The Filum Disease and the Neuro-Cranio-Vertebral Syndrome
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Saethre-Chotzen Syndrome
Saethre-Chotzen syndrome Authors: Professor L. Clauser1 and Doctor M. Galié Creation Date: June 2002 Update: July 2004 Scientific Editor: Professor Raoul CM. Hennekam 1Department of craniomaxillofacial surgery, St. Anna Hospital and University, Corso Giovecca, 203, 44100 Ferrara, Italy. [email protected] Abstract Keywords Disease name and synonyms Excluded diseases Definition Prevalence Management including treatment Etiology Diagnostic methods Genetic counseling Antenatal diagnosis Unresolved questions References Abstract Saethre-Chotzen Syndrome (SCS) is an inherited craniosynostotic condition, with both premature fusion of cranial sutures (craniostenosis) and limb abnormalities. The most common clinical features, present in more than a third of patients, consist of coronal synostosis, brachycephaly, low frontal hairline, facial asymmetry, hypertelorism, broad halluces, and clinodactyly. The estimated birth incidence is 1/25,000 to 1/50,000 but because the phenotype can be very mild, the entity is likely to be underdiagnosed. SCS is inherited as an autosomal dominant trait with a high penetrance and variable expression. The TWIST gene located at chromosome 7p21-p22, is responsible for SCS and encodes a transcription factor regulating head mesenchyme cell development during cranial tube formation. Some patients with an overlapping SCS phenotype have mutations in the FGFR3 (fibroblast growth factor receptor 3) gene; especially the Pro250Arg mutation in FGFR3 (Muenke syndrome) can resemble SCS to a great extent. Significant intrafamilial -

Oral Surgery Procedures in a Patient with Hajdu-Cheney Syndrome Treated with Denosumab—A Rare Case Report
International Journal of Environmental Research and Public Health Article Oral Surgery Procedures in a Patient with Hajdu-Cheney Syndrome Treated with Denosumab—A Rare Case Report Magdalena Kaczoruk-Wieremczuk 1,†, Paulina Adamska 1,† , Łukasz Jan Adamski 1, Piotr Wychowa ´nski 2 , Barbara Alicja Jereczek-Fossa 3,4 and Anna Starzy ´nska 1,* 1 Department of Oral Surgery, Medical University of Gda´nsk,7 D˛ebinkiStreet, 80-211 Gda´nsk,Poland; [email protected] (M.K.-W.); [email protected] (P.A.); [email protected] (Ł.J.A.) 2 Department of Oral Surgery, Medical University of Warsaw, 6 St. Binieckiego Street, 02-097 Warsaw, Poland; [email protected] 3 Department of Oncology and Hemato-Oncology, University of Milan, 7 Festa del Perdono Street, 20-112 Milan, Italy; [email protected] 4 Division of Radiotherapy, IEO European Institute of Oncology, IRCCS, 435 Ripamonti Street, 20-141 Milan, Italy * Correspondence: [email protected] † Co-first author, these authors contributed equally to this work. Abstract: Background: Hajdu-Cheney syndrome (HCS) is a very rare autosomal-dominant congenital disease associated with mutations in the NOTCH2 gene. This disorder affects the connective tissue and is characterized by severe bone resorption. Hajdu-Cheney syndrome most frequently affects Citation: Kaczoruk-Wieremczuk, M.; the head and feet bones (acroosteolysis). Case report: We present an extremely rare case of a 34- Adamska, P.; Adamski, Ł.J.; Wychowa´nski,P.; Jereczek-Fossa, year-old male with Hajdu-Cheney syndrome. The patient was admitted to the Department of Oral B.A.; Starzy´nska,A. Oral Surgery Surgery, Medical University of Gda´nsk,in order to perform the extraction of three teeth. -

Cervical Medullary Syndrome Secondary to Craniocervical
Neurosurgical Review https://doi.org/10.1007/s10143-018-01070-4 ORIGINAL ARTICLE Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization Fraser C. Henderson Sr1,2 & C. A. Francomano1 & M. Koby1 & K. Tuchman2 & J. Adcock3 & S. Patel4 Received: 10 October 2018 /Revised: 28 November 2018 /Accepted: 10 December 2018 # The Author(s) 2019 Abstract A great deal of literature has drawn attention to the Bcomplex Chiari,^ wherein the presence of instability or ventral brainstem compression prompts consideration for addressing both concerns at the time of surgery. This report addresses the clinical and radiological features and surgical outcomes in a consecutive series of subjects with hereditary connective tissue disorders (HCTD) and Chiari malformation. In 2011 and 2012, 22 consecutive patients with cervical medullary syndrome and geneticist-confirmed hereditary connective tissue disorder (HCTD), with Chiari malformation (type 1 or 0) and kyphotic clivo-axial angle (CXA) enrolled in the IRB-approved study (IRB# 10-036-06: GBMC). Two subjects were excluded on the basis of previous cranio-spinal fusion or unrelated medical issues. Symptoms, patient satisfaction, and work status were assessed by a third-party questionnaire, pain by visual analog scale (0–10/10), neurologic exams by neurosurgeon, function by Karnofsky performance scale (KPS). Pre- and post-operative radiological measurements of clivo-axial angle (CXA), the Grabb-Mapstone- Oakes measurement, and Harris measurements were made independently by neuroradiologist, with pre- and post-operative imaging (MRI and CT), 10/20 with weight-bearing, flexion, and extension MRI. -

Klippel Feil Syndrome: a Case Report
Chattogram Maa-O-Shishu Hospital Medical College Journal Volume 19, Issue 1, January 2020 Case Report Klippel Feil Syndrome: A Case Report Dhananjoy Das1* Abstract M A Chowdhury (Arzu)1 Klippel-Feil Syndrome (KFS) is a complex syndrome comprises of classical clinical S M Zafar Hossain1 triad of short neck, limitation of head and neck movements and low posterior hairline. This syndrome is resulting from failure of the normal segmentation of cervical vertebra. 1Autism and Child Development Centre & In this present case in addition to classical clinical triad we have found short stature, Child Neurology Unit scoliosis at cervico- dorsal junction and sprengel deformity of the shoulder. We Chattogram Maa Shishu-O-Shishu Hospital Medical College didn’t find any association of hearing impairment, congenital heart disease and Chattogram, Bangladesh. renal abnormalities. There was no any neurological deficit and normal school performance. Patient with KFS usually have good prognosis if cardiopulmonary, genitourinary, auditory problems are identified and treated early. Key words: Congenital; Fusion; Klippel-Feil syndrome; Cervical vertebrae. INTRODUCTION Klippel-Feil Syndrome (KFS) was first discovered by Maurice Klippel and Andre Feil in 19121. KFS is a complex syndrome comprises of classical clinical triad of short neck, limitation of head and neck movements (Especially lateral bending) and low posterior hairline2. In 50% cases have all three component of this syndrome. It occurs in 1 of every 42,000 births and 60% cases are Female2. KF syndrome is group of deformities that result due to failure of the normal segmentation and fusion processes of mesodermal somites, which occurs between the third and seventh week of embryonic life3,4. -
Neurocranial Defects with Neuro-Ophthalmic Significance
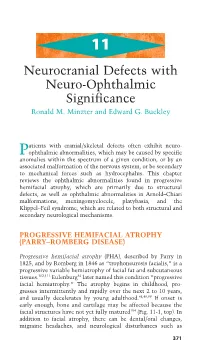
11 Neurocranial Defects with Neuro-Ophthalmic Significance Ronald M. Minzter and Edward G. Buckley atients with cranial/skeletal defects often exhibit neuro- Pophthalmic abnormalities, which may be caused by specific anomalies within the spectrum of a given condition, or by an associated malformation of the nervous system, or be secondary to mechanical forces such as hydrocephalus. This chapter reviews the ophthalmic abnormalities found in progressive hemifacial atrophy, which are primarily due to structural defects, as well as ophthalmic abnormalities in Arnold–Chiari malformations, meningomyelocele, platybasia, and the Klippel–Feil syndrome, which are related to both structural and secondary neurological mechanisms. PROGRESSIVE HEMIFACIAL ATROPHY (PARRY–ROMBERG DISEASE) Progressive hemifacial atrophy (PHA), described by Parry in 1825, and by Romberg in 1846 as “trophoneurosis facialis,” is a progressive variable hemiatrophy of facial fat and subcutaneous tissues.102,111 Eulenburg34 later named this condition “progressive facial hemiatrophy.” The atrophy begins in childhood, pro- gresses intermittently and rapidly over the next 2 to 10 years, and usually decelerates by young adulthood.48,49,99 If onset is early enough, bone and cartilage may be affected because the facial structures have not yet fully matured104 (Fig. 11-1, top). In addition to facial atrophy, there can be dental/oral changes, migraine headaches, and neurological disturbances such as 371 372 handbook of pediatric neuro-ophthalmology A B CD FIGURE 11-1A–D. Progressive nature of progressive hemifacial atrophy (PHA) in a patient at 8 years old (A) and again at 15 years (B), showing left-sided atrophy. Fundus photos of the normal contralateral side (C) and the ipsilateral affected side with hypopigmentary disturbances (D), par- ticularly along the inferior arcade. -

Part I, Cervical Spine
Open Access Review Article DOI: 10.7759/cureus.8667 Anatomical Variations That Can Lead to Spine Surgery at the Wrong Level: Part I, Cervical Spine Manan Shah 1 , Dia R. Halalmeh 2 , Aubin Sandio 1 , R. Shane Tubbs 3, 4, 5 , Marc D. Moisi 2 1. Neurosurgery, Wayne State University, Detroit Medical Center, Detroit, USA 2. Neurosurgery, Detroit Medical Center, Detroit, USA 3. Neurosurgery and Structural & Cellular Biology, Tulane University School of Medicine, New Orleans, USA 4. Anatomical Sciences, St. George's University, St. George's, GRD 5. Neurosurgery and Ochsner Neuroscience Institute, Ochsner Health System, New Orleans, USA Corresponding author: Dia R. Halalmeh, [email protected] Abstract Spine surgery at the wrong level is an adversity that many spine surgeons will encounter in their career, and it falls under the wrong-site surgery sentinel events reporting system. The cervical spine is the second most common location in the spine at which surgery is performed at the wrong level. Anatomical variations of the cervical spine are one of the most important incriminating risk factors. These anomalies include craniocervical junction abnormalities, cervical ribs, hemivertebrae, and block/fused vertebrae. In addition, patient characteristics, such as tumors, infection, previous cervical spine surgery, obesity, and osteoporosis, play an important role in the development of cervical surgery at the wrong level. These were described, and several effective techniques to prevent this error were provided. A thorough review of the English-language literature was performed in the database PubMed between 1981 and 2019 to review and summarize these risk factors. Compulsive attention to these factors is essential to ensure patient safety. -

Neurological Manifestations of Achondroplasia
Current Neurology and Neuroscience Reports (2019) 19:105 https://doi.org/10.1007/s11910-019-1008-x NEUROLOGY OF SYSTEMIC DISEASES (J BILLER, SECTION EDITOR) Neurological Manifestations of Achondroplasia John B. Bodensteiner1,2,3 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of review This review is to delineate the neurological complications seen in patients with achondroplasia. Recent findings As the understanding of the genetics of this disorder has advanced, the possibility of targets for intervention which might modify the development and management of the neurological complications of this disease may be identified. Summary Achondroplasia is a hereditary short-limbed dwarfism which has been known for millennia. The genetic defect is a gain of function sequence variation in the fibroblast growth factor receptor 3 (FGFR3). This gene normally regulates (inhibits) bone growth thus the gain of function results in abnormal or excessive inhibition of growth. The resulting bone is subject to distortion and the result is that bone impinges on nervous tissue, most commonly at the foramen magnum, spinal canal, and nerve root outlet foramen. Awareness of the range of these complications will, hopefully, allow early and more effective intervention so as to ameliorate the nature and severity of the long-term effects of the neurological complications in patients with achondroplasia. Keywords Achondroplasia . Spinal stenosis . Macrocephaly . Communicating hydrocephalus . Craniovertebral impingement . Claudication Introduction impact of the interplay between the skeletal abnormalities and the underlying nervous system on functions including respi- Achondroplasia is the most completely delineated of the ration and sleep in addition to the more widely recognized short-limbed dwarfing conditions. -

Identification of Clinical and Radiographic Predictors of Central
www.nature.com/scientificreports OPEN Identifcation of clinical and radiographic predictors of central nervous system injury in genetic skeletal disorders Antônio L Cunha Jr1*, Ana P S Champs1, Carla M. Mello1, Mônica M. M. Navarro1, Frederico J. C. Godinho1, Cássia M. B. Carvalho1 & Teresa C. A. Ferrari2 Some studies report neurological lesions in patients with genetic skeletal disorders (GSDs). However, none of them describe the frequency of neurological lesions in a large sample of patients or investigate the associations between clinical and/or radiological central nervous system (CNS) injury and clinical, anthropometric and imaging parameters. The project was approved by the institution’s ethics committee (CAAE 49433215.5.0000.0022). In this cross-sectional observational analysis study, 272 patients aged four or more years with clinically and radiologically confrmed GSDs were prospectively included. Genetic testing confrmed the diagnosis in the FGFR3 chondrodysplasias group. All patients underwent blinded and independent clinical, anthropometric and neuroaxis imaging evaluations. Information on the presence of headache, neuropsychomotor development (NPMD), low back pain, joint deformity, ligament laxity and lower limb discrepancy was collected. Imaging abnormalities of the axial skeleton and CNS were investigated by whole spine digital radiography, craniocervical junction CT and brain and spine MRI. The diagnostic criteria for CNS injury were abnormal clinical and/or radiographic examination of the CNS. Brain injury included malacia, encephalopathies and malformation. Spinal cord injury included malacia, hydrosyringomyelia and spinal cord injury without radiographic abnormalities. CNS injury was diagnosed in more than 25% of GSD patients. Spinal cord injury was found in 21.7% of patients, and brain injury was found in 5.9%. -

The 22Q11.2 Deletion Syndrome As a Model for Idiopathic Scoliosis
UITNODIGING Uitnodiging voor het bijwonen The 22q11.2 Deletion Syndrome van de openbare verdediging van as a Model for Idiopathic Scoliosis mijn proefschrift The 22q11.2 Deletion Syndrome Deletion The 22q11.2 The 22q11.2 Deletion Syndrome as a Model for Idiopathic Scoliosis J.F. Homans as a Model for Idiopathic Scoliosis Jelle F. Homans, 2020 Donderdag 23 januari 2020 16.15 uur Academiegebouw Domplein 29 Utrecht Aansluitend zal een receptie plaatsvinden. U bent van harte uitgenodigd! Paranimfen: Rob Brink Cor Homans [email protected] Jelle Homans [email protected] Jelle F. Homans The 22q11.2 Deletion Syndrome as a Model for Idiopathic Scoliosis Jelle Frederik Homans Colofon © 2020 Jelle F. Homans. All rights reserved. No part of this book may be reproduced or transmitted in any form or by any means, whitout prior written permission of the author. The research in this thesis was financially supported by: K2M research grant - Scoliosis Research Society. The reproduction of this thesis was supported by: Dutch Spine Society - Nederlandse Orthopaedische Vereniging - Castor EDC - Chipsoft - InSpine Netherlands B.V. - Loopvisie B.V. - Sectra Benelux ISBN: 978-94-6380-672-5 Layout: Fenna Schaap Printed by: Proefschriftmaken.nl The 22q11.2 Deletion Syndrome as a Model for Idiopathic Scoliosis Het 22q11.2 Deletie Syndroom als Model voor Idiopathische Scoliose (met een samenvatting in het Nederlands) Proefschrift ter verkrijging van de graad van doctor aan de Universiteit Utrecht op gezag van de rector magnificus, prof.dr. H.R.B.M. Kummeling, ingevolge het besluit van het college voor promoties in het openbaar te verdedigen op donderdag 23 januari 2020 des middags te 4.15 uur door Jelle Frederik Homans geboren op 11 mei 1989 te Hengelo Promotoren: Prof. -

Cover and Comments 23-2
BARROW QUARTERLY VOLUME 23 ◊ NUMBER 2 ◊ 2007 BARROW NEUROLOGICAL INSTITUTE OF ST. JOSEPH’S HOSPITAL AND MEDICAL CENTER • PHOENIX, ARIZONA Copyright © 2006, Barrow CRANIOFACIAL SURGERY Copyright © 2007, Barrow Neurological Institute COMMENTS No single discipline has the expertise to fully treat children with a craniofacial anomaly. Consequently, such children require care from many different disciplines. Typically, surgical, medical, dental, and psy- chosocial specialists are involved. When a large number of professionals are involved in the multifaceted care of patients, healthcare teams develop. Cleft and craniofacial teams, which were formed in response to the complex, life-long, ongoing clinical and psychosocial needs of this patient population, are widely considered an effective means to avoid fragmentation and dehumanization in the delivery of such highly specialized health care. Team care represents an improvement over splintered, community-based, multispecialty care. The benefits of healthcare delivery by the team approach include the abilities to provide interdisciplinary ser- vices, to address the emotional and psychological needs of patients and their family, and to perform mul- tifaceted examinations that enable comprehensive treatment plans to be formed based on the team’s rec- ommendations and the family’s preferences. Since 1986 the Barrow Craniofacial Center (formerly the Southwest Craniofacial Center) has been treating children and adults with cleft and craniofacial disorders from Arizona and the Southwest through this essential interdisciplinary team approach. The team helps address parental concerns about the choice and timing of treatment and the coordination of ongoing care. In addition to providing these clinical craniofacial services, the team conducts clinical research and provides education for students of these dis- ciplines. -

Nasopharyngeal Dysmorphology in the Syndromes of Apert and Crouzon SALLY J. PETERSON-FALZONE, Ph.D. SAMUEL PRUZANSKY, D.D.S., M
Nasopharyngeal Dysmorphology In The Syndromes of Apert and Crouzon SALLY J. PETERSON-FALZONE, Ph.D. SAMUEL PRUZANSKY, D.D.S., M.S. PAMELA J. PARRIS, M.S. JOANNE L. LAFFER, M.S. Chicago, Illinors 60680 Serial cephalometric studies on 29 patients with Apert syndrome and 26 patients with Crouzon disease confirmed and expanded previously reported observations of dysmor- phology of the nasopharynx and contiguous structures. Particularly remarkable were alterations in pharyngeal depth, pharyngeal height, length of the posterior cranial base, and length of the hard and soft palate. The distortions and displacements contributing to diminition of the nasopharyngeal space were typically present early in life and became more severe as the patient matured. Implications for care and treatment planning are discussed. KEY WORDS: Cephalometrics, Apert syndrome, Crouzon disease, nasopharynx In 1974, the current authors reported on tine processes. Peterson and Pruzansky (1974) palatal anomalies in a series of 19 patients found these accumulations to occur in both with Apert syndrome and 13 patients with Apert and Crouzon patients but to be more Crouzon disease. The focus of that report was consistent in occurrence and more severe in twofold: (a) a detailed description of the the former. No relationship was found be- anomalous configuration of the maxillary tween presence of either a bifid uvula or an arch and palatal vault, both of which had overt cleft palate and either the abnormal size been at least partially described by previous of the soft palate or the aberrant configuration investigators but only in Apert patients of the palatal vault, which creates the image (Blank, 1960; Buchanan, 1968; Buckley and of a pseudo-cleft. -

Spine Radiograph in Dysplasias: a Pictorial Essay
Published online: 2021-07-14 MUSCULOSKELETAL IMAGING Spine radiograph in dysplasias: A pictorial essay Pavan Gabra, Manisha Jana, Priyanka Naranje, Neerja Gupta1, Madhulika Kabra1, Arun K Gupta, Richa Yadav Departments of Radiodiagnosis and 1Paediatrics (Division of Genetics), All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India Correspondence: Dr. Manisha Jana, Department of Radiodiagnosis, All India Institute of Medical Sciences, Ansari Nagar, New Delhi ‑ 110 029, India. E‑mail: [email protected] Abstract Spine radiograph is an essential component of a skeletal survey. It provides important diagnostic clues to various types of skeletal dysplasia. In some conditions, a spine radiograph alone may be diagnostic and characteristic; but mostly, it yields more value as a part of the complete skeletal survey. In this article we will discuss about a few common lethal and non‑lethal skeletal dysplasias and their characteristic imaging findings; primarily focusing on the spine radiograph. Key words: Achondroplasia; mucopolysaccharidosis; radiograph; skeletal dysplasia; spine Introduction They appear in the upper cervical, cervicothoracic and thoracolumbar locations. All three ossification centers are The vertebral column is composed of vertebrae and present by the 5th month of intrauterine life.[1] surrounding ligaments. The dorsolumbar spine (AP and lateral views) radiographs are an essential part Normal Appearance in Different Age Group of any skeletal survey done to look for skeletal dysplasias. The rapidly evolving pediatric body makes the knowledge At birth, the centra are united with the neural arches by a of normal imaging appearance of pediatric spine across the synchondrosis. The arches unite with the vertebral bodies temporal spectrum an indispensable tool to look for any beginning in the first year of life, with the upper lumbar abnormality.