Accelerating the Performance of District Health Systems Towards Achieving UHC Via Twinning Partnerships
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

National Situation Analysis of Children and Women in Ethiopia
Ministry of Finance For every child Whoever she is. Wherever he lives. Every child deserves a childhood. A future. A fair chance. That’s why UNICEF is there. For each and every child. Working day in and day out. In more than 190 countries and territories. Reaching the hardest to reach. The furthest from help. The most excluded. It’s why we stay to the end. And never give up. National Situation Analysis of Children and Women in Ethiopia Cover photo © UNICEF Ethiopia/2017/Martha Tadesse Ministry of Finance Ministry of Finance The United Nations Children’s Fund P.O.Box: 1037 Or 1905, Addis Ababa, Ethiopia P.O.Box 1169, Addis Ababa, Ethiopia Email: [email protected] Email: [email protected] Telephone: +251 11 155 2015 Telephone: +251 11 518 4000 Fax: +251 11 155 5189 Fax: +251 11 551 1628 Website: www.mofed.gov.et Website: www.unicef.org/ethiopia Ministry of Finance National Situation Analysis of Children and Women in Ethiopia National Situation Analysis of Children and Women in Ethiopia FOREWORD The Federal Democratic Republic of Ethiopia is on the cusp of transformational changes that could ii solidify its place as a leader on the African continent and an important actor in the global landscape. As the second most-populous country in Africa, and a country that has demonstrated resilience in the face of recurrent hazards, Ethiopia can be a country model for inclusive development that is sustainable, equity-focused and risk-informed. In pursuit of the Sustainable Development Goals of the United Nations Agenda 2030, the African Union’s Agenda 2063 and Ethiopia’s own current national development agenda, the Second Five- Year Growth and Transformation Plan 2015/2016-2019/2020 (GTP II), there must be broad-scale commitment across country stakeholders to leave no one behind. -

Adoption of Agricultural Technologies and Risk in a Peasant Economy
Munich Personal RePEc Archive Strategic Decision-Making: Adoption of Agricultural Technologies and Risk in a Peasant Economy Mariam, Yohannes and Galaty, John and Coffin, Garth 12 June 1993 Online at https://mpra.ub.uni-muenchen.de/387/ MPRA Paper No. 387, posted 11 Oct 2006 UTC Strategic Decision-Making: Adoption of Agricultural Technologies and Risk in a Peasant Economy Yohannes Kebede (also known Yohannes Mariam) 1/, John Galaty2/, Garth Coffin3/ 1/ Washington Utilities and Transportation Commission, Olympia, WA, 2/ Professor, McGill University, Department of Anthropology, McGill University, Montreal, Quebec, CA 3/ Formerly Associate Professor and Associate Dean, Faculty of Agricultural and Environmental Sciences, McGill University Acknowledgement: This paper is based on the principal author’s doctoral dissertation completed at McGill University in 1993.The financial support of the Rockefeller Foundation (African dissertation internship award), International Development Research Center, and McGill University, and technical support provided by the International Livestock Center for Africa (ILCA) for field work in Ethiopia is highly appreciated. Abstract Descriptive and logit analysis were employed to investigate the impact of social, economic and technical factors on decisions to adopt new agricultural technologies in the Ada and Selale districts of Ethiopia. Peasants follow sequential adoption of technologies. In both study areas, priority is given to adoption of crop production augmenting technologies followed by technologies that complement crop production (Ada) and contribute to increases in milk production (Selale). Producers of both regions require existence of certain pre-conditions prior to the adoption of technologies. Ada farmers require more pre-conditions related to livestock production while Selale farmers require more preconditions related crop production. -

Sustainable Land Management Ethiopia
www.ipms-ethiopia.org www.eap.gov.et Working Paper No. 21 Sustainable land management through market-oriented commodity development: Case studies from Ethiopia This working paper series has been established to share knowledge generated through Improving Productivity and Market Success (IPMS) of Ethiopian Farmers project with members of the research and development community in Ethiopia and beyond. IPMS is a five-year project funded by the Canadian International Development Agency (CIDA) and implemented by the International Livestock Research Institute (ILRI) on behalf of the Ethiopian Ministry of Agriculture and Rural Development (MoARD). Following the Government of Ethiopia’s rural development and food security strategy, the IPMS project aims at contributing to market-oriented agricultural progress, as a means for achieving improved and sustainable livelihoods for the rural population. The project will contribute to this long-term goal by strengthening the effectiveness of the Government’s efforts to transform agricultural production and productivity, and rural development in Ethiopia. IPMS employs an innovation system approach (ISA) as a guiding principle in its research and development activities. Within the context of a market-oriented agricultural development, this means bringing together the various public and private actors in the agricultural sector including producers, research, extension, education, agri-businesses, and service providers such as input suppliers and credit institutions. The objective is to increase access to relevant knowledge from multiple sources and use it for socio-economic progress. To enable this, the project is building innovative capacity of public and private partners in the process of planning, implementing and monitoring commodity-based research and development programs. -
Agroforestry: an Attractive REDD+ Policy Option?
AGROFORESTRY – TEEBAGRIFOOD [Exploratory Study] Agroforestry: an attractive REDD+ policy option? worldagroforestry.org unep-wcmc.org un-redd.org teebweb.org Agroforestry: an attractive REDD+ policy option? Authors ICRAF: Sara Namirembe, Scott McFatridge, Lalisa Duguma, Florence Bernard, Peter Minag UNEP WCMC: Marieke Sassen, Arnout van Soersbergen, Eyerusalem Akalu Edited by: Salman Hussain (UNEP TEEB), Kavita Sharma (UNEP TEEB) and Ivo Mulder (UNEP) Disclaimer The contents of this report do not necessarily reflect the views or policies of UNEP, contributory organisations or editors. The designations employed and the presentations of material in this report do not imply the expression of any opinion whatsoever on the part of UNEP or contributory organisations, editors or publishers concerning the mention of a commercial entity or product, the legal status of any country, territory, city area or its authorities, or concerning the delimitation or designation of its frontiers or boundaries or the designation of its name, frontiers or boundaries. October 2015 2 TABLE OF CONTENTS SUMMARY……………………………………………………………………………………………………………………………………… 8 1. Introduction ............................................................................................................................................................... 23 1.1. Selection of case studies…………………………………………………………………………………………………………..…..24 2. Methods for Ecosystem Services Quatification, Valuation & Scenarios Analysis ... 24 2.1. Information acquisition and management .................................................................................................................... -

Girma Gebresenbet
Curriculum Vitae Girma Gebresenbet Girma Gebresenbet is a Professor, head of Logistics and Transport Division (www.slu.se/logistik), at the Swedish University of Agricultural Sciences, Department of Energy and Technology. His MSc degree is in Mechanical Engineering and obtained honour degree, and for his PhD degree he obtained a special reward from the Swedish Academy of Forestry and Agriculture for the outstanding doctoral dissertation of the year. Currently, Gebresenbet is coordinating and managing many national and international research projects, where researchers and industry partners participated from many countries, mainly in the subject area of Logistics and Supply Chain Management with specific emphasis on Food Production and Marketing Chain in relation to quality, safety (including animal welfare), security, and environment. Name Girma Gebresenbet Citizenship Swedish Gender Male Residence adress: Girma Gebresenbet Intagsgränd 47 163 41 Spånga Sweden Tel +46 8 7615084 Office address: Girma Gebresenbet Department of Energy and Technology, Swedish University of Agricultural Sciences Box 7032, 750 07 Uppsala, Sweden Tel: +46 18 671901 E- mail: [email protected] 1 Language Read Write Speak Excel Good Fair Slight Excel Good Fair Slight Excel Good Fair Slight lent lent lent English x x x Swedish x x x Russian x x x French x x x Oromo* x x x Amharic* x x x * Ethiopian languages Education 1973 - 1974 Flying school of Ethiopian Air force 1974 - 1975 Addis Ababa University, Ethiopia 1977 - 1983 Master of Science in Engineering, -

Somali and Benishangul-Gumuz Regions Adegehe, A.K
Federalism and ethnic conflict in Ethiopia. A comparative study of the Somali and Benishangul-Gumuz regions Adegehe, A.K. Citation Adegehe, A. K. (2009, June 11). Federalism and ethnic conflict in Ethiopia. A comparative study of the Somali and Benishangul-Gumuz regions. Retrieved from https://hdl.handle.net/1887/13839 Version: Not Applicable (or Unknown) Licence agreement concerning inclusion of doctoral thesis in the License: Institutional Repository of the University of Leiden Downloaded from: https://hdl.handle.net/1887/13839 Note: To cite this publication please use the final published version (if applicable). Peripherality, Ethnic Makeup 5 and History: Somali and Benishangul-Gumuz Regions 5.1 Introduction The previous chapter examined the asymmetrical features of Ethiopian federalism and provided an outline about emerging trends of autonomy conflicts at the country level. The task of this chapter is, however, to provide a general background on the two study regions – Somali and Benishangul-Gumuz. Both regions share a number of similarities. For instance, they were historically peripheral to the Ethiopian State and hence their constituent ethnic groups have little presence in the national political landscape. They also suffered from chronic marginality in terms of social and physical infrastructure development. Indeed, in spite of some of the positive changes since 1992, the two regions still lag significantly behind the highland regions. Besides peripherality, both regions have cross-border ethnic ties. In fact, the international boundaries that Ethiopia shares with the Sudan and Somalia divide the ethnic groups of the two regions. There is, however, some variance in the significance of the ethnic groups to the politics of the neighbouring countries. -

Uses of Wild Edible Plants in Quara District, Northwest Ethiopia
Tebkew et al. Agric & Food Secur (2018) 7:12 https://doi.org/10.1186/s40066-018-0163-7 Agriculture & Food Security RESEARCH Open Access Uses of wild edible plants in Quara district, northwest Ethiopia: implication for forest management Mekuanent Tebkew*, Yohannis Gebremariam, Tadesse Mucheye, Asmamaw Alemu, Amsalu Abich and Dagim Fikir Abstract Background: Wild edible plants are of crucial importance in all parts of the world in supporting global food basket (about one billion people) on a daily basis. They are means of survival for rural communities, especially during times of drought, famine, shocks and risks. This study assessed wild edible plants, uses, management practices and their threats in Quara district. It further investigates the implication of wild edible plants utilization for forest management. Methods: Structured and semi-structured questionnaire interview, focus group discussion, rapid market survey and informants guided fled walks were used to collect data in three purposively selected administrative Kebeles. A total of ninety-four randomly selected sample households were interviewed for data collection. Both quantitative and qualita- tive data analyses were made. Descriptive and regression analysis were made to analyze the data using SPSS version 16.0. Results: The area harbors a total of 36 wild edible plants. In addition to food values, these plants provide diverse benefts to the local community including income, fuel wood, fencing, construction, medicine and fodder. Adansonia digitata L., Ziziphus spina-christi Willd, Ximenia Americana L., Tamarindus indica L. and Balanites aegyptiaca L. were highly cited species by respondents. WEPs were threatened by anthropogenic factors including fre, agricultural expansion, deforestation, free grazing, fuel wood and construction. -

Living Documents Tropical Forest Portfolio ‘Land Is Given by God’ Conserving the Roof of Africa Bale Mountains National Park, Ethiopia
EthiopiaDef 20-11-2000 11:29 Pagina 1 DGIS-WWF Living Documents Tropical Forest Portfolio ‘Land is Given by God’ Conserving the Roof of Africa Bale Mountains National Park, Ethiopia • A frozen wilderness • Save the wild Arabica! • The lonely Ethiopian Wolf • A situation rapidly getting out of control • 'It's this thing they call democracy' More than three-quarters of all African land above 3,000m is to be found in Ethiopia.The Bale Mountains lie at the heart of this unique Afro-alpine landscape.The home of wild coffee plants and of the endangered Ethiopian Wolf, it is also an area of ever-increasing settlements, cultivation and large- scale cattle grazing.Winning the hearts of local people is the challenge for the Bale Mountains conservation project. EthiopiaDef 20-11-2000 11:29 Pagina 2 LIVING DOCUMENTS DGIS-WWF Tropical Forest Portfolio ‘What we actually do is crisis management’ Asked whether Ethiopia’s protected areas will ever suffers from inadequate and demoralised staff, but become exclusion zones, where only tourists and scientists also the continued lack of road and buildings can go, Tesfaye Hundessa’s answer is maintenance. As yet, the Park has not even been gazetted. resolutely negative: ‘Forget it.’ ‘What we actually do is crisis management’, admits Hundessa without hesitation. ‘That’s really all n the eyes of Hundessa, who is the General we can do for the moment. The lack of funding I Manager of the Federal Ethiopian Wildlife means there is no way we can work towards a Conservation Organisation (EWCO), the whole idea structural build-up of capacity in parks like Bale of recreating a kind of pristine situation is nothing Mountains. -

Utilization of Institutional Delivery Service and Associated Factors Among Mothers in North West Ethiopian Solomon Weldemariam1*, Amare Kiros2 and Mengistu Welday1
Weldemariam et al. BMC Res Notes (2018) 11:194 https://doi.org/10.1186/s13104-018-3295-8 BMC Research Notes RESEARCH NOTE Open Access Utilization of institutional delivery service and associated factors among mothers in North West Ethiopian Solomon Weldemariam1*, Amare Kiros2 and Mengistu Welday1 Abstract Objective: The aim of this study was to assess institutional delivery and its associated factors in Benishangul-Gumez region, North-West of Ethiopia. The data were obtained at community level in a single survey within 1 month and there is no continuation of this study or previously published part elsewhere. Results: Among the 428 eligible respondents recruited for this study, 427 of them responded completely to the interview, giving a response rate of 99.8%. Of the total (427) respondents, 51.1% women delivered the recent child at health facility in the 12 months preceding the survey. Among the common reasons for home delivery were, labour was urgent (25.8%), home birth was usual habit for them (23.9%) and distance to health center was too far. Age (AOR 3.4, 95% CI 1.46, 7.97), husband occupation (AOR 5.16, 95% CI 1.74, 15.31), frequency of antenatal care visit (AOR = 3.34, 95% CI 1.88, 5.94) and maternal knowledge on= danger signs of pregnancy and delivery (AOR 7.18, 95% CI 3.77,= 13.66) were signifcantly associated factors with institutional delivery. Although, the prevalence of =institutional delivery has improved when compared to previous reports, strategic modifcation is important to increase health facility delivery. Keywords: Institutional delivery, Associated factors, Benishangul-Gumez, Ethiopia Introduction most SSA women still give birth at home in the absence Globally, the total number of maternal deaths decreased of skilled birth attendant (SBA) [4]. -

Beekeepingpractices in Four Districts of Tigray Region, Northern Ethiopia
Nigerian J. Anim. Sci. 2018, 20 (1): 1-10 Beekeeping practices in four districts of tigray region, northern Ethiopia Gebregiorgis A. G., Berihu G., Tsegay T. G., Niraj K.* and Abrha B. H. College of Veterinary Medicine, Mekelle University, Mekelle, Ethiopia *Corresponding Author: [email protected] Target audience: Ministry of Agriculture, Researchers, Apiculture Professionals Abstract A survey was carried out on beekeeping practices in four districts (Degua-Timben, Hawzen, Saesiea- Tsaeda-Emba and Atsib-Wemberta) of Tigray Region, Northern Ethiopia. Data were obtained from 164 beekeepers by using pre-tested, structured questionnaire on demographic characteristics and honey production practices. Beekeeping was dominated by male (91.46%). Higher proportion (56.71%) of the respondents used traditional hive, while 22.56% worked with modern hive only and 20.73% were practicing both. The overall average number of traditional and modern hives per respondent in the study area was 7.45 and 3.20, respectively. Majority (76.22%) of the respondents practiced supplementary feeding of bee colonies, with 72.56% who fed bees in March to May. Annual honey production per traditional hive was significantly (p<0.05) higher in Saesiea-Tsaeda-Emba (11.42±1.77 kg), Atsib- Wemberta (10.55±0.84 kg) and Hawzen (10.15±1.36 kg) than what was realized in Degua-Timben (7.88±1.40 kg), while honey production per modern hive was significantly (p<0.05) higher in Atsib- Wemberta (35.33±2.20 kg) and Hawzen (33.05±1.94 kg) districts than what was realized in Saesiea- Tsaeda-Emba (23.22±1.81 kg). -
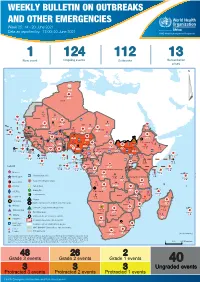
Weekly Bulletin on Outbreaks
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 25: 14 - 20 June 2021 Data as reported by: 17:00; 20 June 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 124 112 13 New event Ongoing events Outbreaks Humanitarian crises 64 0 135 928 3 631 Algeria ¤ 36 13 936 0 6 045 181 Mauritania 14 381 524 48 0 110 0 42 404 1 158 Niger 20 336 481 5 362 19 Mali 21 0 9 0 Cape Verde 6 471 16 4 946 174 Chad Eritrea Senegal 5 469 193 Gambia 3 0 66 0 32 002 283 1 414 8 Guinea-Bissau 847 17 Burkina Faso 236 49 275 194 4 283 167 155 2 117 Guinea 13 469 167 13 0 3 825 69 1 1 30 0 Benin 198 0 Nigeria 1 063 4 6 0 1 0 Ethiopia 13 2 6 995 50 556 5 872 15 Sierra Leone Togo 530 0 80 090 1 310 Ghana 7 139 98 Côte d'Ivoire 10 786 115 19 000 304 68 0 South Sudan 45 0 Liberia 199 2 17 0 Central African Republic 1 308 2 0 25 0 50 14 0 6 738 221 Cameroon 23 450 289 3 0 48 044 308 94 913 793 34 135 194 7 0 56 0 1 347 30 3 1 620 1 178 078 3 437 2 0 168 0 4 816 82 13 721 128 2 0 8 698 120 Equatorial Guinea Uganda 356 0 822 9 Sao Tome and Principe 4 0 2 995 95 71 543 660 Kenya Gabon Legend Congo 2 682 83 305 26 Rwanda 8 140 103 2 362 37 30 048 378 24 736 156 Democratic Republic of the Congo 12 298 161 Burundi Measles 5 242 8 Seychelles 37 809 879 427 0 Humanitarian crisis 536 32 Monkeypox United Republic of Tanzania 197 0 14 549 52 Suspected Drancuculiasis Lassa fever 509 21 63 1 6 257 229 Cholera Yellow fever 37 678 859 129 003 1 644 Comoros Meningitis 304 3 cVDPV2 Angola Malawi Leishmaniasis 34 868 1 168 726 0 3 908 146 Zambia 133 0 COVID-19 Mozambique -

Ethiopian Evangelical Church Mekane Yesus - Development and Social Services Commission (EECMY –DASSC)
SECRETARIAT - 150 route de Ferney, P.O. Box 2100, 1211 Geneva 2, Switzerland - TEL: +41 22 791 6033 - FAX: +41 22 791 6506 www.actalliance.org Appeal Ethiopia Drought Response - ETH111, Revision 3 Appeal Target: US$7,621,198 Balance Requested US$2,220,641 Geneva, 10 July, 2012 Dear Colleagues, The ACT Alliance Ethiopia forum has found it necessary to revise the current appeal to include drought rehabilitation activities and to prioritise activities based on the funding received to date. This revised appeal replaces the previous one issued on October 6th 2011, ETHrev2. New and revised parts of the document are highlighted in green colour. Pre ETH111: The worst drought in 60 years hit the Horn of Africa, affecting more than 12.4 million people according to UN OCHA. In Ethiopia, some 4.8 million needed immediate support to meet their daily food requirements. In addition, approximately 120,000 people from Somalia crossed the border to Ethiopia and are currently living in crowded and under-resourced refugee camps in Dollo Odo. Recent conflict in Sudan has also resulted to more than 25,000 refugees crossing the border seeking refuge in Ethiopia. The prolonged La Nina conditions in Ethiopia affected a second consecutive rain season resulting in drought. Following a complete failure of the 2010 October‐December rains and related harvests, the 2011 March‐May rains began late and were erratic. This led to the current drought, which is considered the worst in thirty years. The drought is characterised by substantial harvest failure, decrease in water availability, deteriorating pasture conditions and livestock losses in the southern, south-eastern pastoral and agro-pastoral parts of the country, including major bulgar cropping areas of Amhara, Oromia, SNNPR and Tigray.