Radial Head and Neck Fractures Thomas Krupko M.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CASE REPORT Injuries Following Segway Personal
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Injuries Following Segway Personal Transporter Accidents: Case Report and Review of the Literature Permalink https://escholarship.org/uc/item/37r4387d Journal Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health, 16(5) ISSN 1936-900X Authors Ashurst, John Wagner, Benjamin Publication Date 2015 DOI 10.5811/westjem.2015.7.26549 License https://creativecommons.org/licenses/by/4.0/ 4.0 Peer reviewed eScholarship.org Powered by the California Digital Library University of California CASE REPORT Injuries Following Segway Personal Transporter Accidents: Case Report and Review of the Literature John Ashurst DO, MSc Conemaugh Memorial Medical Center, Department of Emergency Medicine, Benjamin Wagner, DO Johnstown, Pennsylvania Section Editor: Rick A. McPheeters, DO Submission history: Submitted April 20, 2015; Accepted July 9, 2015 Electronically published October 20, 2015 Full text available through open access at http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.2015.7.26549 The Segway® self-balancing personal transporter has been used as a means of transport for sightseeing tourists, military, police and emergency medical personnel. Only recently have reports been published about serious injuries that have been sustained while operating this device. This case describes a 67-year-old male who sustained an oblique fracture of the shaft of the femur while using the Segway® for transportation around his community. We also present a review of the literature. [West J Emerg Med. 2015;16(5):693-695.] INTRODUCTION no parasthesia was noted. In 2001, Dean Kamen developed a self-balancing, zero Radiograph of the right femur demonstrated an oblique emissions personal transportation vehicle, known as the fracture of the proximal shaft of the femur with severe Segway® Personal Transporter (PT).1 The Segway’s® top displacement and angulation (Figure). -

The Appendicular Skeleton Appendicular Skeleton
THE SKELETAL SYSTEM: THE APPENDICULAR SKELETON APPENDICULAR SKELETON The primary function is movement It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton SKELETON OF THE UPPER LIMB Each upper limb has 32 bones Two separate regions 1. The pectoral (shoulder) girdle (2 bones) 2. The free part (30 bones) THE PECTORAL (OR SHOULDER) GIRDLE UPPER LIMB The pectoral girdle consists of two bones, the scapula and the clavicle The free part has 30 bones 1 humerus (arm) 1 ulna (forearm) 1 radius (forearm) 8 carpals (wrist) 19 metacarpal and phalanges (hand) PECTORAL GIRDLE - CLAVICLE The clavicle is “S” shaped The medial end articulates with the manubrium of the sternum forming the sternoclavicular joint The lateral end articulates with the acromion forming the acromioclavicular joint THE CLAVICLE PECTORAL GIRDLE - CLAVICLE The clavicle is convex in shape anteriorly near the sternal junction The clavicle is concave anteriorly on its lateral edge near the acromion CLINICAL CONNECTION - FRACTURED CLAVICLE A fall on an outstretched arm (F.O.O.S.H.) injury can lead to a fractured clavicle The clavicle is weakest at the junction of the two curves Forces are generated through the upper limb to the trunk during a fall Therefore, most breaks occur approximately in the middle of the clavicle PECTORAL GIRDLE - SCAPULA Also called the shoulder blade Triangular in shape Most notable features include the spine, acromion, coracoid process and the glenoid cavity FEATURES ON THE SCAPULA Spine - -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Hand Rehabilitation Current Awareness Bulletin NOVEMBER 2015
1 Hand Rehabilitation Current Awareness Bulletin NOVEMBER 2015 2 Lunchtime Drop-in Sessions The Library and Information Service provides free specialist information skills training for all UHBristol staff and students. To book a place, email: [email protected] If you’re unable to attend we also provide one-to-one or small group sessions. Contact library@ or katie.barnard@ to arrange a session. Literature Searching October (12pm) An in -depth guide on how to search Thurs 8th Statistics the evidence base, including an introduction to UpToDate and Fri 16th Literature Searching Anatomy.tv. Mon 19th Understanding articles Tues 27th Statistics Useful for anybody who wants to find the best and quickest way to source articles. November (1pm) Weds 4th Literature Searching Thurs 12th Understanding articles How to understand an article Fri 20th Statistics How to assess the strengths and Mon 23rd Literature Searching weaknesses of published articles. Examining bias and validity. December (12pm) Tues 1st Understanding articles Weds 9th Statistics Medi cal Statistics Thurs 17th Literature Searching A basic introduction to the key statistics in medical articles. Giving an overview of statistics that compare risk, test confidence, analyse clinical investigations, and test difference. 3 Contents Contents .................................................................................................................................................. 3 New from Cochrane Database of Systematic Reviews .......................................................................... -

Radial Head Fractures Treated with Open Reduction and Internal Fixation
Moghaddam et al. Trauma Cases Rev 2016, 2:028 Volume 2 | Issue 1 ISSN: 2469-5777 Trauma Cases and Reviews Research Article: Open Access Radial Head Fractures Treated with Open Reduction and Internal Fixation Moghaddam A1*, Raven TF1, Kaghazian P1, Studier-Fischer S2, Swing T1, Grützner PA2 and Biglari B2 1Trauma & Reconstructive Surgery, University hospital Heidelberg, Germany 2BG Unfallklinik, Ludwigshafen, Germany *Corresponding author: Prof. Dr. med. Arash Moghaddam, Consultant Orthopaedic & Trauma Surgeon Center of Trauma, Orthopaedics & Paraplegiology, Division of Trauma & Reconstructive Surgery, University hospital Heidelberg, Schlierbacher Landstraße 200a, 69118 Heidelberg, Germany, Tel: 0049-6221-5626263, Fax: 0049- 6221-26298, E-mail: [email protected] to a high percentage of associated injuries [6]. The combination of a Abstract dislocated fracture and unstable joint makes operative treatment as Background: Radial head fractures are responsible for 2 to 5% of well as early mobilization difficult. Other treatment options include adult fractures. Especially problematic is the treatment of dislocated the implantation of a radial head prosthesis and resection of the and unstable fractures which often have a worst prognosis. The radial head. The radial head prosthesis has become established as the purpose of this study was to evaluate the results of open reduction choice of treatment for multi-fragmented radial head fractures with and internal fixation (ORIF) in the treatment of radial head fractures. associated injuries, while resection of the radial head has increasingly Materials and Methods: Between June 2001 and January 2006, fallen out of use and is now reserved for isolated fractures of the 41 reconstructive surgical procedures were executed. Thirty-seven radial head without associated injuries [7]. -

Del Vecchio Upper Extremity Injury
UPPER EXTREMITY INJURIES Jeff Del Vecchio MPAS, PA-C, DFAAPA Mercy Clinic Orthopedics Springfield, Missouri OBJECTIVES IDENTIFY COMMON UPPER EXTREMITY INJURIES AND FRACTURES REVIEW EXAMINATION TECHNIQUES FOR COMMON UPPER EXTREMITY INJURIES DISCUSS AND REVIEW RADIOGRAPHIC FINDINGS OF UPPER EXTREMITY FRACTURES DISCUSS AND REVIEW TREATMENT OPTIONS FOR COMMON UPPER EXTREMITY INJURIES LATERAL EPICONDYLITIS Tennis elbow Definition Pain about lateral aspect of elbow Involves extensor musculature Rotation of arm and wrist extension Secondary to repetitive overuse or injury Microtears to tendon⇒ inflammation⇒fibrosis⇒degeneration Affects pt’s 30-60 yrs Clinical symptoms Outside elbow and back of upper forearm pain Pain lifting with palm facing down Holding lightweight objects difficult Physical Examination Lateral epicondylar area tender to palpation Tennis elbow test- elbow 90 deg, extend wrist against resistance. +pain at lateral epicondaylar area Radiographs Obtain to rule out osteoarthritis or calcifications Treatment NSAID’s (10-14 days) Avoid activities causing pain Heat or ice Corticosteroid injection Stretching and gradual strengthening program Tennis elbow strap MEDIAL EPICONDYLITIS Golfer’s elbow Definition Inflammation of flexor-pronator’s Less common than lateral epicondylitis Clinical Symptoms Medial elbow pain Physical Examination Pain with palpation over medial condyle Pain with flexion and pronation of wrist against resistance Rule out ulnar neuropathy Treatment Same as lateral epicondylitis CLAVICLE FRACTURE Most common bone injury -
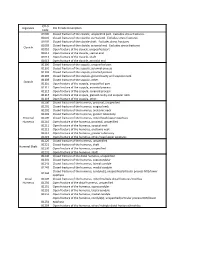
ICD*9, Diganosis ICD*9,Code,Description Code 81000 Closed,Fracture,Of,The,Clavicle,,Unspecified,Part.,,Excludes,Stress,Fractures
ICD*9, Diganosis ICD*9,Code,Description Code 81000 Closed,fracture,of,the,clavicle,,unspecified,part.,,Excludes,stress,fractures. 81001 Closed,fracture,of,the,clavicle,,sternal,end.,,Excludes,stress,fractures. 81002 Closed,fracture,of,the,clavicle,shaft.,,Excludes,stress,fractures. 81003 Closed,fracture,of,the,clavicle,,acromial,end.,,Excludes,stress,fractures. Clavicle 81010 Open,fracture,of,the,clavicle,,unspecified,part 81011 Open,fracture,of,the,clavicle,,sternal,end 81012 Open,fracture,of,the,clavicle,,shaft 81013 Open,fracture,of,the,clavicle,,acromial,end 81100 Closed,fracture,of,the,scapula,,unspecified,part 81101 Closed,fracture,of,the,scapula,,acromial,process 81102 Closed,fracture,of,the,scapula,,coracoid,process 81103 Closed,fracture,of,the,scapula,,glenoid,cavity,and,scapular,neck 81109 Closed,fracture,of,the,scapula,,other. Scapula 81110 Open,fracture,of,the,scapula,,unspecified,part 81111 Open,fracture,of,the,scapula,,acromial,process 81112 Open,fracture,of,the,scapula,,coracoid,process 81113 Open,fracture,of,the,scapula,,glenoid,cavity,and,scapular,neck 81119 Open,fracture,of,the,scapula,,other. 81200 Closed,fracture,of,the,humerus,,proximal,,unspecified 81201 Closed,fracture,of,the,humerus,,surgical,neck 81202 Closed,fracture,of,the,humerus,,anatomic,neck 81203 Closed,fracture,of,the,humerus,,greater,tuberosity Proximal, 81209 Closed,fracture,of,the,humerus,,other/head/upper,epiphysis Humerus 81210 Open,fracture,of,the,humerus,,proximal,,unspecified 81211 Open,fracture,of,the,humerus,,surgical,neck 81212 Open,fracture,of,the,humerus,,anatomic,neck -
Radial Head Fracture Repair and Rehabilitation
1 Radial Head Fracture Repair and Rehabilitation Surgical Indications and Considerations Anatomical Considerations: The elbow is a complex joint due to its intricate functional anatomy. The ulna, radius and humerus articulate in such a way as to form four distinctive joints. Surrounding the osseous structures are the ulnar collateral ligament complex, the lateral collateral ligament complex and the joint capsule. Four main muscle groups provide movement: the elbow flexors, the elbow extensors, the flexor-pronator group, and the extensor-supinator groups. Different types of radial head fractures can occur each of which has separate surgical indications and considerations. Fractures of the proximal one-third of the radius normally occur in the head region in adults and in neck region in children. The most recognized and used standard for assessing radial head fractures is the 4-part Mason classification system. It is used for both treatment and prognosis. Classification: Type I fracture A fissure or marginal fracture without displacement. Type II fracture Marginal fractures with displacement involving greater than 2 mm displacement. Type III fracture Comminuted fractures of the whole radial head. Type IV fracture (variation) A comminuted fracture, with an associated dislocation, ligament injury, coronoid fracture, or Monteggia lesion. Pathogenesis: Severe comminuted fractures or fracture dislocations of the head of the radius often occur as the result of a fall on an outstretched arm with the distal forearm angled laterally, or a valgus stress on the elbow. Fractures can also occur from a direct blow or force to the elbow (e.g. MVA). Chronic synovitis and mild deterioration of the articular surfaces associated with arthritis (e.g. -

Shoulder Shoulder
SHOULDER SHOULDER ⦿ Connects arm to thorax ⦿ 3 joints ◼ Glenohumeral joint ◼ Acromioclavicular joint ◼ Sternoclavicular joint ⦿ https://www.youtube.com/watch?v=rRIz6oO A0Vs ⦿ Functional Areas ◼ scapulothoracic ◼ scapulohumeral SHOULDER MOVEMENTS ⦿ Global Shoulder ⦿ Arm (Shoulder Movement Joint) ◼ Elevation ◼ Flexion ◼ Depression ◼ Extension ◼ Abduction ◼ Abduction ◼ Adduction ◼ Adduction ◼ Medial Rotation ◼ Medial Rotation ◼ Lateral Rotation ◼ Lateral Rotation SHOULDER MOVEMENTS ⦿ Movement of shoulder can affect spine and rib cage ◼ Flexion of arm Extension of spine ◼ Extension of arm Flexion of spine ◼ Adduction of arm Ipsilateral sidebending of spine ◼ Abduction of arm Contralateral sidebending of spine ◼ Medial rotation of arm Rotation of spine ◼ Lateral rotation of arm Rotation of spine SHOULDER GIRDLE ⦿ Scapulae ⦿ Clavicles ⦿ Sternum ⦿ Provides mobile base for movement of arms CLAVICLE ⦿ Collarbone ⦿ Elongated S shaped bone ⦿ Articulates with Sternum through Manubrium ⦿ Articulates with Scapula through Acromion STERNOCLAVICULAR JOINT STERNOCLAVICULAR JOINT ⦿ Saddle Joint ◼ Between Manubrium and Clavicle ⦿ Movement ◼ Flexion - move forward ◼ Extension - move backward ◼ Elevation - move upward ◼ Depression - move downward ◼ Rotation ⦿ Usually movement happens with scapula Scapula Scapula ● Flat triangular bone ● 3 borders ○ Superior, Medial, Lateral ● 3 angles ○ Superior, Inferior, Lateral ● Processes and Spine ○ Acromion Process, Coracoid Process, Spine of Scapula ● Fossa ○ Supraspinous, Infraspinous, Subscapularis, Glenoid SCAPULA -

Right Or Left Bones? Clavicle Ulna
Right or Left Bones? Clavicle Ulna . Together, the clavicles make a . Lay the ulna on the table. “handlebar” shape (low at the middle . Can you see the radial notch? of the chest, higher near the shoulders). o If yes, the open side of the . The blunt tip (sternal end) touches the trochlear (semilunar) notch tells sternum at the middle of the chest. you the bone orientation (see . The round tip (acromial end) touches the photo 1). scapula at the shoulder. o If no, the open side of the . The bumpy side of the clavicle faces the trochlear (semilunar) notch is the rib cage. opposite of the bone orientation . The smooth side of the clavicle faces (see photo 2). outward Radius Fibula . The styloid process always touches the . The smoother tip (head of the fibula) thumb. touches the knee. If the lower end of the radius (near the . The rougher tip (lateral malleolus) styloid process) is rough, you are touches the ankle. looking at the back of the wrist. The point of the lateral malleolus points . If the lower end of the radius is smooth, to the pinkie toe, not the middle of the you are looking at the inside of the wrist. foot. The front of the fibula (anterior view) has an edge. The back of the fibula (posterior view) is flat. References: University of Liverpool Faculty of Health and Life Sciences. (2013). Radius and ulna (right forearm) [Digital photograph]. Retrieved from https://www.flickr.com/photos/liverpoolhls/10819145494. . -

Upper Extremity Scapula
Lab 6 FUNCTIONAL HUMAN ANATOMY LAB #6 UPPER/LOWER EXTREMITY OSTEOLOGY OSTEOLOGY: UPPER EXTREMITY SCAPULA: Borders: Medial (Vertebral) - most superior aspect called the Superior angle Lateral - most inferior aspect called the inferior angle Fossa: Supraspinous fossa Infraspinous fossa Subscapular fossa Glenoid fossa Other Features: acromion process coracoid process scapular spine scapular notch infraglenoid tubercle - located at the bottom of the glenoid fossa supraglenoid tubercle - located at the top of the glenoid fossa Note: the shape of the Glenoid fossa suggests that shoulder stability is heavily reliant on connective tissues surrounding the joint to prevent dislocation CLAVICLE: sternal end - blunt, articulates with the Manubrium acromial end - flat/bladelike, articulates with the Acromium process HUMERUS: head greater tubercle lesser tubercle interturbicular (bicipital) groove - located between the tubercles deltoid tuberosity shaft medial/lateral epicondyles capitulum - the part of the distal condyle that articulates with the Radius trochlea - the part of the distal condyle that articulates with the Ulna olecranon fossa coronoid fossa ULNA: 1 Lab 6 coronoid process olecranon process trochlear notch ulnar tuberosity body head (distal end) radial notch - where the proximal end of the radius articulates interosseous border (lateral side) styloid process RADIUS: body neck head (proximal end) radial tuberosity anterior oblique line interosseous border styloid process CARPAL BONES # of rows? # of bones? Which carpal primarily articulates