The Surgery New Patient Health Questionnaire
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hythe Ward Hythe Ward
Cheriton Shepway Ward Profile May 2015 Hythe Ward Hythe Ward -2- Hythe Ward Foreword ..........................................................................................................5 Brief Introduction to area .............................................................................6 Map of area ......................................................................................................7 Demographic ...................................................................................................8 Local economy ...............................................................................................11 Transport links ..............................................................................................16 Education and skills .....................................................................................17 Health & Wellbeing .....................................................................................22 Housing .........................................................................................................33 Neighbourhood/community ..................................................................... 36 Planning & Development ............................................................................41 Physical Assets ............................................................................................ 42 Arts and culture ..........................................................................................48 Crime .......................................................................................................... -

66 the Street, Hawkinge, Folkestone, CT18 7DE EPC Rating: D £319,995
66 The Street, Hawkinge, Folkestone, CT18 7DE EPC Rating: D Part of £319,995 66 The Street Hawkinge, Folkestone A beautiful recently updated 3 bedroom detached bungalow with conservatory, large gardens and generous off road parking. Situation Services The property is ideally located within the popular, All main services are understood to be connected semi-rural village of Hawkinge Close by are a to the property. variety of amenities to include shops, Doctor's and Dental Surgeries, Pharmacies, Post Office and two Local Authority Primary Schools. Hawkinge also offers a range of Shepway District Council, Council Offices, Castle Leisure activities within the Village Hall and Hill Avenue, Folkestone, Kent, CT20 2QY. Community Centre. The village offers an extensive bus service running to Folkestone Town and The Cathedral City of Canterbury as well as the M20 Current Council Tax Band: D motorway and mainline railway service are both a short drive away, with the High Speed Link from Agents Note Folkestone to London St. Pancras via Ashford The property is ‘bought as seen’ and the Agents are running to some 53 minutes. unable to comment on the state and condition of any fixtures, fittings and appliances etc. The Property This spacious detached light and airy 3 bedroom bungalow has recently undergone major refurbishments to include a new modern kitchen, new fully tiled wet room and recent garage conversion. The property has been re-wired and a new Vaillant boiler installed. The double bedrooms are of a good size with the third currently being used as a study. The sitting room is double aspect with a central feature gas coal fire leading into the conservatory. -
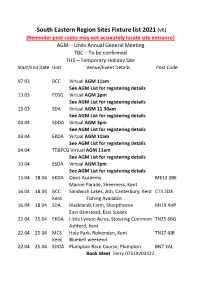
South Eastern Region Sites Fixture List 2021 (V6)
-South Eastern Region Sites Fixture list 2021 (v6) (Reminder post codes may not accurately locate site entrance} AGM – Units Annual General Meeting TBC – To be confirmed THS – Temporary Holiday Site Start/End Date Unit Venue/Event Details Post Code 07.03 BCC Virtual AGM 11am See AGM List for registering details 13.03 FDSG Virtual AGM 3pm See AGM List for registering details 13.03 SDA Virtual AGM 11.30am See AGM List for registering details 03.04 SDDA Virtual AGM 3pm See AGM List for registering details 03.04 EKDA Virtual AGM 11am See AGM List for registering details 04.04 TT&FCG Virtual AGM 11am See AGM List for registering details 10.04 ESDA Virtual AGM 2pm See AGM List for registering details 15.04 18.04 EKDA Oasis Academy ME12 2BE Marine Parade, Sheerness, Kent 16.04 18.04 BCC Sandwich Lakes, Ash, Canterbury, Kent CT3 2DA Kent Fishing Available 16.04 18.04 SDA Blacklands Farm, Sharpthorne RH19 4HP East Grinstead, East Sussex 22.04 25.04 EKDA Little Lynton Acres, Stowting Commom TN25 6BG Ashford, Kent 22.04 25.04 MCS Hole Park, Rolvenden, Kent TN17 4JB Kent Bluebell weekend 22.04 25.04 SDDA Plumpton Race Course, Plumpton BN7 3AL Book Meet Terry 07519203422 23.04 25.04 BCC Kent Fir Tree Farm, Rhodes Minnis, Kent CT4 6XR 29.04 04.05 MCS Orchard Farm, Chidham, Bosham PO18 8PP Southern West Sussex. PH/Bus close by BHM 29.04 03.05 EKDA Jemmet Farm, Mersham, Kent BHM TN25 7HB 29.04 04.05 MCS Kent Quex Park, Birchington, Kent BHM CT7 0BH 29.04 04.05 SDA Pierrepont Farm, Tilford, Surrey BHM GU10 3BS 29.04 03.05 ESDA Laughing Fish, Isfield, -

Flat 10, Birchwood House, Defiant Close, Hawkinge, Folkestone, CT18 7SU Price £172,000 Leasehold Part of EPC Rating: C
Flat 10, Birchwood House, Defiant Close, Hawkinge, Folkestone, CT18 7SU Price £172,000 Leasehold Part of EPC Rating: C Flat 10, Birchwood House Defiant Close, Hawkinge, Folkestone A well-presented new purpose built executive second floor apartment with two bedrooms and luxuriously fitted bathroom, along with a contemporary open plan sitting/dining room with well fitted kitchen situated in a popular location. Situation Defiant Close is ideally situated within the parking this superb apartment is most highly innovative development namely Terlingham Forum recommended. in the popular village of Hawkinge. Close by are a number of walks and rides over surrounding Outside countryside. The village of Hawkinge boasts a There is designated refuse storage with recycle large variety of essential amenities to include Tesco facilities and separate locked storage area for Express, Lidl Superstore, Two Pharmacies, Bank, personal belongings, together with enclosed gated Doctor’s, Dental Surgery, Two Primary Schools, area for parking small vehicles such as motor bikes Post Office and a new excellently equipped Care etc. Home. Leisure and socialising activities within the village include Community Centre, Village Hall, Mayfly Restaurant, The White Horse Public House, Services Cat and Custard Pot Public House, Indian and All main services are understood to be connected Chinese Take Away and several riding to the property. establishments. A bus service runs to both the coastal port of Folkestone to the south and, to the north via the A2, the Cathedral City of Canterbury. Local Authority Both offer excellent shopping, recreational and Shepway District Council, Council Offices, Castle educational facilities, as well as main line train Hill Avenue, Folkestone, Kent, CT20 2QY. -

Site Classification for Seismic Hazard Assessment in Low Seismicity Regions
Site Classification for Seismic Hazard Assessment in Low Seismicity Regions A thesis submitted in fulfilment of the requirements of the Doctor of Philosophy (PhD) degree and the Diploma of Imperial College (DIC) By Sarah Tallett-Williams Department of Civil and Environmental Engineering Imperial College London London SW7 2AZ September 2017 Declaration The work presented in this thesis was carried out in the Department of Civil and Environmental Engineering at Imperial College London. This thesis is the result of my own work and any quotation from, or description of the work of others is acknowledged herein by reference to the sources, whether published or unpublished. This thesis is not the same as any that I have submitted for any degree, diploma or other qualification at any other university. No part of this thesis has been or is being concurrently submitted for any such degree, diploma or other qualification. The copyright of this thesis rests with the author and is made available under a Creative Commons Attribution Non-Commercial No Derivatives licence. Researchers are free to copy, distribute or transmit the thesis on the condition that they attribute it, that they do not use it for commercial purposes and that they do not alter, transform or build upon it. For any reuse or redistribution, researchers must make clear to others the licence terms of this work. Sarah Tallett-Williams London, September 2017 1 Abstract Probabilistic Seismic Hazard Assessment of low seismicity regions has significant uncertainty due to the limited catalogue of earthquake records. Part of this uncertainty relates to the modification of ground motions by near-surface geo-materials: site amplification. -

The Folkestone School for Girls
Buses serving Folkestone School for Girls page 1 of 6 via Romney Marsh and Palmarsh During the day buses run every 20 minutes between Sandgate Hill and New Romney, continuing every hour to Lydd-on-Sea and Lydd. Getting to school 102 105 16A 102 Going from school 102 Lydd, Church 0702 Sandgate Hill, opp. Coolinge Lane 1557 Lydd-on-Sea, Pilot Inn 0711 Hythe, Red Lion Square 1618 Greatstone, Jolly Fisherman 0719 Hythe, Palmarsh Avenue 1623 New Romney, Light Railway Station 0719 0724 0734 Dymchurch, Burmarsh Turning 1628 St Mary’s Bay, Jefferstone Lane 0728 0733 0743 Dymchurch, High Street 1632 Dymchurch, High Street 0733 0738 0748 St. Mary’s Bay, Jefferstone Lane 1638 Dymchurch, Burmarsh Turning 0736 0741 0751 New Romney, Light Railway Station 1646 Hythe, Palmarsh Avenue 0743 0749 0758 Greatstone, Jolly Fisherman 1651 Hythe, Light Railway Station 0750 0756 0804 Lydd-on-Sea, Pilot Inn 1659 Hythe, Red Lion Square 0753 0759 0801 0809 Lydd, Church 1708 Sandgate Hill, Coolinge Lane 0806 C - 0823 Lydd, Camp 1710 Coolinge Lane (outside FSG) 0817 C - Change buses at Hythe, Red Lion Square to route 16A This timetable is correct from 27th October 2019. @StagecoachSE www.stagecoachbus.com Buses serving Folkestone School for Girls page 2 of 6 via Swingfield, Densole, Hawkinge During the daytime there are 5 buses every hour between Hawkinge and Folkestone Bus Station. Three buses per hour continue to Hythe via Sandgate Hill and there are buses every ten minutes from Folkestone Bus Station to Hythe via Sandgate Hill. Getting to school 19 19 16 19 16 Going -

Parish of Postling
PARISH OF POSTLING ANNUAL PARISH MEETING 2016 DRAFT Minutes of Postling Annual Parish Meeting held at Parish Village Hall on Wednesday 25 May 2016 starting at 7.30pm. PRESENT: Cllr Frank Hobbs (Chair), Cllr Christine Hobbs, Cllr John Elphick, Cllr Helen Calderbank, Jo Maher (Clerk), County District Councillor Susan Carey, KALC Chairman Ray Evison, Clive Adsett, Christine Webb, Tony Van Eldik, Marieke Van Eldik, Pat Elphick, Jan Wood, Derek Wood, Jenny Mannion 1) APOLOGIES: District Councillor Jenny Hollingsbee, Cllr John Pattrick, Cllr Charlie Wilkins, Cllr Jane Reynolds, Chris Reynolds, Gill Dixon 2) MINUTES OF THE PREVIOUS MEETING: The Minutes of the previous Annual Parish Meeting held on Wednesday 20 May 2015 were approved and signed by the Chair. This was proposed by Cllr Elphick, seconded by Cllr Christine Hobbs and unanimously agreed. 3) CHAIRMAN’s REPORT: Your Parish Council had another busy year. We are currently threatened by major developments in the area. The on-going consultation about the lorry park at Junction 11 was expected to report some time ago on the preferred site, but there is no news yet, and now probably won’t be released until after the referendum. This could have a knock-on effect on the sand extraction site if they chose Option 2. And now there is the proposal from Shepway DC for a “garden town” running on the southern side of the motorway from Junction 11 to the western edge of Sellindge, no doubt Cllr Carey will enlighten us more in her report. We have been invited to a meeting at SDC early next month, along with the other affected parishes, to be briefed fully on the proposed project. -

Agenda 4Th March 2019 Final Page to ALL COUNCILLORS 27Th
TO ALL COUNCILLORS 27th February 2019 THERE IS TO BE A MONTHLY MEETING OF THE ABOVE PARISH COUNCIL ON MONDAY 4th MARCH 2019. IT WILL BE HELD IN THE VILLAGE HALL STARTING 7.30pm. YOU ARE HEREBY SUMMOND TO ATTEND. THE AGENDA IS AS FOLLOWS: 41/19 To record those present and list any apologises. 42/19 To declare any Disclosable Pecuniary Interests (DPI), Other significant Interests (OSI’s) or a Voluntary interest relating to items on the agenda. A member who declares a DPI in relation to any item on the agenda will need to leave the meeting for the whole of that item and will not be able to speak or take part unless a relevant Dispensation has been granted. A member who declares an OSI will be able to speak on the item but will be required to leave the meeting for the vote. Councillors may also declare a voluntary interest if they are unsure of their position. Inclusion and voting will be decided at the time of the declaration, unless this has been discussed with the clerk prior to the meeting. 43/19 To note and agree minutes of a) The February 2019 PC meeting. b) The Extraordinary meeting February 2019. 44/19 To consider any matters arising from the Minutes not on the agenda elsewhere. 45/19 Core Strategy Review Submission Draft 1) To discuss and agree action. 46/19 Folkestone and Hythe Heritage Strategy Public Consultation 1) To discuss and agree action. 47/19 Public Contribution (For members of the public to ask questions – This item will last no more than 15 minutes) 1 . -
Some Problems of the North Downs Trackway in Kent
http://kentarchaeology.org.uk/research/archaeologia-cantiana/ Kent Archaeological Society is a registered charity number 223382 © 2017 Kent Archaeological Society SOME PROBLEMS OF THE NORTH DOWNS TRACKWAY IN KENT By REV. H. W. R. Liman, S.J., M.A.(0xon.) THE importance of this pre-historic route from the Continent to the ancient habitat of man in Wiltshire has long been recognized. In the Surrey Archceological Collections of 1964 will be found an attempted re-appraisal of its route through the county of Surrey. Although the problems connected with its passage through Kent are fewer owing to its being better preserved, there are some points which I think still deserve attention—the three river crossings of the Darenth, the Medway and the Stour; the crossing of the Elham valley; and the passage to Canterbury of the branch route from Eastwell Park, known as the Pilgrims' Way. It may be worth while, before dealing with the actual crossings, to note a few general characteristics. Mr. I. D. Margary—our most eminent authority on ancient roads in Britain—has pointed out the dual nature of this trackway. It com- prises a Ridgeway and a Terraceway. The first runs along the crest of the escarpment. The second runs parallel to it, usually at the point below the escarpment where the slope flattens out into cultivation. In Kent for the most part the Terraceway has survived more effectually than the Ridgeway. It is for much of its length used as a modern road, marked by the familiar sign 'Pilgrims' Way'. Except at its eastern terminus the Ridgeway has not been so lucky, although it can be traced fairly accurately by those who take the trouble to do so. -
A Guide to Parish Registers the Kent History and Library Centre
A Guide to Parish Registers The Kent History and Library Centre Introduction This handlist includes details of original parish registers, bishops' transcripts and transcripts held at the Kent History and Library Centre and Canterbury Cathedral Archives. There is also a guide to the location of the original registers held at Medway Archives and Local Studies Centre and four other repositories holding registers for parishes that were formerly in Kent. This Guide lists parish names in alphabetical order and indicates where parish registers, bishops' transcripts and transcripts are held. Parish Registers The guide gives details of the christening, marriage and burial registers received to date. Full details of the individual registers will be found in the parish catalogues in the search room and community history area. The majority of these registers are available to view on microfilm. Many of the parish registers for the Canterbury diocese are now available on www.findmypast.co.uk access to which is free in all Kent libraries. Bishops’ Transcripts This Guide gives details of the Bishops’ Transcripts received to date. Full details of the individual registers will be found in the parish handlist in the search room and Community History area. The Bishops Transcripts for both Rochester and Canterbury diocese are held at the Kent History and Library Centre. Transcripts There is a separate guide to the transcripts available at the Kent History and Library Centre. These are mainly modern copies of register entries that have been donated to the -

(Public Pack)Agenda Document for Governance Committee, 13/07
Despatched: 03.07.15 GOVERNANCE COMMITTEE 13 July 2015 at 6.00 pm Conference Room, Argyle Road, Sevenoaks AGENDA Membership : Chairman: Cllr. Pett Vice -Chairman: Cllr. Ms. Tennessee Cllrs. Dr. Canet, Clack, Halford, Layland and London Pages Contact Apologies for Absence 1. Minutes (Pages 1 - 4) To agree the Minutes of the meeting of the Committee held on 26 February 2015 as a correct record. 2. Declarations of Interest Any interest not already registered 3. Actions arising from the last meeting (if any) 4. Overview of Governance Committee (Pages 5 - 8) Christine Nuttall Tel: 01732 227245 5. The Local Authorities (Standing (Pages 9 - 20) Christine Nuttall Orders)(England)(Amendment) Regulations 2015 - Tel: 01732 227245 Appointment and Dismissal of Senior Officers 6. KCC Boundary Review - Response to Consultation (Pages 21 - 92) Christine Nuttall Tel: 01732 227245 7. Work Plan (Pages 93 - 94) EXEMPT ITEMS (At the time of preparing this agenda there were no exempt items. During any such items which may arise the meeting is likely NOT to be open to the public.) To assist in the speedy and efficient despatch of business, Members wishing to obtain factual information on items included on the Agenda are asked to enquire of the appropriate Contact Officer named on a report prior to the day of the meeting. Should you require a copy of this agenda or any of the reports listed on it in another format please do not hesitate to contact the Democratic Services Team as set out below. For any other queries concerning this agenda or the meeting please contact: The Democratic Services Team (01732 227241) Agenda Item 1 GOVERNANCE COMMITTEE Minutes of the meeting held on 26 February 2015 commencing at 7.00 pm Present : Cllr. -

NAME ADDRESS EMPTY START DATE Coral Estates Ltd 97
NAME ADDRESS EMPTY START DATE Coral Estates Ltd 97, Sandgate Road, Folkestone, Kent, CT20 2BQ EPRN 01/04/2008 Our Lady Of Fidelity Folkestone Trust St Marys Westbrook, Ravenlea Road, Folkestone, Kent, CT20 2JU EPRN 08/12/2008 Bede Property Investments Ltd Unit K, 9a, Lympne Industrial Park, Lympne, Hythe, Kent, CT21 4LR RV under 2600 01/04/2010 Industrial Investment Partnership Unit K, 9a, Lympne Industrial Park, Lympne, Hythe, Kent, CT21 4LR RV under 2600 01/04/2010 Irere Eagle 1 Ltd & Irere Eagle 2 Ltd Unit K, 9a, Lympne Industrial Park, Lympne, Hythe, Kent, CT21 4LR RV under 2600 01/04/2010 Schroder Exempt Prop Unit Trust Unit K, 9a, Lympne Industrial Park, Lympne, Hythe, Kent, CT21 4LR RV under 2600 01/04/2010 Schroder Exempt Prop Unit Trust Unit K, 9a, Lympne Industrial Park, Lympne, Hythe, Kent, CT21 4LR RV under 2600 01/04/2010 Dollond & Aitchison Limited 78a, Sandgate Road, Folkestone, Kent, CT20 2AA EPRN 01/04/2011 East Kent Housing 33, The Green, Burmarsh, Romney Marsh, Kent, TN29 0JL EPRN 01/04/2011 Eat.The Real Food Co. Ltd 12, Stop 24 Services & Port Early Arrivals, Junction 11 M20 Stanford Intersection, Stanford, Ashford, Kent, CT21 4BL EPRN 01/04/2011 Glengate (Folkestone) Ltd 1st Flr, 81-83, Sandgate Road, Folkestone, Kent, CT20 2AF EPRN 01/04/2011 Haag Juristen College (Cyprus Ltd) Ground Floor 80, Sidney Street, Folkestone, Kent, CT19 6HA EPRN 01/04/2011 Hsbc Bank Plc 353, Cheriton Road, Folkestone, Kent, CT19 4BP EPRN 01/04/2011 Irere Eagle 1 Ltd & Irere Eagle 2 Ltd Unit 7 2nd Floor, Dyna House, Lympne Industrial Park,