Access to Medicine Index 2018 Methodologyaccess to REPORT Medicine Index 2018 Methodology Report 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
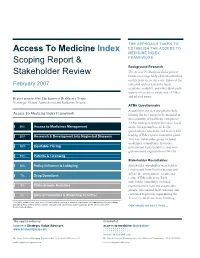
Access to Medicine Index Scoping Report & Stakeholder Review
THE APPROACH TAKEN TO Access To Medicine Index ESTABLISH THE ACCESS TO MEDICINE INDEX Scoping Report & FRAMEWORK Background Research The Access To Medicine Index project Stakeholder Review builds on a large body of work published on this issue in recent years. Innovest has February 2007 collected and reviewed the latest academic, industry, and other third-party reports on access to medicines (ATMs) and related issues. Report prepared by The Innovest Healthcare Team: Veronique Menou, Adam Savitz and Katharine Preston. ATMs Questionnaire A questionnaire was designed to help Access To Medicine Index Framework identify the key issues to be included in an evaluation of healthcare companies’ ATMs strategies and performance based 20% Access to Medicines Management on the background research. The questionnaire was delivered to over 200 20% Research & Development into Neglected Diseases leading ATMs experts around the globe. This key stakeholder group included academics, consultants, investors, 18% Equitable Pricing government representatives, and non- governmental organizations (NGOs). 15% Patents & Licensing Stakeholder Roundtables 10% Policy Influence & Lobbying Stakeholder roundtables were held in London and New York to discuss and debate the questionnaire results and 7% Drug Donations refine ATMs indicators. Each stakeholder roundtable included 5% Philanthropic Activities representatives from the stakeholder groups, who shared their expertise and 5% Ethical Promotion & Marketing Activities continued to provide input during the Access To Medicine Index building This table includes the eight most relevant criteria, ranked in order of importance, as indicated by the percentage weighting. This criteria will be used to evaluate each pharmaceutical company’s performance during the CONTINUED ON NEXT PAGE… benchmarking phase. -

2020 Health for Humanity Report
2020 Health for Humanity Report Progress in Sustainability Contents | Message from Our CEO | Our Approach | United in Defeating COVID-19 | Better Health for All | Responsible Business Practices | Reporting Hub Contents Message from Our Chairman and CEO 3 2020 Year in Brief 4 Our Recognitions 5 Our Approach 6 Health for Humanity Strategy & Goals 9 Sustainability Governance 13 Sustainability Priorities 14 United in Defeating COVID-19 15 Caring for Patients 17 Supporting the Front Lines of Care 24 Protecting Employees 25 Supply Chain Resilience 28 Better Health for All 30 Innovation 31 Global Public Health Strategy 35 Access & Affordability 45 Strengthening Health Systems 48 Responsible Business Practices 52 Ethics & Values 53 Our People 60 Product Quality & Safety 74 Environmental Health 79 Responsible Supply Base 90 ABOVE: During the COVID-19 pandemic, Report overview community healthcare workers in Peru Reporting Hub 98 This Report details the progress of the Johnson & Johnson Family traveled door-to-door to reach children with ESG Summary 98 of Companies in sustainability. It is also our primary source of VERMOX Chewable tablets for treatment of Performance Data 98 annual disclosure on environmental, social and governance intestinal worms. The medicine is donated GRI Content Index 98 (ESG) performance and should be reviewed in conjunction by Johnson & Johnson and implemented GRI Culture of Health for Business Framework 98 with disclosures on the ESG Policies & Positions page. Data by INMED Partnerships for Children. SASB Index 98 in this Report cover the period between January 1, 2020, and Photo by INMED Partnerships for Children. TCFD 98 December 31, 2020, unless otherwise noted. -
The Access to Medicine Index 2014 Access to Medicine Foundation Scheepmakersdijk 5A NL-2011 AS Haarlem the Netherlands
The Access to Medicine Index 2014 Access to Medicine Foundation Scheepmakersdijk 5a NL-2011 AS Haarlem The Netherlands On behalf of the Access to Medicine Foundation, Please contact Jayasree K. Iyer, Head of Research E [email protected] and [email protected] T +31 (0)23 53 39 187 W www.accesstomedicineindex.org Funders This report was made possible by financial support from the Bill & Melinda Gates Foundation, the UK Department for International Development (DFID), and the Dutch Ministry of Foreign Affairs. The Access to Medicine Index 2014 Access to Medicine Foundation November 2014 Access to Medicine Index 2014 Acknowledgements The 2014 Access to Medicine Index 2014 is made possible through the collaborative team effort of several experts, authors, researchers and analysts.1 The Foundation is grateful for their contributions and expertise, and would like offer thanks to those individuals who provided valuable feedback throughout the development of the 2014 Index. Funders Bill & Melinda Gates Foundation UK Department for International Development (DFID) The Netherlands Ministry of Foreign Affairs Expert Review Committee The Access to Medicine Hans Hogerzeil (Chair) Research team Natacha Dimitrijevic Jayasree K. Iyer Marja Esveld Delphi Coppens Regina Kamoga Danny Edwards Richard Laing Tara Prasad Dennis Ross-Degnan Laurien Rook Dilip Shah Lisanne Urlings Peter Shelby Editorial team Technical subcommittees Hans Hogerzeil Peter Beyer Jayasree K. Iyer Esteban Burrone Anna Massey Jennifer Dent Ed Monchen Jaime Espin Emma Ross Michele Forzley Suzanne Wolf Javier Guzman Warren Kaplan Data collection and scoring Jillian Kohler Sustainalytics Niranjan Konduri Andrea van Dijk Prashant Yadav Teodora Blidaru Radoslav Georgiev Reviewers Hazel Goedhart Esteban Burrone Vikram Puppala Jennifer Dent Hans Hogerzeil Report Design Richard Laing Explanation Design BV Jillian Kohler Niranjan Konduri IT Efficiency Online BV Other contributors Gbola Amusa Printers Sara Brewer Drukkerij Aeroprint Theo K. -
Access to Medicine Index 2018 Access to Medicine Foundation
Access to Medicine Index 2018 Access to Medicine Foundation Access to Medicine Index 2018 ACCESS TO MEDICINE FOUNDATION November 2018 1 Access to Medicine Index 2018 ACKNOWLEDGEMENTS The Access to Medicine Foundation would like to thank the following people and organisations for their contributions to this report. FUNDERS UK Department for International Development The Dutch Ministry of Foreign Aff airs Bill & Melinda Gates Foundation EXPERT REVIEW COMMITTEE RESEARCH TEAM Hans Hogerzeil – Chair Danny Edwards Sanne Frost Helt Beth Boyer Fumie Griego Clarke Cole Suzanne Hill Myriam Diallo Frasia Karua Karrar Karrar Dennis Ross-Degnan Alex Kong Dilip Shah Nestor Papanikolaou Yo Takatsuki Stine Trolle Joshua Wamboga Margo Warren Prashant Yadav Mariska van der Zee REVIEWERS EDITORIAL TEAM Hans Hogerzeil Anna Massey Gabrielle Breugelmans Deirdre Cogan Esteban Burrone Emma Ross Jennifer Dent Michele Forzley ADDITIONAL CONTRIBUTORS Frasia Karua We would like to thank the many other experts Niranjan Konduri who contributed their views to the development of this report (see Appendix XVI). ACCESS TO MEDICINE FOUNDATION The Access to Medicine Foundation is an independent non-profi t organisation based in the Netherlands. It aims to advance access to medicine in low- and middle-income countries by stimulating and guiding the pharmaceutical industry to play a greater role in improving access. Naritaweg 227-A 1043 CB, Amsterdam The Netherlands For questions about this report, please contact Danny Edwards, Research Programme Manager [email protected] +31 (0) 20 215 35 35 www.accesstomedicineindex.org 2 Access to Medicine Foundation How to radically ramp up access to healthcare How can we radically ramp up access to healthcare worldwide? This 6th Access to Medicine Index shows where pharmaceutical companies are currently focusing their efforts to improve access. -

P a T I E N T S Innovation P a R T N E
Annual Report 2018 PATIENTS INNOVATION PARTNERS In cancer, modern care helps Advanced analytics enable us to Roche is expanding its colla b where no effective treatments were create a wealth of new data insights orations, combining its own available previously. Innovative and opportunities across the strengths with the unique tools of therapies allow this woman on entire product lifecycle and R&D its partners to elevate personalised the cover picture to carry on with value chain to ultimately improve healthcare to a new level for many her life. See back cover for more. outcomes for patients. more patients. Keith Terry, Genentech, USA “This was an emotional hire for me.” I am the Medical Doctor Talent Scout for Genentech with family and friends—and not dwell on the in South San Francisco and work closely with our negative. It has taught me to stay in the moment. Product Development Neuroscience team. Ironically, There have been some down times too, when I I had a big win with the hiring of a senior medical experienced a relapse. I felt so fatigued that it was director for Ocrevus, the medication that I currently an effort just to breathe. It is difficult to imagine use to treat my multiple sclerosis (MS). This was an this level of fatigue until you have experienced it. emotional hire for me. This illness has really increased my capacity for empathy for those that are ill. I was diagnosed with multiple sclerosis 16 years ago at the age of 37. I had been experiencing extreme But overall there have been many positives. -
The Role of Intellectual Property in Local Production in Developing
Monitoring and Intellectual R&D, Technology Financing Property and Trade Innovation Transfer Improving Access Reporting Opportunities and challenges The role of intellectual property in local production in developing countries The role of intellectual property in local production in developing countries Opportunities and challenges WHO Library Cataloguing-in-Publication Data The role of intellectual property in local production in developing countries: opportunities and challenges. 1.Intellectual Property. 2.Technology Transfer. 3.Drugs, Essential. 4.Patents. 5.Developing Countries. I.World Health Organization ISBN 978 92 4 151030 1 (NLM classification: QV 704) © World Health Organization 2016 All rights reserved. Publications of the World Health Organization are available on the WHO website (http://www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications –whether for sale or for non- commercial distribution– should be addressed to WHO Press through the WHO website (http:// www.who.int/about/licensing/copyright_form/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

New Products Alone Are Not Enough. Pharma Can Do More to Halt COVID-19
VIEWPOINT New products alone are not enough. Pharma can do more to halt COVID-19. By Danny J Edwards, Research Programme Manager, Access to Medicine Foundation 14 April 2020 The COVID-19 epidemic will hit the most have been tracking and evaluating their actions in vulnerable people hardest. The pharmaceutical this area for more than ten years. industry has a responsibility to do more than develop new vaccines and medicines – it must also Positive steps being taken help achieve fair, global access to new products. The actions for pharmaceutical companies to take during this crisis are clear: the development and The COVID-19 pandemic is confirming many equitable delivery of health products, done in an important truths – two of which stand out from ethical and responsible manner. We have the perspective of our organisation. First, any confirmed these priorities via a broad-ranging successful response requires the pharmaceutical stakeholder dialogue and distilled them into the industry to fully engage and respond with agility. new analytical framework for the next Access to This industry will play a critical role in saving lives Medicine Index. first and foremost and in getting us back on our It is encouraging to see companies already feet to restart a stalling global economy. taking positive steps in response to global calls for Second, this pandemic is going to hit the people action, particularly to develop new medicines and living in low- and middle-income countries the vaccines. This is despite some counter examples, hardest. With weaker health systems and greater such as movements (now reversed) to extend or threats to health, these countries face a tougher safeguard exclusivity rights for potential challenge from COVID-19. -

Taming Big Pharma Assessing How Insurers Push Pharmaceutical Companies to Improve Access to Medicine and Pay Fair Taxes
Taming Big Pharma Assessing how insurers push pharmaceutical companies to improve access to medicine and pay fair taxes Fair Insurance Guide 25 April 2019 Fair Insurance Guide Taming Big Pharma Assessing how insurers push pharmaceutical companies to improve access to medicine and pay fair taxes The Fair Insurance Guide is a coalition of the following organisations: Amnesty International, FNV, Milieudefensie, Oxfam Novib, PAX and World Animal Protection.1 25 April 2019 Research by: the Centre for Research on Multinational Corporations (SOMO) Acronyms AtM Access to Medicine BEPS Base erosion and profit shifting ESG Environmental, social and governance ETR Effective tax rate FDA Food and Drug Administration (US) GRI Global Reporting Initiative OECD Organisation for Economic Co-operation and Development OHCHR United Nations Office of the High Commissioner for Human Rights PRI Principles for Responsible Investment R&D Research and Development SDG Sustainable Development Goal SEC Securities and Exchange Commission (US) SOMO Centre for Research on Multinational Corporations SRI Socially responsible investment TRIPS Trade-Related Intellectual Property UN United Nations WHO World Health Organization WTO World Trade Organization Table of contents Summary ................................................................................................................. 1 Chapter 1 Introduction.............................................................................................. 8 Context and research aims ............................................................................................ -

Patients at Our Center Pfizer 2018 Annual Review from Leadership Our Business Our Innovation Our Culture, Our Purpose Our Performance
Patients at Our Center Pfizer 2018 Annual Review From Leadership Our Business Our Innovation Our Culture, Our Purpose Our Performance Contents From Leadership Partnering in Innovation 3 A Letter from Our Executive Chairman and CEO 31 Pfizer Tackles Antimicrobial Resistance 31 Improving Global Outcomes in Metastatic Breast Cancer Our Business 32 Advancing Sickle Cell Disease Awareness, Understanding & Diagnosis Understanding the External Environment 32 Partnering in Hemophilia 6 Providing Access to Patent Information to Improve Global Health Outcomes 33 Sparking Innovative Ideas to Deliver Vaccines to the Hardest-To-Reach "Last Mile" 6 Resilience Matters 33 Prioritizing Preventive Care and CDC-Recommended Immunizations With Baby 7 Understanding the External Environment Checkups Count 9 Making Our Medicines Accessible to the Patients Who Need Them 34 Driving Increased Colorectal Cancer Screening: Addressing a Substantial Unmet Need 9 Pfizer Launches New Framework to Enable Quicker, More Effective Response to Major 34 Partnering to Help Protect Babies in the U.S. Societal Issues 34 Eliquis® Continues to Differentiate in NVAF 10 Three Virtues Initiative Strives to Transform African-American Health and Wellness 35 BMS-Pfizer Alliance Working to Understand Gaps in Atrial Fibrillation (AFib) Detection and Diagnosis Manufacturing & Supply Chain Excellence 35 Innovation in Chronic Pain Management 11 Pfizer Sites Provide an Inclusive and Inspiring Work Environment 11 Students and Faculty Visit a Pfizer Site to Learn About Modern Manufacturing Advancing -
The Access to Medicine Index 2014 Access to Medicine Foundation Scheepmakersdijk 5A NL-2011 AS Haarlem the Netherlands
The Access to Medicine Index 2014 Access to Medicine Foundation Scheepmakersdijk 5a NL-2011 AS Haarlem The Netherlands On behalf of the Access to Medicine Foundation, Please contact Jayasree K. Iyer, Head of Research E [email protected] and [email protected] T +31 (0)23 53 39 187 W www.accesstomedicineindex.org Funders This report was made possible by financial support from the Bill & Melinda Gates Foundation, the UK Department for International Development (DFID), and the Dutch Ministry of Foreign Affairs. The Access to Medicine Index 2014 Access to Medicine Foundation November 2014 Access to Medicine Index 2014 Acknowledgements The 2014 Access to Medicine Index 2014 is made possible through the collaborative team effort of several experts, authors, researchers and analysts.1 The Foundation is grateful for their contributions and expertise, and would like offer thanks to those individuals who provided valuable feedback throughout the development of the 2014 Index. Funders Bill & Melinda Gates Foundation UK Department for International Development (DFID) The Netherlands Ministry of Foreign Affairs Expert Review Committee The Access to Medicine Hans Hogerzeil (Chair) Research team Natacha Dimitrijevic Jayasree K. Iyer Marja Esveld Delphi Coppens Regina Kamoga Danny Edwards Richard Laing Tara Prasad Dennis Ross-Degnan Laurien Rook Dilip Shah Lisanne Urlings Peter Shelby Editorial team Technical subcommittees Hans Hogerzeil Peter Beyer Jayasree K. Iyer Esteban Burrone Anna Massey Jennifer Dent Ed Monchen Jaime Espin Emma Ross Michele Forzley Suzanne Wolf Javier Guzman Warren Kaplan Data collection and scoring Jillian Kohler Sustainalytics Niranjan Konduri Andrea van Dijk Prashant Yadav Teodora Blidaru Radoslav Georgiev Reviewers Hazel Goedhart Esteban Burrone Vikram Puppala Jennifer Dent Hans Hogerzeil Report Design Richard Laing Explanation Design BV Jillian Kohler Niranjan Konduri IT Efficiency Online BV Other contributors Gbola Amusa Printers Sara Brewer Drukkerij Aeroprint Theo K. -
Ten-Year Impact of the Access to Medicine Index: Changes in Industry Pricing and Intellectual Property Policies in Low- and Middle-Income Countries from 2008-2018
Ten-year impact of the Access to Medicine Index: Changes in industry pricing and intellectual property policies in Low- and Middle-Income Countries from 2008-2018 Hans V Hogerzeil, Daniel J Edwards, Jayasree K Iyer 23-24 October 2019, Vienna Acknowledgements • This study was made possible with financial support from UK Aid, the Bill & Melinda Gates Foundation and the Dutch Ministry of Foreign Affairs • Researchers were independent in their analysis and in the presentation of the results; they have no potential conflict of interest to report • The study was performed by Alex Kong, Margo Warren, Danny Edwards, Karrar Karrar and Jayasree K. Iyer; and was edited by Anna V. Massey • The full report is available on: accesstomedicinefoundation.org/publications The Access to Medicine Foundation • The Access to Medicine Foundation is an independent non-profit organisation, based in the Netherlands. • It aims to advance access to medicine in low- and middle-income countries by stimulating and guiding the pharmaceutical industry to play a greater role in improving access to medicine. • It has published the Access to Medicine Index every two years since 2008. • 106 Low- and Middle-Income Countries are covered by the ATM Index; covering 83% of the world population. • In 2017 it published its first Access to Vaccines Index, and in 2018 the first Antimicrobial Resistance Benchmark. Since 2008, multiple companies have pioneered good practice • Merck & Co began a donation programme for onchocerciasis in 1987, which is ongoing today. • Novartis was the first to publicly commit to establishing access plans for all innovative new medicines. Access plans can cover pricing, registration and supply. -
Second-Party Opinion Novartis Sustainability-Linked Notes
Second-Party Opinion Novartis Sustainability-Linked Notes Evaluation Summary Sustainalytics is of the opinion that the Novartis Sustainability-Linked Notes align with Evaluation date September 2020 the Sustainability Linked Bond Principles 2020 and considers the KPIs to be relevant Issuer Location Luxembourg, and material to the issuer and the SPTs to be credible and impactful. This assessment Grand Duchy of is based on the following: Luxembourg Novartis has Introduction .................................................. 2 selected two internally tracked KPIs, (i) Strategic Innovative Sustainalytics’ Opinion ................................ 3 Therapies Patient Reach and (ii) Flagship Programs Patient Reach, Appendix 1 ................................................. 11 for the Sustainability Linked Notes (SLN). Sustainalytics considers the KPIs chosen to be relevant and material for the Group, and further considers the Flagship Programs (FP) KPI to be clear and credible. Sustainalytics notes the significant discretion of Novartis’ For inquiries, contact the Sustainable Executive Committee members in the selection of Strategic Finance Solutions project team: Innovative Therapies (SIT) considered in its SIT KPI to be a limitation. Lili Hocke (Amsterdam) Product Manager Novartis [email protected] has established SPTs (2025 Patient Access Targets) to increase its (+31) 20 205 0040 KPI performance by 200% for the SIT KPI and 50% for the FP KPI by 2025. Sustainalytics considers the SPTs to be aligned with the Rebecca Dreyfus (Amsterdam) issuer’s sustainability strategy. Sustainalytics further considers the Project Manager SPTs for both the FP KPI and SIT KPI to represent material [email protected] improvements based on past performance, and to support access (+31) 20 299 46 92 to medicine in low- and middle- income countries.