Access to Medicine Index
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
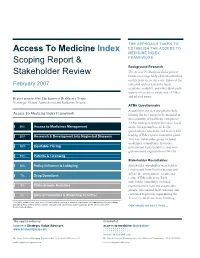
Access to Medicine Index Scoping Report & Stakeholder Review
THE APPROACH TAKEN TO Access To Medicine Index ESTABLISH THE ACCESS TO MEDICINE INDEX Scoping Report & FRAMEWORK Background Research The Access To Medicine Index project Stakeholder Review builds on a large body of work published on this issue in recent years. Innovest has February 2007 collected and reviewed the latest academic, industry, and other third-party reports on access to medicines (ATMs) and related issues. Report prepared by The Innovest Healthcare Team: Veronique Menou, Adam Savitz and Katharine Preston. ATMs Questionnaire A questionnaire was designed to help Access To Medicine Index Framework identify the key issues to be included in an evaluation of healthcare companies’ ATMs strategies and performance based 20% Access to Medicines Management on the background research. The questionnaire was delivered to over 200 20% Research & Development into Neglected Diseases leading ATMs experts around the globe. This key stakeholder group included academics, consultants, investors, 18% Equitable Pricing government representatives, and non- governmental organizations (NGOs). 15% Patents & Licensing Stakeholder Roundtables 10% Policy Influence & Lobbying Stakeholder roundtables were held in London and New York to discuss and debate the questionnaire results and 7% Drug Donations refine ATMs indicators. Each stakeholder roundtable included 5% Philanthropic Activities representatives from the stakeholder groups, who shared their expertise and 5% Ethical Promotion & Marketing Activities continued to provide input during the Access To Medicine Index building This table includes the eight most relevant criteria, ranked in order of importance, as indicated by the percentage weighting. This criteria will be used to evaluate each pharmaceutical company’s performance during the CONTINUED ON NEXT PAGE… benchmarking phase. -

2020 Health for Humanity Report
2020 Health for Humanity Report Progress in Sustainability Contents | Message from Our CEO | Our Approach | United in Defeating COVID-19 | Better Health for All | Responsible Business Practices | Reporting Hub Contents Message from Our Chairman and CEO 3 2020 Year in Brief 4 Our Recognitions 5 Our Approach 6 Health for Humanity Strategy & Goals 9 Sustainability Governance 13 Sustainability Priorities 14 United in Defeating COVID-19 15 Caring for Patients 17 Supporting the Front Lines of Care 24 Protecting Employees 25 Supply Chain Resilience 28 Better Health for All 30 Innovation 31 Global Public Health Strategy 35 Access & Affordability 45 Strengthening Health Systems 48 Responsible Business Practices 52 Ethics & Values 53 Our People 60 Product Quality & Safety 74 Environmental Health 79 Responsible Supply Base 90 ABOVE: During the COVID-19 pandemic, Report overview community healthcare workers in Peru Reporting Hub 98 This Report details the progress of the Johnson & Johnson Family traveled door-to-door to reach children with ESG Summary 98 of Companies in sustainability. It is also our primary source of VERMOX Chewable tablets for treatment of Performance Data 98 annual disclosure on environmental, social and governance intestinal worms. The medicine is donated GRI Content Index 98 (ESG) performance and should be reviewed in conjunction by Johnson & Johnson and implemented GRI Culture of Health for Business Framework 98 with disclosures on the ESG Policies & Positions page. Data by INMED Partnerships for Children. SASB Index 98 in this Report cover the period between January 1, 2020, and Photo by INMED Partnerships for Children. TCFD 98 December 31, 2020, unless otherwise noted. -

Antiretroviral Price Reductions
UNTANGLING THE WEB OF ANTIRETROVIRAL PRICE REDUCTIONS 18th Edition – July 2016 www.msfaccess.org PREFACE In this report, we provide an update on the key facets of HIV treatment access. It includes the latest HIV treatment guidelines from World Health Organization (WHO), an overview on pricing for first-line, second-line and salvage regimens, and a summary of the opportunities for – and threats to – expanding access to affordable antiretroviral therapy (ART). There is a table with information on ARVs, including quality assurance, manufacturers and pricing on pages 55 to 57. THE MSF ACCESS CAMPAIGN In 1999, on the heels of Médecins Sans Frontières (MSF) being awarded the Nobel Peace Prize – and largely in response to the inequalities surrounding access to HIV/AIDS treatment between rich and poor countries – MSF launched the Campaign for Access to Essential Medicines. Its sole purpose has been to push for access to, and the development of, life-saving and life-prolonging medicines, diagnostics and vaccines for patients in MSF programmes and beyond. www.msfaccess.org MSF AND HIV Médecins Sans Frontières (MSF) began providing antiretroviral therapy to a small number of people living with HIV/AIDS in 2000 in projects in Thailand, South Africa and Cameroon. At the time, treatment for one person for one year cost more than US$10,000. With increased availability of low-cost, quality antiretroviral drugs (ARVs), MSF provides antiretroviral treatment to 240,100 people in 18 countries, implements treatment strategies to reach more people earlier in their disease progression, and places people living with HIV at the centre of their care. -

A Balanced Trade Context for HIV Patent Pool
iMedPub Journals 2011 TRANSLATIONAL BIOMEDICINE Vol. 2 No. 1:3 This article is available from: http://www.transbiomedicine.com doi: 10:3823/420 A Balanced Trade Context for HIV Patent Pool Daniele Dionisio, M.D. Member, European Parliament Working Group on Innovation, Access to Medicines and Poverty- Related Diseases. Reference Advisor for “Drugs for the developing countries”, SIMIT (Italian Abstract Society for Infectious and Tropical Diseases). Former Director, Infectious Disease Division, Pistoia city Hospital (Italy). Background: Reluctance of the multinational pharmaceutical companies to join the Medicines Patent Pool plan for HIV drugs (antiretrovirals-ARVs) might undermine E-mail: [email protected] its desirable objective of scaling up long-term, extended access to novel, affordable and appropriate ARV formulations in resource-limited settings. Methods: This paper makes an analysis of conflicting issues and calls for a trade context facilitating a reverse of multinational drug manufacturers’ reluctance to join patent pool. To this aim, partnerships between multinational companies are urged first to make cutting edge brand fixed-dose combination (FDC) ARVs promptly avail- able, and secondly, to allow patent pool agreements to be negotiated immediately afterwards. This context rejects clauses that exclude middle-income countries from sharing in the patent pool. Expected results: The suggested trade context can help speed up the partici- pation of originator pharmaceutical companies in the Medicines Patent Pool, while allowing them to maintain competitiveness, take advantage of incoming joint ven- ture opportunities and circumvent the need for additional incentives. This context potentially tackles in an appropriate way the directions of evolution in emerging markets, while bringing benefits to resource-limited populations, multinational drug corporations and manufacturers from middle-income countries. -

Licensing Terms and Effectiveness of the Medicines Patent Pool
Oldenburger Studien zur Europäisierung und zur transnationalen Regulierung (ISSN: 1866‐8798) Ausgewählte Abschlussarbeiten ST 2013/05 Licensing Terms and Effectiveness of the Medicines Patent Pool Mareike Sophie Müller Jean Monnet Centre for Europeanisation and Transnational Regulations Oldenburg Fakultät I • Carl-von-Ossietzky-Universität Oldenburg • 26111 Oldenburg Abrufbar im Internet unter: http://www.uni-oldenburg.de/cetro/31251.html Content List of abbreviations IV 1. Introduction 1 2. Intellectual property in the field of pharmaceuticals 5 3. Patent pools and their development of application 8 4. The Medicines Patent Pool 4.1 Patent pools in the field of medicines: The foundation of the Medicines Patent Pool 10 4.2 Motives to establish the Medicines Patent Pool 12 4.3 The MPP’s entities and its operating mechanism 14 5. Licenses granted to the MPP and their licensing terms 5.1 Licenses in the pool 16 5.2 Field of use 23 5.3 Geographic coverage 24 5.4 Termination provisions of the license agreements 33 6. Sublicenses granted by the MPP and their licensing terms 6.1 Sublicensees of the patents licensed to the pool 35 6.2 Sourcing of active pharmaceutical ingredients 44 6.3 Royalties 46 6.4 Ability of sublicensees to supply to countries outside the licensed territory 49 6.5 Grant back provisions 52 6.6 Ability to challenge the licensed patents 55 6.7 Termination of the sublicense agreements 57 7. Effectiveness of the License Agreements 7.1 The MPP-NIH License 60 7.2 The MPP-Gilead License and associated sublicenses 61 7.3 The MPP-ViiV Healthcare License and associated sublicenses 63 7.4 The MPP-Roche License 64 8. -
The Access to Medicine Index 2014 Access to Medicine Foundation Scheepmakersdijk 5A NL-2011 AS Haarlem the Netherlands
The Access to Medicine Index 2014 Access to Medicine Foundation Scheepmakersdijk 5a NL-2011 AS Haarlem The Netherlands On behalf of the Access to Medicine Foundation, Please contact Jayasree K. Iyer, Head of Research E [email protected] and [email protected] T +31 (0)23 53 39 187 W www.accesstomedicineindex.org Funders This report was made possible by financial support from the Bill & Melinda Gates Foundation, the UK Department for International Development (DFID), and the Dutch Ministry of Foreign Affairs. The Access to Medicine Index 2014 Access to Medicine Foundation November 2014 Access to Medicine Index 2014 Acknowledgements The 2014 Access to Medicine Index 2014 is made possible through the collaborative team effort of several experts, authors, researchers and analysts.1 The Foundation is grateful for their contributions and expertise, and would like offer thanks to those individuals who provided valuable feedback throughout the development of the 2014 Index. Funders Bill & Melinda Gates Foundation UK Department for International Development (DFID) The Netherlands Ministry of Foreign Affairs Expert Review Committee The Access to Medicine Hans Hogerzeil (Chair) Research team Natacha Dimitrijevic Jayasree K. Iyer Marja Esveld Delphi Coppens Regina Kamoga Danny Edwards Richard Laing Tara Prasad Dennis Ross-Degnan Laurien Rook Dilip Shah Lisanne Urlings Peter Shelby Editorial team Technical subcommittees Hans Hogerzeil Peter Beyer Jayasree K. Iyer Esteban Burrone Anna Massey Jennifer Dent Ed Monchen Jaime Espin Emma Ross Michele Forzley Suzanne Wolf Javier Guzman Warren Kaplan Data collection and scoring Jillian Kohler Sustainalytics Niranjan Konduri Andrea van Dijk Prashant Yadav Teodora Blidaru Radoslav Georgiev Reviewers Hazel Goedhart Esteban Burrone Vikram Puppala Jennifer Dent Hans Hogerzeil Report Design Richard Laing Explanation Design BV Jillian Kohler Niranjan Konduri IT Efficiency Online BV Other contributors Gbola Amusa Printers Sara Brewer Drukkerij Aeroprint Theo K. -

Access to Medicine Index 2018 Methodologyaccess to REPORT Medicine Index 2018 Methodology Report 2017
Access to Medicine Foundation Access to Medicine Index 2018 METHODOLOGYAccess to REPORT Medicine Index 2018 Methodology Report 2017 ACCESS TO MEDICINE FOUNDATION September 2017 1 Methodology for the 2018 Access to Medicine Index ACKNOWLEDGEMENTS The Access to Medicine Foundation would like to thank the following people and organisations for their contributions to this report. FUNDERS Bill & Melinda Gates Foundation The UK government The Netherlands Ministry of Foreign Affairs EXPERT REVIEW COMMITTEE Hans Hogerzeil (Chair) Sanne Frost-Helt Fumie Griego Suzanne Hill Frasia Karua Dennis Ross-Degnan Dilip Shah Yo Takatsuki Joshua Wamboga Prashant Yadav TECHNICAL SUBCOMMITTEES RESEARCH TEAM EDITORIAL TEAM Esteban Burrone Danny Edwards Anna Massey Nick Chapman Beth Boyer Deirdre Cogan Jennifer Dent Clarke Cole Michele Forzley Luca Genovese Warren Kaplan Catherine Gray Jillian Kohler Nestor Papanikolaou Niranjan Konduri Tara Prasad Stine Trolle ADDITIONAL CONTRIBUTORS We would like to thank the many other experts who contributed their views to the development of this methodology (see page 56). ACCESS TO MEDICINE FOUNDATION The Access to Medicine Foundation is an independent non-profit org- anisation based in the Netherlands. It aims to advance access to medi- cine in low- and middle-income countries by stimulating and guiding the pharmaceutical industry to play a greater role in improving access. Naritaweg 227-A 1043 CB, Amsterdam The Netherlands For questions about this report, please contact Danny Edwards, Research Programme Manager [email protected] +31 (0) 20 215 35 35 www.accesstomedicineindex.org 2 Access to Medicine Foundation A good practice framework There is no simple blueprint for making medicine accessible During ten years of research, we have identified real progress to all who need them. -
Access to Medicine Index 2018 Access to Medicine Foundation
Access to Medicine Index 2018 Access to Medicine Foundation Access to Medicine Index 2018 ACCESS TO MEDICINE FOUNDATION November 2018 1 Access to Medicine Index 2018 ACKNOWLEDGEMENTS The Access to Medicine Foundation would like to thank the following people and organisations for their contributions to this report. FUNDERS UK Department for International Development The Dutch Ministry of Foreign Aff airs Bill & Melinda Gates Foundation EXPERT REVIEW COMMITTEE RESEARCH TEAM Hans Hogerzeil – Chair Danny Edwards Sanne Frost Helt Beth Boyer Fumie Griego Clarke Cole Suzanne Hill Myriam Diallo Frasia Karua Karrar Karrar Dennis Ross-Degnan Alex Kong Dilip Shah Nestor Papanikolaou Yo Takatsuki Stine Trolle Joshua Wamboga Margo Warren Prashant Yadav Mariska van der Zee REVIEWERS EDITORIAL TEAM Hans Hogerzeil Anna Massey Gabrielle Breugelmans Deirdre Cogan Esteban Burrone Emma Ross Jennifer Dent Michele Forzley ADDITIONAL CONTRIBUTORS Frasia Karua We would like to thank the many other experts Niranjan Konduri who contributed their views to the development of this report (see Appendix XVI). ACCESS TO MEDICINE FOUNDATION The Access to Medicine Foundation is an independent non-profi t organisation based in the Netherlands. It aims to advance access to medicine in low- and middle-income countries by stimulating and guiding the pharmaceutical industry to play a greater role in improving access. Naritaweg 227-A 1043 CB, Amsterdam The Netherlands For questions about this report, please contact Danny Edwards, Research Programme Manager [email protected] +31 (0) 20 215 35 35 www.accesstomedicineindex.org 2 Access to Medicine Foundation How to radically ramp up access to healthcare How can we radically ramp up access to healthcare worldwide? This 6th Access to Medicine Index shows where pharmaceutical companies are currently focusing their efforts to improve access. -

P a T I E N T S Innovation P a R T N E
Annual Report 2018 PATIENTS INNOVATION PARTNERS In cancer, modern care helps Advanced analytics enable us to Roche is expanding its colla b where no effective treatments were create a wealth of new data insights orations, combining its own available previously. Innovative and opportunities across the strengths with the unique tools of therapies allow this woman on entire product lifecycle and R&D its partners to elevate personalised the cover picture to carry on with value chain to ultimately improve healthcare to a new level for many her life. See back cover for more. outcomes for patients. more patients. Keith Terry, Genentech, USA “This was an emotional hire for me.” I am the Medical Doctor Talent Scout for Genentech with family and friends—and not dwell on the in South San Francisco and work closely with our negative. It has taught me to stay in the moment. Product Development Neuroscience team. Ironically, There have been some down times too, when I I had a big win with the hiring of a senior medical experienced a relapse. I felt so fatigued that it was director for Ocrevus, the medication that I currently an effort just to breathe. It is difficult to imagine use to treat my multiple sclerosis (MS). This was an this level of fatigue until you have experienced it. emotional hire for me. This illness has really increased my capacity for empathy for those that are ill. I was diagnosed with multiple sclerosis 16 years ago at the age of 37. I had been experiencing extreme But overall there have been many positives. -

2013 Prioritisation Report Priority Antiretrovirals for the Medicines
PRIORITY ANTIRETROVIRALS FOR THE MEDICINES PATENT POOL Third Edition | December 2013 Advancing innovation, access, and public health 1 CONTENTS 3 Introduction 4 Section 1: ARV Prioritisation in Light of New WHO Treatment Guidelines 5 Priority Regimens for Adults 9 Priority Regimens for Children and Adolescents 13 Section 2: Prioritisation of New ARVs and ARVs in the Pipeline 16 Conclusions 18 Annex I - Methodology 22 Annex II - Product Cards 23 Annex IIa: Product Cards for ARVs Prioritised in Light of New WHO Treatment Guidelines 36 Annex IIb: Product Cards for New ARVs and ARVs in the Pipeline 45 Annex IIc: Products in Early Stages of Development* 48 Annex III - Acronyms and Definitions 51 References ACKNOWLEDGMENTS The lead authors of this Working Paper were Esteban Burrone, Head of Policy, and Fernando Pascual, Medical/Pharmaceutical Consultant, of the Medicines Patent Pool. The paper also benefitted from extensive inputs from Robyn Harshaw, Sandeep Juneja, Kaitlin Mara, Chan Park, and Greg Perry. The Medicines Patent Pool (MPP) wants to thank the following external peer reviewers for their comments on an earlier draft: Jintanat Ananworanich, Pascale Boulet, Pedro Cahn, Polly Clayden, Jennifer Cohn, Meg Doherty, Diane Gibb, Raul Gonzalez, Andy Gray, Andrew Hill, Janice Lee, Rohit Malpani, Carmen Pérez-Casas, David Ripin, Marco Vitoria, and the MPP Expert Advisory Group composed of: Labeeb Abboud, Jonathan Berger, Alexandra Calmy, Shing Chang, Carlos Correa, Nelson Juma Otwoma, Eun-Joo Min, Lita Nelsen, Achal Prabhala, Gracia Violeta Ross, Maximiliano Santa Cruz, and Wim Vandevelde. 2 INTRODUCTION TO THE THIRD EDITION OF THE WORKING PAPER Since the first antiretroviral (ARV) information on the patent status, regulatory status received regulatory approval by the US and market trends for different ARVs. -

Projected Savings Through Public Health Voluntary Licences of HIV Drugs Negotiated by the Medicines Patent Pool (MPP)
RESEARCH ARTICLE Projected savings through public health voluntary licences of HIV drugs negotiated by the Medicines Patent Pool (MPP) Sandeep Juneja1, Aastha Gupta1*, Suerie Moon2, Stephen Resch2 1 Medicines Patent Pool, Geneva, Switzerland, 2 Harvard T.H. Chan School of Public Health, Boston, United States of America * [email protected] a1111111111 Abstract a1111111111 a1111111111 The Medicines Patent Pool (MPP) was established in 2010 to ensure timely access to low- a1111111111 a1111111111 cost generic versions of patented antiretroviral (ARV) medicines in low- and middle-income countries (LMICs) through the negotiation of voluntary licences with patent holders. While robust data on the savings generated by MPP and other major global public health initiatives is important, it is also difficult to quantify. In this study, we estimate the savings generated by licences negotiated by the MPP for ARV medicines to treat HIV/AIDS in LMICs for the period OPEN ACCESS 2010±2028 and generate a cost-benefit ratio±based on people living with HIV (PLHIVs) in Citation: Juneja S, Gupta A, Moon S, Resch S any new countries which gain access to an ARV due to MPP licences and the price differen- (2017) Projected savings through public health voluntary licences of HIV drugs negotiated by the tial between originator's tiered price and generics price, within the period where that ARV is Medicines Patent Pool (MPP). PLoS ONE 12(5): patented. We found that the direct savings generated by the MPP are estimated to be USD e0177770. https://doi.org/10.1371/journal. 2.3 billion (net present value) by 2028, representing an estimated cost-benefit ratio of 1:43, pone.0177770 which means for every USD 1 spent on MPP, the global public health community saves Editor: Eduard J. -

Expanding for Better Treatment Options
ANNUAL REPORT 2016 EXPANDING FOR BETTER TREATMENT OPTIONS 1 Style Guide February 2017 Table of contents Message from the Chair of the Governance Board and the Executive Director p. 2 • Governance / Our funder p. 4 • 2016 Achievements p. 6 • How We Work p. 7 • HIV p. 9 • Hepatitis C p. 13 • Tuberculosis p. 14 • Product Development p. 17 • Technical Expertise p. 18 • Financial Statements p. 20 • Acronyms p. 32 1 VisionStyle Guide The vision of the MPP is a world in which people in low- and middle-income countries have rapid access to affordable and appropriate HIV, hepatitis C and tuberculosis treatments. February 2017 Mission Our mission is to increase access and promote innovation in the fields of HIV, hepatitis C and tuberculosis treatment through voluntary licensing and patent pooling. Founded in 2010 by Unitaid, the MPP works with a range of partners – industry, civil society, international organisations, patient groups and governments – to prioritise and license new and existing medicines for low- and middle-income countries. Medicines Patent Pool ANNUAL REPORT 2016 1 Message from the Chair of the Governance Board and the Executive Director e are pleased to present our 2016 Annual Report to all stakehol- ders and supporters. Twenty sixteen was a dynamic year for the Medicines Patent Pool (MPP) and for the access to medicines field. With MPP funder Unitaid’s approval for our expansion into hepati- Wtis C and tuberculosis (TB) in late 2015, we made quick headway in these new disease areas. The MPP signed its first sublicensing agreements for a hepatitis C antiviral and our first memorandum of understanding to pro- mote TB drug development in the early part of the year.