Alberta Health Annual Report 2012/13
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CALGARY Zone NEWS Zone
CALGARY Zone NEWS Zone Your HealtH Care in Your CommunitY 2016 january “IT’s comforTIng To Have sage sIT on my lap anD be surrounDeD by all HIs Toys wHIle He’s geTTIng TreaTmenT – Calgary mom Hilary Daum easy care calgary oncology nurse shelaine semmens gives sage amor, age three, a chemotherapy treatment in the comfort of his own home as mom Hilary Daum holds him close. The service is part of a pilot project called Janet Mezzarobba photo | Hospital at Home. PAGE 3 insPirEd tEchnoloGy wE lovE thE niGhtlifE hElPs PrEEmiEs – All Across AlbErtA researchers at foothills medical centre have what to do on a long winter’s night? get outside, that’s developed a state-of-the-art device that allows what! There’s no better way to kick off those new newly-born premature babies to get critical medical year’s resolutions than by getting active when the stars attention while remaining connected to are out. Here are our suggestions for their umbilical cords. PAGE 4 some great winter workouts. PAGE 6 START HEALTHY. STAY HEALTHY. Influenza has arrived in Alberta. If you haven’t been immunized yet this season, you and your loved ones are at risk. The good news? It’s not too late. Influenza immunization is still available, free of charge. Start your year healthy, and stay that way. GET IMMUNIZED. WHY CHANCE IT? #whychanceit? www.ahs.ca/influenza | Call Health Link 811 File Name: AHS_ZoneNews_StartHealthy4C_10x3_Dec1 Publication: Zone News 202, 12225 – 105 Avenue, Edmonton, AB T5N 0Y3 Campaign: AHS Influenza Immunization campaign fall 2015 P: 780-702-9888 WWW.KICKMEDIA.CA Date completed: Nov 30, 2015 Format: PDF Size: 10" x 3" Pages: 1 Publication deadline: Dec 1, 2015 Colour: Color Application: InDesign CC Print ready: Yes Run date: December 2015 Bleed: None Draft: 1 PAGE 2 l o C a l l e a d e r s Donna Sharman, who after her stroke spent time recovering in Room 1033 of the Foothills Hospital stroke unit, now regularly visits patients on the unit as a volunteer peer supporter. -

Report on Operations INFRASTRUCTURE
Report on Operations INFRASTRUCTURE Our extensive global experience in the planning, development and operation of a full range of infrastructure projects allows us to provide engineering, procurement, construction and construction management services for projects of all sizes. BUILDINGS Our design/build contract for the new LEED Silver-targeted acoustic concert hall of Montreal employs MCGILL UNIVERSITY state-of-the-art acoustic design that HEALTH CENTRE’S creates a building within a building. We GLEN CAMPUS — CANADA are also designing a LEED Platinum planetarium in Montreal based on our consortium’s award-winning design. In Ontario, we provided mechanical/electrical consulting for Bell Lightbox, new home to the Toronto International Film Festival. In France, we are designing Stade de France’s sound system and working with the Paris Prefecture de Police on a 1000-camera video surveillance system. Also in Paris, we are rebuilding the ZAC Eiffel commercial complex in a congested urban setting, and we are providing overall quality control for the construction of NATO’s new headquarters in Brussels. In Haiti, we conducted numerous post-earthquake infrastructure assessments for the World Bank, and in Libya, work began on Guryan Judicial City, the country’s fi rst detention centre to comply with international human rights standards. SNC-L A VALIN 2010 ANNU AL REPOR T VALIN AL REPOR A 2010 ANNU SNC-L 10 ARCHITECT: JP VIGUIER HEALTHCARE FACILITIES In Quebec, we are designing and building McGill University Health Centre’s Glen Campus, Canada’s largest healthcare facility, and nearing completion of Montérégie’s cancer clinic. In France, we were awarded an engineering contract at Émile Muller Hospital and a design, construction and 25 year O&M contract for the laboratories at the Université de Versailles Saint-Quentin-en-Yvelines. -

Backup of March 03 2015Web.Cdr
Bart introduced our main guest speaker, Debbie Dunwell who is the Program 1 Speaker February 24th Assistant in Volunteer Resources for the South Health Campus. South Health Campus Debbie Dunwell Debbi’'s career started in Oil & Gas and in Construction in Administration & Management roles. In 2008 she changed 2 Meeting Minutes February 24th career direction by DisCon 2015 Keynote Speaker Line-up volunteering at the Foothills Country Hospice where she worked for 5 years, and was instrumental in developing a 3 What’s Up !! very successful volunteer Gregor’s Goings-On program. She was part of hundreds of volunteers who brought quality of life to over 500 people during that time. Gregor’s Goings-On cont’d 4 She has now been at South Health Campus for 2 years, where she uses her South Health Campus Cont’d training in Palliative and Spiritual care, Grief and Bereavement care as well as Alzheimer’s and Dementia. She is passionate about volunteers and the role they Our Arch Supporters ... THANK YOU !! play in Health Care and in End of Life Care. She is hoping Rotarians will decide to volunteer time to this worthy effort. Debbie mentioned the South Health Campus opened in 2013 and now has 270 5 Chinook/Fairview Mentoring Program beds available, with this number to grow to 600. Actually they are already Rotary’s Impact overcrowded. The site is the size of 20 football fields. Eventually 20,000 people will work in the urban area surrounding the hospital. There will be a hotel, medical buildings, VIP movie theatre and restaurants where dinner and drinks will be available. -

Calgary Zone
CALGARY ZONE Service Name Special Designation Service Short Description Location Name Location Address Addiction Services - Adult Addiction and Mental A residential, long-term 1835 House 1835 27 Avenue SW Calgary Long-Term Residential Health treatment program for T2T 1H2 people with substance addiction. Addiction Services - Adult Addiction and Mental A residential, short-term (20 1835 House 1835 27 Avenue SW Calgary Residential Health to 42 days) intensive T2T 1H2 treatment program for adults with addiction issues. Addiction Services - Adult Addiction and Mental Provides support for people 1835 House 1835 27 Avenue SW Calgary Transitional Health who have are transitioning T2T 1H2 from addiction treatment back into daily life. Assessment and Treatment Addiction and Mental Assesses and treats people Addiction and Mental 205 3 Avenue Strathmore Services - Mental Health Health with mental health Health Clinic - Strathmore T1P 1K2 problems. Rural Addiction and Mental Addiction and Mental Provides therapy and Addiction and Mental 205 3 Avenue Strathmore Health Services Health services for individuals Health Clinic - Strathmore T1P 1K2 having addiction and / or mental health concerns and their families. Mental Health Urgent Care Addiction and Mental Offers mental health crisis Airdrie Community Health 604 Main Street S Airdrie Health assessment on a walk-in Centre T4B 3K7 basis. Assessment and Treatment Addiction and Mental Assesses and treats people Airdrie Provincial Building 104 1 Avenue NW Airdrie Services - Mental Health Health with mental health T4B 0R2 problems. Addiction Services - Addiction and Mental Provides alcohol, other Airdrie Provincial Building 104 1 Avenue NW Airdrie Prevention Health drugs, tobacco, and T4B 0R2 gambling prevention, and education services. -

Calgary Clergy Volunteer Contacts
Calgary Zone Volunteer Resources Contact Information Community or Facility Contact Email address Contact number Zone Manager Michele Rondot [email protected] (587) 779-2035 Patient Engagement Kirsten Hrup [email protected] (587) 779-2036 Linda Stilborn Alberta Children’s Hospital Lorne Freno [email protected] (403) 955-7997 Diane Arellano Foothills Medical Centre Marisa Boulet [email protected] (403) 944-1336 Ellie Shock Helen Fung Min Young Peter Lougheed Centre Diane Polesello [email protected] (403) 943-4760 Strathmore General Hospital Cathy Walling Steve Barnes Rockyview General Hospital Therese Hesla [email protected] (403) 943-3566 Bryanne Vergara Patrick Mulvihill South Health Campus Melissa Wannamaker [email protected] (403) 956-1224 Karen Cameron Ashley Hornaday Home Care Diane Polesello [email protected] (403) 803-0109 High River Grace Ledoux [email protected] (403) 652-0113 Oilfields General Hospital (Black Diamond) Robin Carnegie (403) 933-6564 Okotoks Community Care Centre (403) 995-2660 Didsbury General Hospital Dawna Faryna [email protected] (403) 910-2984 Airdrie Community Care Cochrane Community Care Updated: November 2015 Community or Facility Contact Email address Contact number Canmore General Hospital Lori McClain [email protected] (403) 678-7253 Banff Community Care (403) 762-2990 Claresholm Willow Creek Continuing Care Carmelle Steel [email protected] (403) 625-8632 Claresholm General Hospital Vulcan General Hospital Nanton Community -

Department of Surgery Annual Report 2010/2011 April 1, 2010 to March 31, 2011
/ DEPARTMENT OF SURGERY ANNUAL REPORT 2010/2011 APRIL 1, 2010 TO MARCH 31, 2011 TOGETHER, LEADING AND CREATING EXCELLENCE IN SURGICAL CARE ANNUAL REPORT 2010/2011 Report Designed, Compiled and Edited by Matthew Hayhurst, Christine Bourgeois and Andria Marin-Stephens All Content and Photography (Unless Otherwise Stated) Provided by Matthew Hayhurst We Wish to Thank all the Surgeons, Administrators and other team members, whose tremendous efforts made this report possible. Matthew Hayhurst No Part of this Publication may be reproduced, stored in, or introduced into a retrieval system, or transmitted in any form or by any means (electronic, mechanical, photocopying, recording or otherwise) without the prior written permission of the copyright owners. Mailing Address: Foothills Medical Centre 1403 - 29th Street N.W. Calgary, Alberta, T2N 2T9 ph: (403) 944-1697 fax: (403) 270-8409 [email protected] Copyright © 2011 Department of Surgery/University of Calgary. All Rights Reserved Page ii ANNUAL REPORT 2010/2011 TABLE OF CONTENTS This Year in the Department Message from Dr. John Kortbeek 1 Surgical Executive Team 2 About the Department 3 From the Office of Surgical Education 5 From the Office of Surgical Research 7 From the Office of Health Technology & Innovation 9 From the Office of the Safety Officer 11 Around the Hospital Remote Ultrasound 13 Mentorship Program 14 Our Faculty Clinical Research Award, Dr. Bryan Donnelly 15 South Health Campus (2011 Update) 16 Richmond Road Otolaryngology Clinic (now in full service) -

MTU IM Orientation
Junior Resident Medical Teaching Unit Orientation Document Foothills Medical Centre Peter Lougheed Centre Rockyview General Hospital South Health Campus Welcome to the Medical Teaching Unit (MTU) at the University of Calgary! You will receive a brief orientation on your first day depending on which site you are assigned to, but this is a detailed overview of the locations, schedules and expectations of the MTU. MTU is first and foremost a teaching unit. You will be part of a multidisciplinary team with various levels and areas of training. Formal teaching is scheduled at each site as per the schedule below. MTU patients are typically academically interesting, complex or too unstable for other services. Sometimes they are all three! Remember that your two priorities on the MTU are patient care and your education. Have fun! Last updated September 2016 A TYPICAL DAY ON THE MTU: Morning • Handover: Meet at 8 am sharp in the designated team rooms (see site specific section). Here you will meet your team, receive patient handover. • Print out a single spaced patient list and write the clerk / resident assigned for the day next to the patient name. Provide this list to the Unit Clerk (FMC Unit 36/PLC Unit 38/RGH Unit 93/SHC Unit 66). • Morning Report: site dependant • Review Admissions: Meet with your staff to review overnight admissions • See your patients: See patients in order from sickest >> those needing discharge >> least sick. Afternoon • Lunchtime Rounds: (site specific) • “Run the List” - Meet with your team in the afternoon to discuss the patient list (depending on the senior resident/staff, generally 2-3pm) • Follow up on any outstanding issues from the morning • Update Signout Tool: Update the electronic Sign-Out in SCM • Evening Handover: Meet the evening / overnight team at 5 pm for patient handover Teaching (Site Specific) • Educational Rounds are a strong tradition within the culture of MTU. -

APL Memo- Calgary Zone Outpatient Lab Closures in Acute Sites
MEMORANDUM DATE: April 15, 2020 TO: All Calgary Zone Clinical Trial and Research Study Teams FROM: Alberta Precision Laboratories RE: Urban Hospital Outpatient Labs KEY MESSAGES: Effective Thursday, April 16 the outpatient labs located at Alberta Children’s Hospital (ACH), Peter Lougheed Centre (PLC), Rockyview General Hospital (RGH) and South Health Campus (SHC) will be closed. Patients will be re-directed to community Patient Service Centres. Staff will be deployed as appropriate. The safety of vulnerable patient populations and staff in the urban hospitals is a priority as we respond to the COVID-19 pandemic. Closing outpatient laboratory collections within urban acute care sites will reduce the number of individuals entering these facilities, limiting the risk of COVID-19 transmission. An APL memo was distributed on March 25th, 2020 strongly recommending physicians cease ordering routine or non- essential lab work. This has already reduced volumes of patients attending outpatient collection locations. The postponement of elective surgery combined with the closure of most ambulatory clinics has already resulted in a decreased need for outpatient lab service. Re-directing lab collections for ambulatory and outpatients to community PSCs will limit traffic into acute care sites and allow for more appropriate physical distancing. ACTION REQUIRED AND COLLECTION PROCESS: Patients who continue to attend remaining ambulatory clinics at the hospital will have their urgent laboratory blood work collected by the onsite phlebotomy team. Tom Baker Cancer Centre patients will continue to receive service in the Special Services Building (SSB) outpatient lab at Foothills Medical Center (FMC) which will remain open. Clinical Trial and Research Study Patients who require KIT/ Research collections originally collected from an Urban Hospital Outpatient Lab will be redirected to go to the SSB Outpatient Lab located at the FMC. -

Join MCKENZIE YOUR Us! OFFICIAL TOWNE COMMUNITY NEWSLETTER for MCKENZIE TOWNE
PUBLISHED BY MIND’S DESIGN STUDIO SINCE 2012 CALL 403-203-9152 FOR ADVERTISING OPPORTUNITIES WWW.MINDSDESIGN.CA Join MCKENZIE YOUR Us! OFFICIAL TOWNE COMMUNITY NEWSLETTER FOR MCKENZIE TOWNE ACIRCULATION | 7700 HOMESb ANDout BUSINESSES TowneOCTOBER | 2015 Hello A u tu m n FUN IN THIS ISSUE!: HALLOWEEN SPOOKTACULAR! P8 WWW.MCKENZIETOWNE.COM We Direct Bill Your Insurance NOW OPEN 7 DAYS A WEEK FOR YOUR CONVENIENCE! CALL FOR INFO. ABOUT PROFESSIONAL $29 TEETH WHITENING! HIGHSTREET IN MCKENZIE TOWNE dental (403)236-1200 50 High St SE Calgary www.highstreetdental.com Hours: 7AM - 8PM New Patients & Children Welcome Dr. Jeff Seckinger and Associates, General Dentists White Fillings . Emergencies . Open Evenings Pg. 2 October 2015 Thank you for supporting your Community Association and your local businesses! McKENZIE TOWNE Community Association Your Official Community Newsletter Board of Directors October Birthday? You rarely learn by mistakes but you must avoid prolonged indecision. Those born in October must establish the Libra’s soul’s purpose to achieve balance, emotional, financial, and spiritual stability during the course of their lifetime. You must stand for yourself and learn decision making by following not only your rational mind but also your accurate Executive intuitions. President: Birthstone: Opal Planet: Venus Jaydel Gluckie Vice-president: Courtesy of Astrostar.com Shannon Lanigain Secretary: Published by: Pablita Thomas-Griffin Treasurer: Aysha Khaliq Directors Mind’s Design Stephaine Kusie, Jim Fitz-morris, SERVING COMMUNITY RESIDENTS, Lori Mayson, Shelley Waryk-Martin, COMMUNITY ASSOCIATIONS Adam Johnson, Jim Boyle & LOCAL BUSINESSES FOR OVER 11 YEARS! Address WWW.MINDSDESIGN.CA McKenzie Towne Community Association c/o McKenzie Towne Residential Association ADVERTISE YOUR BUSINESS TODAY! 40 Mckenzie Towne Blvd S.E. -
Changes to Operating Hours at South Health Campus YMCA
Frequently Asked Questions _______________________________________ Changes to Operating Hours at South Health Campus YMCA What changes are being made? Effective January 14, 2019, the operating hours of the South Health Campus will change to the following: Monday – Friday 5.30 am – 9:00 pm Weekends & Holidays 7:00 am – 5.30 pm * Workout areas will continue to close 30 minutes prior to closing hours Why are the hours changing? We have reviewed current usage patterns at South Health Campus YMCA and have determined that early mornings remain a popular workout time. However, late evening usage is limited. The new Brookfield YMCA at Seton (opening January 14, 2019) will offer additional amenities, programs and services not offered at the South Health Campus YMCA. To balance this and the limited late evening usage at South Health Campus YMCA, we believe we will be able to more efficiently serve the community at the Brookfield Residential YMCA in the late evenings. How does this impact AHS Staff who are YMCA Members? Alberta Health Services staff will continue to have 24hr access to the workout areas at the South Health Campus YMCA. However, after regular operational hours (identified above), the facility will not be staffed by the YMCA. Protective Services will continue to provide emergency support after hours. AHS staff who wish to have 24hr access should contact the YMCA Member Services team to schedule an orientation and set up card access. How does this impact YMCA Members who are not AHS staff? YMCA Members who are not AHS staff will need to access the South Health Campus YMCA during the new operational hours identified above. -

Bedside and Community: 50 Years of Contributions to the Health of Albertans by the University of Calgary
University of Calgary PRISM: University of Calgary's Digital Repository University of Calgary Press University of Calgary Press Open Access Books 2020-02 Bedside and Community: 50 Years of Contributions to the Health of Albertans by the University of Calgary University of Calgary Press Mansell, D., Stahnisch, F., & Larsson, P. (Eds.). (2020). Bedside and Community: 50 Years of Contributions to the Health of Albertans by the University of Calgary. Calgary, AB: University of Calgary Press. http://hdl.handle.net/1880/111577 book https://creativecommons.org/licenses/by-nc-nd/4.0 Downloaded from PRISM: https://prism.ucalgary.ca BEDSIDE AND COMMUNITY: 50 Years of EDITED BY Diana Mansell, Frank W. Stahnisch, and Paula Larsson Contributions to the Health of Albertans by the University of Calgary Edited by Diana Mansell, Frank W. Stahnisch, and Paula Larsson ISBN 978-1-77385-073-3 THIS BOOK IS AN OPEN ACCESS E-BOOK. It is an electronic version of a book that can be purchased in physical form through any bookseller or on-line retailer, or from our distributors. Please support this open access publication by requesting that your university purchase a print copy of this book, or by purchasing BEDSIDE and a copy yourself. If you have any questions, please contact us at COMMUNITY [email protected] 50 Years of Contributions to the Health of Albertans by the University of Calgary Cover Art: The artwork on the cover of this book is not open access and falls under traditional copyright provisions; it cannot be reproduced in any way without written permission of the artists and their agents. -
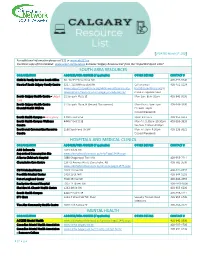
Calgary Resource Guide
UPDATED March 5th, 2020 For additional information please call 211 or www.ab.211.ca Electronic copy of this handout: www.scpcn.ca/resources & choose ‘Calgary Resource List’ from the “Important Quick Links” SOUTH AREA RESOURCES ORGANIZATION ADDRESS/WEB ADDRESS (If applicable) OTHER DETAILS CONTACT # Child & Family Services South Office 60, 10233 Elbow Drive SW 403‑297‑6240 Heart of South Calgary Family Centre 3217, 150 Millrise Blvd SW Call or email 403-452-1124 www.support.aspenfamily.org/what-we-do/community- [email protected] to development/heart-of-south-calgary-family-centre/ make an appointment South Calgary Health Centre - Urgent 31 Sunpark Plaza SE Mon-Sun: 8am-10pm 403-943-9300 Care South Calgary Health Centre 31 Sunpark Plaza SE (Second floor access) Mon-Thurs: 4pm-7pm 403-943-9300 Mental Health Walk-In Fri: 9am-12pm Closed Weekends South Health Campus – Emergency 4448 Front St SE Open 24 Hours 403-956-1111 South Health Campus Wellness 4448 Front St SE Mon-Fri: 5:30pm-10:30pm 403-956-3939 Centre Sat-Sun: 7:00am-8:30pm Southwest Communities Resource 2580 Southland Dr SW Mon-Fri: 9am-4:30pm 403-238-9222 Centre Closed Weekends HOSPITALS AND MEDICAL CLINICS ORGANIZATION ADDRESS/WEB ADDRESS (If applicable) OTHER DETAILS CONTACT # AHS Safeworks 1213 4th St SW Supervised Consumption Site www.albertahealthservices.ca/info/Page15434.aspx Alberta Children’s Hospital 2888 Shaganappi Trail NW 403-955-7211 Claresholm Care Centre 139 43 Avenue West, Claresholm, AB 403-682-3500 www.albertahealthservices.ca/services/page13575.aspx CUPS Medical Centre 1001 10 Ave SW 403-221-8797 Foothills Medical Center 1403 29 St NW 403-944-1110 Peter Lougheed Center 3500 26 Ave NE 403-943-4555 Rockyview General Hospital 7007 14 Street SW 403- 943-3000 Sheldon M.