7 2AZ, UK. 3 Bioengineering Department, Faculty of Engineering, Imperial College London, London SW7 2AZ, UK. 4 Department of Surgery & Cancer, Faculty of Medicine, Imperial College London, London SW7 2AZ, UK. -

Increased Expression of the Tail-Anchored Membrane Protein SLMAP in Adipose Tissue from Type 2 Tally Ho Diabetic Mice
Hindawi Publishing Corporation Experimental Diabetes Research Volume 2011, Article ID 421982, 10 pages doi:10.1155/2011/421982 Research Article Increased Expression of the Tail-Anchored Membrane Protein SLMAP in Adipose Tissue from Type 2 Tally Ho Diabetic Mice Xiaoliang Chen1 and Hong Ding2 1 Second People Hospital of Hangzhou, No. 1 Wenzhou Road, Hangzhou 310015, China 2 Department of Pharmacology, Weill Cornell Medical College in Qatar, P.O. Box 24144, Doha, Qatar Correspondence should be addressed to Hong Ding, [email protected] Received 6 April 2011; Accepted 5 May 2011 Academic Editor: N. Cameron Copyright © 2011 X. Chen and H. Ding. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The tail-anchored membrane protein, sarcolemmal membrane associated protein (SLMAP) is encoded to a single gene that maps to the chromosome 3p14 region and has also been reported in certain diabetic populations. Our previous studies with db/db mice shown that a deregulation of SLMAP expression plays an important role in type 2 diabetes. Male Tally Ho mice were bred to present with either normoglycemia (NG) or hyperglycemia (HG). Abdominal adipose tissue from male Tally Ho mice of the HG group was found to have a significantly lower expression of the membrane associated glucose transporter-4 (GLUT-4) and higher expression of SLMAP compared to tissue from NG mice. There were 3 isoforms expressed in the abdominal adipose tissue, but only 45 kDa isoform of SLMAP was associated with the GLUT-4 revealed by immunoprecipitation data. -
0.5) in Stat3∆/∆ Compared with Stat3flox/Flox
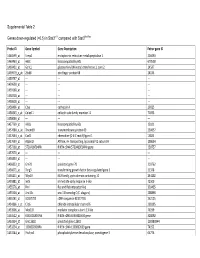
Supplemental Table 2 Genes down-regulated (<0.5) in Stat3∆/∆ compared with Stat3flox/flox Probe ID Gene Symbol Gene Description Entrez gene ID 1460599_at Ermp1 endoplasmic reticulum metallopeptidase 1 226090 1460463_at H60c histocompatibility 60c 670558 1460431_at Gcnt1 glucosaminyl (N-acetyl) transferase 1, core 2 14537 1459979_x_at Zfp68 zinc finger protein 68 24135 1459747_at --- --- --- 1459608_at --- --- --- 1459168_at --- --- --- 1458718_at --- --- --- 1458618_at --- --- --- 1458466_at Ctsa cathepsin A 19025 1458345_s_at Colec11 collectin sub-family member 11 71693 1458046_at --- --- --- 1457769_at H60a histocompatibility 60a 15101 1457680_a_at Tmem69 transmembrane protein 69 230657 1457644_s_at Cxcl1 chemokine (C-X-C motif) ligand 1 14825 1457639_at Atp6v1h ATPase, H+ transporting, lysosomal V1 subunit H 108664 1457260_at 5730409E04Rik RIKEN cDNA 5730409E04Rik gene 230757 1457070_at --- --- --- 1456893_at --- --- --- 1456823_at Gm70 predicted gene 70 210762 1456671_at Tbrg3 transforming growth factor beta regulated gene 3 21378 1456211_at Nlrp10 NLR family, pyrin domain containing 10 244202 1455881_at Ier5l immediate early response 5-like 72500 1455576_at Rinl Ras and Rab interactor-like 320435 1455304_at Unc13c unc-13 homolog C (C. elegans) 208898 1455241_at BC037703 cDNA sequence BC037703 242125 1454866_s_at Clic6 chloride intracellular channel 6 209195 1453906_at Med13l mediator complex subunit 13-like 76199 1453522_at 6530401N04Rik RIKEN cDNA 6530401N04 gene 328092 1453354_at Gm11602 predicted gene 11602 100380944 1453234_at -

DNA Replication Stress Response Involving PLK1, CDC6, POLQ
DNA replication stress response involving PLK1, CDC6, POLQ, RAD51 and CLASPIN upregulation prognoses the outcome of early/mid-stage non-small cell lung cancer patients C. Allera-Moreau, I. Rouquette, B. Lepage, N. Oumouhou, M. Walschaerts, E. Leconte, V. Schilling, K. Gordien, L. Brouchet, Mb Delisle, et al. To cite this version: C. Allera-Moreau, I. Rouquette, B. Lepage, N. Oumouhou, M. Walschaerts, et al.. DNA replica- tion stress response involving PLK1, CDC6, POLQ, RAD51 and CLASPIN upregulation prognoses the outcome of early/mid-stage non-small cell lung cancer patients. Oncogenesis, Nature Publishing Group: Open Access Journals - Option C, 2012, 1, pp.e30. 10.1038/oncsis.2012.29. hal-00817701 HAL Id: hal-00817701 https://hal.archives-ouvertes.fr/hal-00817701 Submitted on 9 Jun 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution - NonCommercial - NoDerivatives| 4.0 International License Citation: Oncogenesis (2012) 1, e30; doi:10.1038/oncsis.2012.29 & 2012 Macmillan Publishers Limited All rights reserved 2157-9024/12 www.nature.com/oncsis ORIGINAL ARTICLE DNA replication stress response involving PLK1, CDC6, POLQ, RAD51 and CLASPIN upregulation prognoses the outcome of early/mid-stage non-small cell lung cancer patients C Allera-Moreau1,2,7, I Rouquette2,7, B Lepage3, N Oumouhou3, M Walschaerts4, E Leconte5, V Schilling1, K Gordien2, L Brouchet2, MB Delisle1,2, J Mazieres1,2, JS Hoffmann1, P Pasero6 and C Cazaux1 Lung cancer is the leading cause of cancer deaths worldwide. -
Multidrug Transporter MRP4/ABCC4 As a Key Determinant of Pancreatic
www.nature.com/scientificreports OPEN Multidrug transporter MRP4/ ABCC4 as a key determinant of pancreatic cancer aggressiveness A. Sahores1, A. Carozzo1, M. May1, N. Gómez1, N. Di Siervi1, M. De Sousa Serro1, A. Yanef1, A. Rodríguez‑González2, M. Abba3, C. Shayo2 & C. Davio1* Recent fndings show that MRP4 is critical for pancreatic ductal adenocarcinoma (PDAC) cell proliferation. Nevertheless, the signifcance of MRP4 protein levels and function in PDAC progression is still unclear. The aim of this study was to determine the role of MRP4 in PDAC tumor aggressiveness. Bioinformatic studies revealed that PDAC samples show higher MRP4 transcript levels compared to normal adjacent pancreatic tissue and circulating tumor cells express higher levels of MRP4 than primary tumors. Also, high levels of MRP4 are typical of high-grade PDAC cell lines and associate with an epithelial-mesenchymal phenotype. Moreover, PDAC patients with high levels of MRP4 depict dysregulation of pathways associated with migration, chemotaxis and cell adhesion. Silencing MRP4 in PANC1 cells reduced tumorigenicity and tumor growth and impaired cell migration. Transcriptomic analysis revealed that MRP4 silencing alters PANC1 gene expression, mainly dysregulating pathways related to cell-to-cell interactions and focal adhesion. Contrarily, MRP4 overexpression signifcantly increased BxPC-3 growth rate, produced a switch in the expression of EMT markers, and enhanced experimental metastatic incidence. Altogether, our results indicate that MRP4 is associated with a more aggressive phenotype in PDAC, boosting pancreatic tumorigenesis and metastatic capacity, which could fnally determine a fast tumor progression in PDAC patients. Pancreatic ductal adenocarcinoma (PDAC) is one of the most lethal human malignancies, due to its late diag- nosis, inherent resistance to treatment and early dissemination 1. -

Supplemental Information
Supplemental information Dissection of the genomic structure of the miR-183/96/182 gene. Previously, we showed that the miR-183/96/182 cluster is an intergenic miRNA cluster, located in a ~60-kb interval between the genes encoding nuclear respiratory factor-1 (Nrf1) and ubiquitin-conjugating enzyme E2H (Ube2h) on mouse chr6qA3.3 (1). To start to uncover the genomic structure of the miR- 183/96/182 gene, we first studied genomic features around miR-183/96/182 in the UCSC genome browser (http://genome.UCSC.edu/), and identified two CpG islands 3.4-6.5 kb 5’ of pre-miR-183, the most 5’ miRNA of the cluster (Fig. 1A; Fig. S1 and Seq. S1). A cDNA clone, AK044220, located at 3.2-4.6 kb 5’ to pre-miR-183, encompasses the second CpG island (Fig. 1A; Fig. S1). We hypothesized that this cDNA clone was derived from 5’ exon(s) of the primary transcript of the miR-183/96/182 gene, as CpG islands are often associated with promoters (2). Supporting this hypothesis, multiple expressed sequences detected by gene-trap clones, including clone D016D06 (3, 4), were co-localized with the cDNA clone AK044220 (Fig. 1A; Fig. S1). Clone D016D06, deposited by the German GeneTrap Consortium (GGTC) (http://tikus.gsf.de) (3, 4), was derived from insertion of a retroviral construct, rFlpROSAβgeo in 129S2 ES cells (Fig. 1A and C). The rFlpROSAβgeo construct carries a promoterless reporter gene, the β−geo cassette - an in-frame fusion of the β-galactosidase and neomycin resistance (Neor) gene (5), with a splicing acceptor (SA) immediately upstream, and a polyA signal downstream of the β−geo cassette (Fig. -

Supplementary Table S1. Correlation Between the Mutant P53-Interacting Partners and PTTG3P, PTTG1 and PTTG2, Based on Data from Starbase V3.0 Database
Supplementary Table S1. Correlation between the mutant p53-interacting partners and PTTG3P, PTTG1 and PTTG2, based on data from StarBase v3.0 database. PTTG3P PTTG1 PTTG2 Gene ID Coefficient-R p-value Coefficient-R p-value Coefficient-R p-value NF-YA ENSG00000001167 −0.077 8.59e-2 −0.210 2.09e-6 −0.122 6.23e-3 NF-YB ENSG00000120837 0.176 7.12e-5 0.227 2.82e-7 0.094 3.59e-2 NF-YC ENSG00000066136 0.124 5.45e-3 0.124 5.40e-3 0.051 2.51e-1 Sp1 ENSG00000185591 −0.014 7.50e-1 −0.201 5.82e-6 −0.072 1.07e-1 Ets-1 ENSG00000134954 −0.096 3.14e-2 −0.257 4.83e-9 0.034 4.46e-1 VDR ENSG00000111424 −0.091 4.10e-2 −0.216 1.03e-6 0.014 7.48e-1 SREBP-2 ENSG00000198911 −0.064 1.53e-1 −0.147 9.27e-4 −0.073 1.01e-1 TopBP1 ENSG00000163781 0.067 1.36e-1 0.051 2.57e-1 −0.020 6.57e-1 Pin1 ENSG00000127445 0.250 1.40e-8 0.571 9.56e-45 0.187 2.52e-5 MRE11 ENSG00000020922 0.063 1.56e-1 −0.007 8.81e-1 −0.024 5.93e-1 PML ENSG00000140464 0.072 1.05e-1 0.217 9.36e-7 0.166 1.85e-4 p63 ENSG00000073282 −0.120 7.04e-3 −0.283 1.08e-10 −0.198 7.71e-6 p73 ENSG00000078900 0.104 2.03e-2 0.258 4.67e-9 0.097 3.02e-2 Supplementary Table S2. -

TITLE PAGE Oxidative Stress and Response to Thymidylate Synthase
Downloaded from molpharm.aspetjournals.org at ASPET Journals on October 2, 2021 -Targeted -Targeted 1 , University of of , University SC K.W.B., South Columbia, (U.O., Carolina, This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. The final version may differ from this version. This article has not been copyedited and formatted. -

Review Article Molecular Chaperones of Leishmania: Central Players in Many Stress-Related and -Unrelated Physiological Processes
Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 301326, 21 pages http://dx.doi.org/10.1155/2015/301326 Review Article Molecular Chaperones of Leishmania: Central Players in Many Stress-Related and -Unrelated Physiological Processes Jose M. Requena,1 Ana M. Montalvo,2 and Jorge Fraga2 1 Centro de Biolog´ıa Molecular “Severo Ochoa” (CSIC-UAM), Universidad Autonoma´ de Madrid, 28049 Madrid, Spain 2Departamento de Parasitolog´ıa, Instituto de Medicina Tropical “Pedro Kour´ı”, 17100 Habana, Cuba Correspondence should be addressed to Jose M. Requena; [email protected] Received 7 March 2015; Accepted 24 May 2015 Academic Editor: Mehdi Chenik Copyright © 2015 Jose M. Requena et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Molecular chaperones are key components in the maintenance of cellular homeostasis and survival, not only during stress but also under optimal growth conditions. Folding of nascent polypeptides is supported by molecular chaperones, which avoid the formation of aggregates by preventing nonspecific interactions and aid, when necessary, the translocation of proteins to their correct intracellular localization. Furthermore, when proteins are damaged, molecular chaperones may also facilitate their refolding or, in the case of irreparable proteins, their removal by the protein degradation machinery of the cell. During their digenetic lifestyle, Leishmania parasites encounter and adapt to harsh environmental conditions, such as nutrient deficiency, hypoxia, oxidative stress, changing pH, and shifts in temperature; all these factors are potential triggers of cellular stress. We summarize here our current knowledge on the main types of molecular chaperones in Leishmania and their functions. -

Celastrol Increases Glucocerebrosidase Activity in Gaucher Disease by Modulating Molecular Chaperones
Celastrol increases glucocerebrosidase activity in Gaucher disease by modulating molecular chaperones Chunzhang Yanga,1, Cody L. Swallowsa, Chao Zhanga, Jie Lua, Hongbin Xiaob, Roscoe O. Bradya,1, and Zhengping Zhuanga,1 aSurgical Neurology Branch, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, MD 20892-1260; and bInstitute of Chinese Materia Medica, China Academy of Chinese Medical Sciences, Beijing 100700, China Contributed by Roscoe O. Brady, November 19, 2013 (sent for review October 21, 2013) Gaucher disease is caused by mutations in the glucosidase, beta, acid increased the catalytic activity of mutant GCase. Celastrol interfered gene that encodes glucocerebrosidase (GCase). Glucosidase, beta, with the recruitment of Cdc37 to Hsp90 halting the assembly of the acid mutations often cause protein misfolding and quantitative loss requisite chaperone complex. Inhibition of Hsp90 reduced its rec- of GCase. In the present study, we found that celastrol, an herb de- ognition of mutant GCase and therefore limited the proteasomal rivative with known anticancer, anti-inflammatory, and antioxidant degradation of the mutant protein. Additionally, celastrol triggered activity, significantly increased the quantity and catalytic activity of a reorganization of the gene expression pattern of molecular chap- GCase. Celastrol interfered with the establishment of the heat-shock erones such as DnaJ homolog subfamily B members 1 and 9 protein 90/Hsp90 cochaperone Cdc37/Hsp90-Hsp70-organizing pro- (DNAJB1/9), heat shock 70kDa proteins 1A and 1B (HSPA1A/B), tein chaperone complex with mutant GCase and reduced heat-shock and Bcl2-associated athanogene 3 (BAG3). The presence of BAG protein 90-associated protein degradation. In addition, celastrol mod- family molecular chaperone regulator 3 (BAG3) further stabi- ulated the expression of molecular chaperones. -

Estimation of Non-Null SNP Effect Size Distributions Enables the Detection
bioRxiv preprint doi: https://doi.org/10.1101/597484; this version posted May 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 1 Estimation of Non-null SNP Effect Size Distributions Enables 2 the Detection of Enriched Genes Underlying Complex Traits 3 1,2 1,2 2-4 4 Wei Cheng , Sohini Ramachandran y, and Lorin Crawford y 5 1 Department of Ecology and Evolutionary Biology, Brown University, Providence, RI, 6 USA 7 2 Center for Computational Molecular Biology, Brown University, Providence, RI, USA 8 3 Department of Biostatistics, Brown University, Providence, RI, USA 9 4 Center for Statistical Sciences, Brown University, Providence, RI, USA 10 Corresponding E-mail: [email protected]; lorin [email protected] y 11 Abstract 12 Traditional univariate genome-wide association studies generate false positives and negatives due to 13 difficulties distinguishing associated variants from variants with spurious nonzero effects that do not 14 directly influence the trait. Recent efforts have been directed at identifying genes or signaling pathways 15 enriched for mutations in quantitative traits or case-control studies, but these can be computationally 16 costly and hampered by strict model assumptions. Here, we present gene-", a new approach for identifying 17 statistical associations between sets of variants and quantitative traits. Our key insight is that enrichment 18 studies on the gene-level are improved when we reformulate the genome-wide SNP-level null hypothesis 19 to identify spurious small-to-intermediate SNP effects and classify them as non-causal.