Enrollment Form Scuba Skills Updater.Pub
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Course Description
Instructor: Walter W Lancaster II Off Campus phone: 951-351-1445 x204 Dept phone: NA Cell phone: 951-312-2589 Department of Health and Exercise Science e-mail: [email protected] Spring Quarter, 2016 Alternate e-mail: [email protected] Off Campus Office: La Sierra Academy Office Hours: M-Th 8am – 4pm Consultations by appointment PEAC 106 Scuba Diving Walter Lancaster Location: Health and Exercise Science Classroom 1 (or other assigned instructional locaton) & Pool Tuesdays 6:30pm ~ 9:45pm I. COURSE DESCRIPTION: A. Bulletin Course Description: Course Description Basic SCUBA Diver is an entry-level course for people who have not been previously certified to SCUBA dive, and provides a comprehensive overview of basic concepts that are required to dive safely. Topics include diving equipment, diving physiology, dive planing, environmental considerations, and recognizing and managing risks associated with Open Water diving. Participants who successfully complete the classroom and pool work will qualify for an Open Water certification experience, which must be completed if the student wishes to become a certified diver. Successful completion of the Open Water experience will result in an industry recognized and accepted certification at the level of Basic SCUBA Diver through the National Assocaiton of Underwater Instructors (NAUI). All attendees must be age 16 or older. Students must be able to demonstrate a 10-minute swim/float in water too deep to stand in without the use of swim aids, complete a 200 meter/yard continuous surface swim and demonstrate an underwater (single breath) free dive for a horizontal minimum distance of 25 yards. B. Instructional Materials: Use of the recommended text and Comprehesive Resource Notebook is made available to all students as part of the comprehensive Lab Fee. -
AMBER WAVES DIVING REPAIR CENTER What to Expect Secrets To
307 South Greenwich Rd. Wichita, KS 67207 To unsubscribe click here 316-775-6688 OFF TO EL DORADO ON A SATURDAY MORNING. WE DID A FIRST AIDCLASS FOR THE FIRST BAPTIST PRE-SCHOOL . THANKS FOR A GREAT TIME. THANKS TO INSTRUCTOR JENNIFER HULL AND DIVE MASTERS ERIC BUCK AND JIM PHILLIPS FOR HELPING THESE YOUNG PEOPLE GET TO THE NEXT PHASE OF THEIR SCUBA TRAINING. BACK TO THE SHOP SATURDAY AFTERNOON TO DO A CLASS FOR THESE WONDERFUL PEOPLE WHO ARE PICTURED ABOVE IS OUR GRADUATES FROM SUNDAY’S FIRST BECOMING FOSTER PARENTS. AID CLASS. SCUBA SCHOOL PADI DISCOVER SCUBA MAR 11 WICHITA STATE SCUBA CLASS SCUBA REVIEW MAR 13-15 OPEN WATER PART ONE CLASS OR JUST COME AND PLAY MAR 14 DISCOVER SCUBA, SCUBA REVIEW ANDOVER BRANCH YMCA POOL COURSE, OR JUST COME AND PLAY SATURDAY MARCH 14, 2020 MAR 15 FIRST AID CLASS Why PADI Scuba Review? MAR 18 WICHITA STATE SCUBA CLASS Are you a certified diver, but haven't been in the water lately? Are MAR 20-22 OPEN WATER PART ONE CLASS you looking to refresh your dive skills and knowledge? Are you a PADI Scuba Diver and want to earn your PADI Open Water Diver MAR 21 DISCOVER SCUBA, SCUBA REVIEW certification? If you answered yes to any of these questions then COURSE, OR JUST COME AND PLAY PADI Scuba Review is for you. MAR 22 FIRST AID CLASS What do I need to start? Hold a scuba certification MAR 27-29 OPEN WATER PART ONE CLASS Minimum age: 10 years old MAR 28 DISCOVER SCUBA, SCUBA REVIEW What will I do? First, you'll review the safety information you learned during your COURSE, OR JUST COME AND PLAY initial training. -
Supervised Dive
EFFECTIVE 1 March 2009 MINIMUM COURSE CONTENT FOR Supervised Diver Certifi cation As Approved By ©2009, Recreational Scuba Training Council, Inc. (RSTC) Recreational Scuba Training Council, Inc. RSTC Coordinator P.O. Box 11083 Jacksonville, FL 32239 USA Recreational Scuba Training Council (RSTC) Minimum Course Content for Supervised Diver Certifi cation 1. Scope and Purpose This standard provides minimum course content requirements for instruction leading to super- vised diver certifi cation in recreational diving with scuba (self-contained underwater breathing appa- ratus). The intent of the standard is to prepare a non diver to the point that he can enjoy scuba diving in open water under controlled conditions—that is, under the supervision of a diving professional (instructor or certifi ed assistant – see defi nitions) and to a limited depth. These requirements do not defi ne full, autonomous certifi cation and should not be confused with Open Water Scuba Certifi cation. (See Recreational Scuba Training Council Minimum Course Content for Open Water Scuba Certifi ca- tion.) The Supervised Diver Certifi cation Standards are a subset of the Open Water Scuba Certifi cation standards. Moreover, as part of the supervised diver course content, supervised divers are informed of the limitations of the certifi cation and urged to continue their training to obtain open water diver certifi - cation. Within the scope of supervised diver training, the requirements of this standard are meant to be com- prehensive, but general in nature. That is, the standard presents all the subject areas essential for su- pervised diver certifi cation, but it does not give a detailed listing of the skills and information encom- passed by each area. -
Tune up Your Scuba Skills
To unsubscribe click here SUCCESS! ALL OF OUR WICHITA STATE SCUBA STUDENTS PASSED THEIR SCUBA WATER SKILLS. THANKS TO OUR LEAD INSTRUCTOR ROYCE TAYLOR, INSTRUCTOR VAUGHN COSSEL, AND DIVE MASTER NEIL GARRETT FOR LEADING THIS GROUP THROUGH A WATER WAS COOL, WEATHER WARM, AND LOTS OF FUN WAS GREAT AND WORTHY JOURNEY. HAD. THANKS TO COURSE DIRECTOR CHRIS HULETT AND IDC STAFF INSTRUCTOR SUSAN HULETT FOR HELPING THESE TWO GET OPEN WATER CERTIFIED SARAH WOELK PADI OPEN CHRIS WOELK PADI OPEN WATER DIVER WATER DIVER WE HAD A WONDERFUL TIME TEACHING AND CERTIFYING THIS GROUP FROM A LOCAL CHURCH IN CPR-AED-AND FIRST AID. SCUBA SCHOOL PADI DISCOVER SCUBA OCT 14 WICHITA STATE SCUBA CLASS SCUBA REVIEW—OR JUST COME AND PLAY ANDOVER BRANCH YMCA POOL OCT 16-18 OPEN WATER PART 2, ADVANCED COURSE, AND ANY DIVE SPECIALTY (BEAVER LAKE) SATURDAY OCTOBER 17, 2020 OCT 18 FIRST AID CLASS Why PADI Scuba Review? OCT 21 WICHITA STATE SCUBA CLASS Are you a certified diver, but haven't been in the water lately? Are you looking to refresh your dive skills and knowledge? Are you a OCT 23-25 OPEN WATER PART ONE CLASS PADI Scuba Diver and want to earn your PADI Open Water Diver OCT 24 DISCOVER SCUBA, SCUBA REVIEW certification? If you answered yes to any of these questions then PADI Scuba Review is for you. COURSE, OR JUST COME AND PLAY What do I need to start? OCT 25 FIRST AID CLASS Hold a scuba certification Minimum age: 10 years old OCT 31-NOV 7 ST. -

General Training Standards, Policies, and Procedures
General Training Standards, Policies, and Procedures Version 9.2 GUE General Training Standards, Policies, and Procedures © 2021 Global Underwater Explorers This document is the property of Global Underwater Explorers. All rights reserved. Unauthorized use or reproduction in any form is prohibited. The information in this document is distributed on an “As Is” basis without warranty. While every precaution has been taken in its preparation, neither the author(s) nor Global Underwater Explorers have any liability to any person or entity with respect to any loss or damage caused or alleged to be caused, directly or indirectly, by this document’s contents. To report violations, comments, or feedback, contact [email protected]. 2 GUE General Training Standards, Policies, and Procedures Version 9.2 Contents 1. Purpose of GUE .............................................................................................................................................6 1.1 GUE Objectives ............................................................................................................................................. 6 1.1.1 Promote Quality Education .................................................................................................................. 6 1.1.2 Promote Global Conservation Initiatives .......................................................................................... 6 1.1.3 Promote Global Exploration Initiatives ............................................................................................. 6 -

Michael Burgan – FF PSD Training
08-10-2012 Sugarcreek OH – Michael Burgan – FF PSD Training 08-10-2012 Michael Burgan Aged 46, Captain in the Sugarcreek Fire department (also dived for the Holmes County dive team) participating in an advanced diving class at the White Star Quarry in Gibsonburg, reported as showing signs of distress after 15 minutes into his second dive of the day, surfaced and called for help before he lost consciousness, recovered from about 61' water depth by fellow divers but pronounced dead at the scene. Firehouse.com news http://www.thediversassociation.com/index.php/sheets POLICE & FIRE Ohio man, 46, dies during diving class http://www.toledoblade.com/Police-Fire/2012/08/12/Ohio-man-46-dies-during- diving-class.html Aug. 12, 2012 Blade Staff and News Services GIBSONBURG, Ohio -- A Sugarcreek, Ohio, man died Friday during an advanced diving instruction class at White Star Quarry, authorities said. Michael Burgan, 46, was more than 15 minutes into his second dive of the day about 2:15 p.m. when he surfaced from about 40 feet of water, said Steve Gruner, director of the Sandusky County Park District. There was no earlier indication that the diver was having a problem, but at the surface, "he indicated he was having some distress," Mr. Gruner said. Mr. Burgan, who was a certified diver, lost consciousness and went under water, Mr. Gruner added. The diving instructor recovered him from a depth of 61 feet. Mr. Burgan was pronounced dead at the scene. His body was transported to the Lucas County coroner's office for an autopsy. -

Psdiver Magazine Issue 119 Page 2
Issue 119 August 2018 The PSDiver Workshop Initiative Are You A Professional Diver? Or, Are You A Recreational Diver With A Specialty Card? Distance Determination For Firearm Recovery MORE 2018 PSD Fatalities Detection Of Latent Prints On Handguns After Submersion In Water The Public Safety Diving Discipline. Find It Before You Dive It: Safety at the expense of common sense, Hull Mounted Vs Towed Side Scan Sonar or can both co-exist? Systems By Mark Michaud By Vince Capon, Black Laser Learning Greetings, reveling even this much is a little unsettling. But if it can happen to me, it can happen to you. Recognizing the problem, You may have noticed that the issues of PSDiver Magazine are gaining an understanding of why we are acting the way we not coming out as fast as they used to. Since I retired, I have sometimes do, acknowledging that the relationship problems we tried to focus more time on not working. I try, but I am not have on occasion is probably our fault - is important. Without very good at it. In fact, I enjoy just about every aspect of the that understanding and acknowledgement, there is no path to work I do in Public Safety Diving. But some of the work does recovery. Recovery - not cured as if you had a sinus infection. I take a toll both physically and mentally. do not think PTSD is something that can be cured. It has to be dealt with. The worse the issues, the harder it is to get to that The last issue released focused on PTSD, Critical Incident Stress point – maybe even impossible for some. -
2020 SSI Recreational Programs
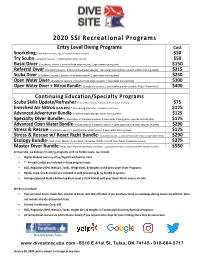
2020 SSI Recreational Programs Entry Level Diving Programs Cost Snorkeling (1 academic session, 1 pool/confined water session) $50 Try Scuba (1 academic session, 1 pool/confined water session) $50 Basic Diver (1 academic session, 1 pool/confined water session, 1 open water training dive) $150 Referral Diver (2 academic sessions, 2 pool/confined water sessions; open water training dives are with another training center) $215 Scuba Diver (1 academic session, 1 pool/confined water session, 2 open water training dives) $250 Open Water Diver* (2 academic sessions, 2 pool/confined water sessions, 4 open water training dives) $300 Open Water Diver + Nitrox Bundle* (2 academic sessions, 2 pool/confined water sessions, 4 Open Water dives) $400 Continuing Education/Specialty Programs Scuba Skills Update/Refresher (1 academic session, 1 pool/confined water session) $75 Enriched Air Nitrox (EAN 40%) * (Non-diving Specialty: 1 academic session) $125 Advanced Adventurer Bundle* (5 different specialty open water training dives) $125 Specialty Diver Bundle* (2 Specialties w/ 1 academic session, 3 open water training dives; requires 12 dives total) $175 Advanced Open Water Bundle* (4 Specialties w/ 1 academic session, 5 open water training dives; requires 24 dives) $290 Stress & Rescue* (1 academic session, 1 pool/confined water session, 3 open water training dives) $175 Stress & Rescue w/ React Right Bundle* (2 academic session, 1 pool/confined water session, 3 open water dives) $290 Ecology Bundle* (Pick 5 from Marine, Turtle, Shark, Manta Ray, Fish ID, Coral ID; Non-diving: 1 academic session) $275 Master Diver Bundle* (AOW, Stress Rescue w/React Right; 2 academic, 1 pool/confined water, 8 OW training dives; requires 50 dives) $550 At Dive Site, we believe in training programs with no hidden costs, we include: • Digital Student Learning Kit w/Digital Certification Card • * - Printed Card(s) are included in these program costs. -

23. SDI – Solo Diver Specialty
SDI Instructor Manual Date: 09/04/2001 Part 4 – Standards & Revision: 2.1 Outlines for Specialties 23. SDI – Solo Diver Specialty 23.1 Introduction The objective of this course is to train divers in the benefits, hazards, and proper procedures for diving solo. Upon successful completion of this course, graduates may engage in solo diving activities. 23.2 Who May Teach Who may teach this course? 1. An active SDI Solo Diver Instructor that has been certified to teach this specialty. 23.3 Student – Instructor Ratio Academic: 1. Unlimited, so long as adequate facility, supplies and time are provided to insure comprehensive and complete training. Confined Water (Swimming pool-like conditions): 1. N/A. Open Water (Ocean, lake, quarry, spring, river or estuary): 1. A maximum of eight (8) students per Instructor. However, it is the instructor’s discretion to reduce this number as conditions dictate. 23.4 Student Pre-Requisites 1. Minimum age twenty one (21). 2. Minimum certification of advanced diver or equivalent. 3. Minimum of one hundred (100) logged dives. 4. Completed Medical Diving Release Form. 5. Completed Waiver and Release Form. SDI Instructor Manual - Part 4 - Page 82 of 98 (2.1).doc Copyright ® 2001, SDI SDI Instructor Manual Date: 09/04/2001 Part 4 – Standards & Revision: 2.1 Outlines for Specialties 23.5 Execution And Structure Open Water execution: 1. Two (2) dives are required with complete briefs and debriefs by the Instructor. 2. Dive plan must include Surface interval, Max no-deco time, etc. to be figured out and logged. Course Structure: 1. SDI allows instructors to structure courses according to the number of students participating and their skill level. -

Catalina Sea Camp Scuba Guide
Scuba Diving Participant Guide \TOYON BAY ❖ CATALINA ISLAND ❖ CALIFORNIA 33.3750° N, 118.3537° W Catalina Sea Camp 2020 Scuba Diving Participant Guide Contents About Catalina Sea Camp...............................................................................2 About the Dive Program .................................................................................3 Dive Program Medical Policies ......................................................................5 Other Dive Program Policies ..........................................................................7 Safety and Risk Management .......................................................................11 Diving at Catalina Sea Camp.........................................................................15 Required Paperwork ......................................................................................20 Selecting Scuba Activities .............................................................................26 About Catalina Sea Camp Catalina Sea Camp has been operated by Guided Discoveries, a 501(c)(3) educational nonprofit organization, since 1980. The mission of Guided Discoveries is to “make a difference in the lives of children through unique opportunities for discovery.” Catalina Sea Camp offers exceptional ocean adventure and marine science experiences along with social camp activities. Located at the Catalina Island Marine Institute’s Toyon Bay campus, the coed, overnight summer camp boasts an expansive, protected waterfront and a 90 acre footprint. Specialty -

Staying Fresh and Current a Little Knowledge Can Go a Long Way
Quarterly Journal: July 2013, Vol. 7, No. 3 In this issue: Staying Fresh and Current A little knowledge can go a long way. We applaud the efforts of our leadership Staying Fresh and team. Many go above and beyond to teach and guide students both in diving Current and in life and are a great benefit to the communities in which they live. In this issue, we highlight little ways to make a difference. Teaching students and SEI Instructor Ogoreuc divers what an actively drowning victim looks like, may prove to one day save awarded a life. Encouraging divers to remain current in their diving skills and offering refresher courses for divers that have not been in the water in a given period SEI Instructor Trainer of time helps them become prepared and more comfortable with the skills Phil Graf Spotlighted they need so they are better able to enjoy the diving experience. Always Ready Advanced divers and even leadership could take a refresher for any specialty they may not have practiced in a while as discussed in the article on the Public Safety Training benefits of a DRAM rescue refresher course. Educating and exciting students and even other instructors to the beauty found in your local diving haunts, What a Drowning wets the appetite for lifelong diving adventures. Creating proactive divers Looks Like/Rescuing a can impact the environment for the better as they help to remove trash or Distressed Diver eliminate invasive predators harming the natural eco-structure balance. Quality Education – Every little bit what we are all about! helps so keep up the good Scuba Diving in work! Fabulous Florida Care for Marine Life Left: Gabrielle Sponge Surprise Gabrielli with students and Lionfish License friends at a Waiver/First Aid PSA/ recent dive in More Info Florida; see related article Continuing Education that starts on and Contact Info page 7. -

Underwater-Diving-Safety-Handbook.Pdf
TABLE OF CONTENTS SECTION Page No. 1. OVERVIEW--------------------------------------------------------------------------------- 1 1.1 Program Mission; Goals, Core Products, and Services; and Management 1 1.2 General Provisions 1 2. POSITIONS AND RESPONSIBILITIES--------------------------------------------- 4 2.1 Deputy Director, Bureau of Safety and Environmental Enforcement 4 2.2 Diving Program Manager 4 2.3 Diving Control and Safety Board 5 2.4 Diving Safety Officer 6 2.5 Regional Diving Officer 7 2.6 Lead Diver 8 2.7 Active Divers 9 2.8 Observer Divers [To Be Developed *] 10 2.9 Diver Reciprocity 10 3. ACTIVE DIVER CERTIFICATION AND TRAINING------------------------------ 12 3.1 Active Diver Certification Requirements 12 3.2 Maintaining Certification 14 3.3 Certification Lapse 15 3.4 Suspension and Revocation of Dive Certifications 15 4. DIVING STANDARDS AND PROCEDURES-------------------------------------- 17 4.1 General 17 4.2 Pre-Dive Procedures 19 4.3 Diving Procedures and Requirements 21 4.4 Post-Dive Procedures 22 4.5 SCUBA Diving Mode 23 4.6 Drysuit Diving 24 4.7 Diving in Low Visibility 24 4.8 Overhead Obstruction Diving 24 4.9 Cold-Water Diving 25 4.10 Offshore Platform Diving 25 4.11 Diving Near Known Unexploded Ordinance 26 4.12 Contaminated Water Diving 26 5. DIVING EQUIPMENT-------------------------------------------------------------------- 27 5.1 General Policy 27 5.2 Support Equipment 27 5.3 Open-Circuit SCUBA Diving Equipment 27 6. MEDICAL STANDARDS---------------------------------------------------------------- 30 6.1 Medical Examinations 30 6.2 Reporting Changes in Medical Condition 30 6.3 Lapsed Dive Physicals 30 6.4 Funding for BSEE Diving Physical Examinations 31 7. NITROX DIVING--------------------------------------------------------------------------- 32 7.1 General 32 7.2 Requirements for Authorization to Use Nitrox 32 7.3 Dive Personnel Requirements 32 iii 7.4 Nitrox Diving Equipment 32 8.