2008 Floods Health Cluster Response Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Mozambican National Resistance (Renamo) As Described by Ex-Patticipants
The Mozambican National Resistance (Renamo) as Described by Ex-patticipants Research Report Submitted to: Ford Foundation and Swedish International Development Agency William Minter, Ph.D. Visiting Researcher African Studies Program Georgetown University Washington, DC March, 1989 Copyright Q 1989 by William Minter Permission to reprint, excerpt or translate this report will be granted provided that credit is given rind a copy sent to the author. For more information contact: William Minter 1839 Newton St. NW Washington, DC 20010 U.S.A. INTRODUCTION the top levels of the ruling Frelirno Party, local party and government officials helped locate amnestied ex-participants For over a decade the Mozambican National Resistance and gave access to prisoners. Selection was on the basis of the (Renamo, or MNR) has been the principal agent of a desuuctive criteria the author presented: those who had spent more time as war against independent Mozambique. The origin of the group Renamo soldiers. including commanders, people with some as a creation of the Rhodesian government in the mid-1970s is education if possible, adults rather than children. In a number of well-documented, as is the transfer of sponsorship to the South cases, the author asked for specific individuals by name, previ- African government after white Rhodesia gave way to inde- ously identified from the Mozambican press or other sources. In pendent Zimbabwe in 1980. no case were any of these refused, although a couple were not The results of the war have attracted increasing attention geographically accessible. from the international community in recent years. In April 1988 Each interview was carried out individually, out of hearing the report written by consultant Robert Gersony for the U. -

Projectos De Energias Renováveis Recursos Hídrico E Solar
FUNDO DE ENERGIA Energia para todos para Energia CARTEIRA DE PROJECTOS DE ENERGIAS RENOVÁVEIS RECURSOS HÍDRICO E SOLAR RENEWABLE ENERGY PROJECTS PORTFÓLIO HYDRO AND SOLAR RESOURCES Edition nd 2 2ª Edição July 2019 Julho de 2019 DO POVO DOS ESTADOS UNIDOS NM ISO 9001:2008 FUNDO DE ENERGIA CARTEIRA DE PROJECTOS DE ENERGIAS RENOVÁVEIS RECURSOS HÍDRICO E SOLAR RENEWABLE ENERGY PROJECTS PORTFOLIO HYDRO AND SOLAR RESOURCES FICHA TÉCNICA COLOPHON Título Title Carteira de Projectos de Energias Renováveis - Recurso Renewable Energy Projects Portfolio - Hydro and Solar Hídrico e Solar Resources Redação Drafting Divisão de Estudos e Planificação Studies and Planning Division Coordenação Coordination Edson Uamusse Edson Uamusse Revisão Revision Filipe Mondlane Filipe Mondlane Impressão Printing Leima Impressões Originais, Lda Leima Impressões Originais, Lda Tiragem Print run 300 Exemplares 300 Copies Propriedade Property FUNAE – Fundo de Energia FUNAE – Energy Fund Publicação Publication 2ª Edição 2nd Edition Julho de 2019 July 2019 CARTEIRA DE PROJECTOS DE RENEWABLE ENERGY ENERGIAS RENOVÁVEIS PROJECTS PORTFOLIO RECURSOS HÍDRICO E SOLAR HYDRO AND SOLAR RESOURCES PREFÁCIO PREFACE O acesso universal a energia em 2030 será uma realidade no País, Universal access to energy by 2030 will be reality in this country, mercê do “Programa Nacional de Energia para Todos” lançado por thanks to the “National Energy for All Program” launched by Sua Excia Filipe Jacinto Nyusi, Presidente da República de Moçam- His Excellency Filipe Jacinto Nyusi, President of the -

Manica Province
Back to National Overview OVERVIEW FOR MANICA PROVINCE Tanzania Zaire Comoros Malawi Cabo Del g ad o Niassa Zambia Nampul a Tet e Manica Zambezi a Manica Zimbabwe So f al a Madagascar Botswana Gaza Inhambane South Africa Maput o N Swaziland 200 0 200 400 Kilometers Overview for Manica Province 2 The term “village” as used herein has the same meaning as “the term “community” used elsewhere. Schematic of process. MANICA PROVINCE 678 Total Villages C P EXPERT OPINION o m l COLLECTION a n p n o i n n e g TARGET SAMPLE n t 136 Villages VISITED INACCESSIBLE 121 Villages 21 Villages LANDMINE- UNAFFECTED BY AFFECTED NO INTERVIEW LANDMINES 60 Villages 3 Villages 58 Villages 110 Suspected Mined Areas DATA ENTERED INTO D a IMSMA DATABASE t a E C n o t r m y p a MINE IMPACT SCORE (SAC/UNMAS) o n n d e A n t n a HIGH IMPACT MODERATE LOW IMPACT l y 2 Villages IMPACT 45 Villages s i s 13 Villages FIGURE 1. The Mozambique Landmine Impact Survey (MLIS) visited 9 of 10 Districts in Manica. Cidade de Chimoio was not visited, as it is considered by Mozambican authorities not to be landmine-affected. Of the 121 villages visited, 60 identified themselves as landmine-affected, reporting 110 Suspected Mined Areas (SMAs). Twenty-one villages were inaccessible, and three villages could not be found or were unknown to local people. Figure 1 provides an overview of the survey process: village selection; data collection; and data-entry into the Information Management System for Mine Action (IMSMA) database, out of which is generated the Mine Impact Score (Appendix I). -

Floods, Food Security
ANNUAL REPORT OF THE HUMANITARIAN/RESIDENT COORDINATOR ON THE USE OF CERF GRANTS Country Mozambique Humanitarian / Resident Mr. Ndolamb Ngokwey Coordinator Reporting Period 1 January-31 December 2008 I. Executive Summary Mozambique is persistently hit by frequent natural disasters which inflict major damage and as a result, set back economic growth. Natural disasters such as floods, cyclones and droughts, continue to be the main obstacle for sustainable development and the achievement of the Millenium Developmental Goals (MDGs). The heavy rains in Mozambique and bordering countries from mid-December 2007 to mid- February 2008 flooded the Save, Buzi, Púngoè and Zambezi river basins in central Mozambique and have created flash floods around the Lugenda, Megaruna, Messalo and Montepuez rivers in the North of the country. Some 21,476 households (102,155 people) were affected by the 2008 Floods and 20 were reported dead. According to the National Institute for Disaster Management (INGC) 150,923 Ha of agricultural land were lost due to the 2008 floods. Following a Council of the Ministers meeting on 3January 2008, the National Institute for Disaster Management (INGC) declared a “Red Alert” later that afternoon. The Central Emergency Operations Centre (CENOE) was activated on 4 January 2008 and meetings with emergency focal points from the line ministries, relevant Government institutions and the Humanitarian Country Team members through the Cluster approach (WASH-water, Sanitation and Hygiene; Food Security; Logistics; Telecommunications; Shelter; Health; Protection; Education; Nutrition and Early Recovery) took place daily to provide updates on the situation and response in areas affected by the flooding. On 8 March 2008 the tropical cyclone “Jokwe” hit the coastland of Nampula and Zambezia, leaving behind a trail of destruction with a total of 40,339 households (201,695 people) affected, a death toll of 13 and 68,522 hectares of agricultural land destroyed. -
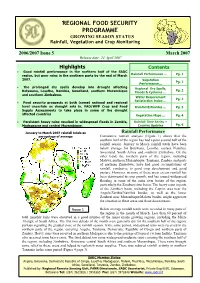
GROWING SEASON STATUS Rainfall, Vegetation and Crop Monitoring
REGIONAL FOOD SECURITY PROGRAMME GROWING SEASON STATUS Rainfall, Vegetation and Crop Monitoring 2006/2007 Issue 5 March 2007 Release date: 24 April 2007 Highlights Contents • Good rainfall performance in the northern half of the SADC region, but poor rains in the southern parts by the end of March Rainfall Performance … Pg. 1 2007. Vegetation Pg. 2 Performance… • The prolonged dry spells develop into drought affecting Regional Dry Spells, Pg. 2 Botswana, Lesotho, Namibia, Swaziland, southern Mozambique Floods & Cyclones … and southern Zimbabwe. Water Requirement Pg. 2 Satisfaction Index … • Food security prospects at both (some) national and regional level uncertain as drought sets in. FAO/WFP Crop and Food Rainfall Estimates … Pg. 3 Supply Assessments to take place in some of the drought affected countries Vegetation Maps … Pg. 4 • Persistent heavy rains resulted in widespread floods in Zambia, Rainfall Time Series + Madagascar and central Mozambique. Country Updates Pg. 6 January to March 2007 rainfall totals as Rainfall Performance percentage of average Cumulative rainfall analysis (Figure 1) shows that the southern half of the region has had a poor second half of the rainfall season. January to March rainfall totals have been below average for Botswana, Lesotho, eastern Namibia, Swaziland, South Africa and southern Zimbabwe. On the other hand, the northern parts of the region, including Malawi, northern Mozambique, Tanzania, Zambia, and parts of northern Zimbabwe, have had good accumulations of rainfall, conducive to good crop development and good pasture. However, in some of these areas excess rainfall has been detrimental to crop growth, and has caused widespread flooding in some of the main river basins of the region, particularly the Zambezi river basin. -

Manica District Development Project
Report Final Participatory Evaluation of the Manica District Development Project Nico Bakker, May 2011 INDEX LIST OF ABBREVIATIONS AND ACRONYMS ............................................................................ 3 EXECUTIVE SUMMARY .............................................................................................................. 4 1. INTRODUCTION AND CONTEXT OF THE PROJECT ......................................................... 6 1.1 Context of the project ..................................................................................................... 6 2. METHODS ............................................................................................................................ 9 2.1 Limitations of the Participatory Final Evaluation ........................................................... 11 3. SHORT DESCRIPTION OF THE PROJECT AND ITS EVOLUTION .................................. 13 3.1 Presentation of quantative and qualitative findings per activity ......................................... 16 3.1.1 Groups of horticulture producers 16 3.1.2 The groups of goat and chicken breeders 19 3.1.3 Accumulative Saving and Credit Association 22 3.1.4 Agrarian Bank 25 3.1.5 Local Consultative Councils (CCLs) 26 3.1.6 The Local Committees for the Management of Disaster Risks (CLGRC) 29 3.1.7 Cross cutting issues 30 4. RELEVANCE, EFFECTIVENESS, EFFICIENCY, IMPACT AND SUSTAINABILITY OF THE PROJECT .......................................................................................................................... -

Smallholder Irrigated Agriculture and Market Access Project
Public Disclosure Authorized Republic of Mozambique --------- Ministry of Agriculture and Food Security National Irrigation Institute Smallholder Irrigated Agriculture and Market Access Project Public Disclosure Authorized Resettlement Policy Framework (RPF) Public Disclosure Authorized Public Disclosure Authorized April, 2018 i LIST OF ACRONYMS AADAPT Agricultural Adaptations – World Bank Impact Evaluation Initiative ADIPSA Danish funded Rural Development Programme AIDS Acquired Immunodeficiency Syndrome ARA Regional Water Administration ARAP Abbreviated Resettlement Plan BP Bank Procedure DA District Administrator DINAS National Directorate of Agriculture and Forestry / Direcção Nacional de Agricultura e Silvicultura DPASA Provincial Directorate of Agriculture and Food Security / Direcção Provincial de Agricultura e Seguranca Alimentar DPTADER Provincial Directorate for Land, Environment and Rural Development Coordination / Direcção Provincial de Terra, Ambiente e Desenvolvimento Rural DPOPHRH Provincial Directorate of Public Works, Housing and Water Resources (Direcção Provincial de Obras Públicas, Habitação e Recursos Hídeicos) DPTADER Provincial Directorates for Coordination of Environmental Action (Direcções Provinciais de Terra, Ambiente e Desenvolvimento Rural) DUAT Right to Use and Benefit of the Land / Direito de Uso e Aproveito da Terra EA Environmental Assessment EDM State Electricity Company / Electricidade de Moçambique EIA Environmental Impact Assessment ESIA Environmental and Social Impact Assessment ESMF Environmental -
Final Report of the Needs Assessment
Assessment of the capacity of the health services to provide essential obstetric care in Tete province, Mozambique Final report of the needs assessment December 2000 1. INTRODUCTION Maternal mortality is a serious health problem in Mozambique. While the last census in 1997 and the DHS1 did not calculate exactly the maternal mortality ratio in the country, careful estimates indicate the MMR to be between 500 and 1500 deaths per 100 000 live births, but no reference is given. The only reliable information that is available comes from a sisterhood survey done in 19952. Even with these important differences in estimation of the exact figure of the maternal mortality, the problem is being recognised as an important one for the health planners and the donors in the country. Mozambique has made a clear commitment to reduce the maternal mortality in the country. In 1998 a first nation-wide Safe Motherhood needs asssesment3 was done, which was followed in the same year by a systematic review of the causes of 90 maternal deaths4. Following this dynamism within the ministry of health, a national strategy to reduce the maternal morbidity and mortality and neonatal mortality was formulated in 1999 and adopted in 2000, the document was launched as the: " …Estrategias para a redução da morbimortalidade materna e neonatal." This document 5forms the basis for formulating interventions to reduce maternal mortality in Mozambique. It is based on strengthening the health services with the concept of the provision of obstetric care ( basic and comprehensive) with an adequate referral system, community involvement and an improved data collection system. -

Baseline Survey
GCP/MOZ/079/BEL. Baseline Survey. November/December 2006 Baseline survey November/December 2006 GCP/MOZ/079/BEL Protecting and Improving Household Food security and Nutrition in HIV/AIDS affected areas of Manica and Sofala Province. FAO / Belgium Survival Fund Ministry of Agriculture in collaboration with the Ministry of Healt, Ministry of Education and Culture, Ministry of Women and Social Action and the Ministry of Planning and Development. 4 year project. 2005-2008. Support for technical assistance on questionnaire development and data analysis was provided by the FAO Nutrition and Consumer Protection Division through the EC/FAO Food Security Information for Action Programme, GCP/GLO/162/EC 1 GCP/MOZ/079/BEL. Baseline Survey. November/December 2006 Acknowledgements I would like to acknowledge the support given to the author of the report by Terri Ballard and Lorenza Mistura of the EC/FAO Programme who with unfailing good spirits continued to improve the analysis of the data from the baseline survey. I would also like to praise the enumerators who, despite difficult field conditions, produced a surprisingly clean set of questionnaires for analysis; giving us the confidence to draw conclusions from the information and hopefully take the discussion on how to develop a robust and practical measurement of food insecurity a step closer to conclusion. Kerry Selvester. [email protected]. Maputo, Mozambique May 2007 2 GCP/MOZ/079/BEL. Baseline Survey. November/December 2006 Glossary and Abbreviations BMI Body Mass Index EC European Community FANTA Food and Nutrition Technical Assistance Project FAO Food and Agriculture Organisation HFIAS Household Food Insecurity Access Scale HDDS Household Dietary Diversity Score IDDS Individual Dietary Diversity Score (IDDS) 3 GCP/MOZ/079/BEL. -

WFP Mozambique Situation Report #1
WFP Mozambique Situation Report #1 6 June 2016 Drought in Numbers Highlights A 90 day red alert was declared by the Government 1.5 million people acutely food insecure on 12 April as a result of the severe drought. and in need of immediate assistance At least 1.5 million people are acutely food insecure 6 of 11 provinces affected by the drought and in need of assistance in southern and central Resources available will allow WFP to reach areas of the country. 263,000 people from June until August 2016 Education authorities are already reporting an alarming surge of drop out in most drought affected areas. Funding Update Situation Update The harsh El Niño induced drought that hit Mozambique Humanitarian Country Team Strategic resulted in the deterioration of food security conditions in Response Plan the country and is expected to affect crops planted in late USD190.5 million January 2016. Immediate assistance has been provided to the most vulnerable populations since late 2015. > Food Security Cluster Food assistance Results of an assessment carried out by the Technical Secretariat for Food Security and Nutrition (SETSAN) last USD 150 million March show that at least 1,5 million people are affected > Nutrition Cluster by the drought in central (Zambezia, Manica, Sofala and USD 8,3 million Tete) and southern (Gaza, Inhambane and Maputo) provinces of the country. Staple food prices have increased by 100% and few WFP Drought Response Plan households still have cereal reserves for consumption. USD 96 million (12 months) Between November 2015 and March 2016, there was a * Not yet incorporated in PRRO 200355 sharp reduction in the quality of the diet. -

PROJECTS and AREAS of INTERVENTION CAM Operates in a Multi-Sectoral and Integrated Development Programme in Sofala Province, Central Mozambique
Consorzio Associazioni con il Mozambico (CAM) is an Italian NGO created in 2002 and headquartered in Trento but originally set up within an experience of decentralised cooperation between the Autonomous Province of Trento (PAT), situated in the northeastern part of Italy, and Caia district in the north of Sofala Province (Mozambique). The project was launched in 2000 in the framework of the Programme for Local Human Development that UNOPS (United Nations Organization for Project Service) was managing in Mozambique, with funds among others of the Italian Ministry of Foreign Affairs. This led to the signature of a cooperation agreement between PAT and the Province of Sofala in 2002, which was then updated in 2005. This was based on the construction of territorial partnerships and on the beginning of new cooperation relationships between decentralised entities and civil society actors in the two territories. CAM was officially founded in 2002 by five associations already operating in Mozambique. Since its establishment in 2002, the identity of CAM matched with a multisectoral community cooperation programme "Trentino in Mozambique - Mozambique in Trentino" that the organisation coordinated with and on behalf of the Autonomous Province of Trento in the districts of Caia and Marromeu. In the last few years, CAM expanded its geographical area of intervention in Central Mozambique. In particular, since 2016, CAM has been implementing various projects in Beira in the area of waste management and more recently water and sanitation. PROJECTS AND AREAS OF INTERVENTION CAM operates in a multi-sectoral and integrated development programme in Sofala Province, central Mozambique. The logic of this programme is to maximize the impact of sectoral interventions and achieve sustainable development at a local level. -

MASARYK UNIVERSITY BRNO Diploma Thesis
MASARYK UNIVERSITY BRNO FACULTY OF EDUCATION Diploma thesis Brno 2018 Supervisor: Author: doc. Mgr. Martin Adam, Ph.D. Bc. Lukáš Opavský MASARYK UNIVERSITY BRNO FACULTY OF EDUCATION DEPARTMENT OF ENGLISH LANGUAGE AND LITERATURE Presentation Sentences in Wikipedia: FSP Analysis Diploma thesis Brno 2018 Supervisor: Author: doc. Mgr. Martin Adam, Ph.D. Bc. Lukáš Opavský Declaration I declare that I have worked on this thesis independently, using only the primary and secondary sources listed in the bibliography. I agree with the placing of this thesis in the library of the Faculty of Education at the Masaryk University and with the access for academic purposes. Brno, 30th March 2018 …………………………………………. Bc. Lukáš Opavský Acknowledgements I would like to thank my supervisor, doc. Mgr. Martin Adam, Ph.D. for his kind help and constant guidance throughout my work. Bc. Lukáš Opavský OPAVSKÝ, Lukáš. Presentation Sentences in Wikipedia: FSP Analysis; Diploma Thesis. Brno: Masaryk University, Faculty of Education, English Language and Literature Department, 2018. XX p. Supervisor: doc. Mgr. Martin Adam, Ph.D. Annotation The purpose of this thesis is an analysis of a corpus comprising of opening sentences of articles collected from the online encyclopaedia Wikipedia. Four different quality categories from Wikipedia were chosen, from the total amount of eight, to ensure gathering of a representative sample, for each category there are fifty sentences, the total amount of the sentences altogether is, therefore, two hundred. The sentences will be analysed according to the Firabsian theory of functional sentence perspective in order to discriminate differences both between the quality categories and also within the categories.