CHAPTER 3 Structure and Function of the Auditory System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Guide to Sensory Processing.Pdf
Guide to Sensory Processing Prepared by Allison Travnik, MSOTS Level II Fieldwork Student Project Kavitha N Krishnan MS OTR/L Fieldwork Instructor Sensory Processing In order to understand what is going on around us, we need to organize all of the incoming sensory information (Ayres, 2005). The sensory information involves what we see, smell, taste, hear, feel on our body, where our body is in relation to others, and how well we are balanced. This is a lot of information that our brains need to process in order to engage in productive behavior, learn, and form accurate perceptions. Proprioceptive Where are body is in space Tactile Auditory What we feel The noise on our skin around us Sensory Smell Processing The Sight difference What we see scents around us around us Oral Sensory Processing Vestibular The sensations Jean Ayres developed the sensory Our sense of Disorder + balance that food give integration (SI) theory. SI gives us in our mouth meaning to what our senses are recognizing. When the sensations are not being organized properly may notice some of the same qualities in the brain, Ayres compared it to about yourself.It is important to a traffic jam. The traffic jam of remember that everyone has some sensory information can lead to quirks about their sensory processing learning difficulties and problem whether it be a sensitivity to loud behavior (Ayres, 2005). Children noises or dislike of light touch. with Sensory Processing Disorder However the identification of SPD is (SPD) are struggling with this reserved for individuals whose traffic jam. sensory quirks are outside of the Sensory processing is a typical range and affect their daily dynamic and complex theory. -

Perforated Eardrum
Vinod K. Anand, MD, FACS Nose and Sinus Clinic Perforated Eardrum A perforated eardrum is a hole or rupture m the eardrum, a thin membrane which separated the ear canal and the middle ear. The medical term for eardrum is tympanic membrane. The middle ear is connected to the nose by the eustachian tube. A perforated eardrum is often accompanied by decreased hearing and occasional discharge. Paih is usually not persistent. Causes of Eardrum Perforation The causes of perforated eardrum are usually from trauma or infection. A perforated eardrum can occur: if the ear is struck squarely with an open hand with a skull fracture after a sudden explosion if an object (such as a bobby pin, Q-tip, or stick) is pushed too far into the ear canal. as a result of hot slag (from welding) or acid entering the ear canal Middle ear infections may cause pain, hearing loss and spontaneous rupture (tear) of the eardrum resulting in a perforation. In this circumstance, there may be infected or bloody drainage from the ear. In medical terms, this is called otitis media with perforation. On rare occasions a small hole may remain in the eardrum after a previously placed P.E. tube (pressure equalizing) either falls out or is removed by the physician. Most eardrum perforations heal spontaneously within weeks after rupture, although some may take up to several months. During the healing process the ear must be protected from water and trauma. Those eardrum perforations which do not heal on their own may require surgery. Effects on Hearing from Perforated Eardrum Usually, the larger the perforation, the greater the loss of hearing. -

Understanding Sensory Processing: Looking at Children's Behavior Through the Lens of Sensory Processing
Understanding Sensory Processing: Looking at Children’s Behavior Through the Lens of Sensory Processing Communities of Practice in Autism September 24, 2009 Charlottesville, VA Dianne Koontz Lowman, Ed.D. Early Childhood Coordinator Region 5 T/TAC James Madison University MSC 9002 Harrisonburg, VA 22807 [email protected] ______________________________________________________________________________ Dianne Koontz Lowman/[email protected]/2008 Page 1 Looking at Children’s Behavior Through the Lens of Sensory Processing Do you know a child like this? Travis is constantly moving, pushing, or chewing on things. The collar of his shirt and coat are always wet from chewing. When talking to people, he tends to push up against you. Or do you know another child? Sierra does not like to be hugged or kissed by anyone. She gets upset with other children bump up against her. She doesn’t like socks with a heel or toe seam or any tags on clothes. Why is Travis always chewing? Why doesn’t Sierra liked to be touched? Why do children react differently to things around them? These children have different ways of reacting to the things around them, to sensations. Over the years, different terms (such as sensory integration) have been used to describe how children deal with the information they receive through their senses. Currently, the term being used to describe children who have difficulty dealing with input from their senses is sensory processing disorder. _____________________________________________________________________ Sensory Processing Disorder -

Experimental Studies on the Function of the Stapedius Muscle Inman
EXPERIMENTAL STUDIES ON THE FUNCTION OF THE STAPEDIUS MUSCLE INMAN AKADEMISK AVHANDLING som med vederbörligt tillstånd av Medicinska fakulteten vid Umeå Universitet för vinnande av medicine doktorsgrad offentligen försvaras i Samhällsvetarhuset, sal D, lördagen den 25 maj 1974 kl. 9.15 f.m. av JOHN-ERIK ZAKRISSON med.lic. UMEÅ 1974 UMEÀ UNIVERSITY MEDICAL DISSERTATIONS No. 18 1974 From the Department of Otorhinolaryngology, University of Umeå, Umeå, Sweden and the Division of Physiological Acoustics, Department of Physiology II, Karolinska Institutet, Stockholm, Sweden EXPERIMENTAL STUDIES ON THE FUNCTION OF THE STAPEDIUS MUSCLE IN MAN BY JOHN-ERIK ZAKRISSON UMEÂ 1974 To Karin Eva and Gunilla The present thesis is based on the following papers which will be referred to in the text by the Roman numerals: I. Zakrisson, J.-E., Borg, E. & Blom, S. The acoustic impedance change as a measure of stapedius muscle activity in man. A methodological study with electromyography. Acta Otolaryng, preprint. II. Borg, E. & Zakrisson, J.-E. Stapedius reflex and monaural masking. Acta Otolaryng, preprint. III. Zakrisson, J.-E. The role of the stapedius reflex in poststimulatory audi tory fatigue. Acta Otolaryng, preprint. IV. Borg, E. & Zakrisson, J.-E. The activity of the stapedius muscle in man during vocalization. Acta Otolaryng, accepted for publication. CONTENTS ABBREVIATIONS .......................................... 8 INTRODUCTION.............................................................................................. 9 MATERIAL..................................................................................................... -
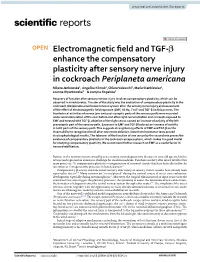
Electromagnetic Field and TGF-Β Enhance the Compensatory
www.nature.com/scientificreports OPEN Electromagnetic feld and TGF‑β enhance the compensatory plasticity after sensory nerve injury in cockroach Periplaneta americana Milena Jankowska1, Angelika Klimek1, Chiara Valsecchi2, Maria Stankiewicz1, Joanna Wyszkowska1* & Justyna Rogalska1 Recovery of function after sensory nerves injury involves compensatory plasticity, which can be observed in invertebrates. The aim of the study was the evaluation of compensatory plasticity in the cockroach (Periplaneta americana) nervous system after the sensory nerve injury and assessment of the efect of electromagnetic feld exposure (EMF, 50 Hz, 7 mT) and TGF‑β on this process. The bioelectrical activities of nerves (pre‑and post‑synaptic parts of the sensory path) were recorded under wind stimulation of the cerci before and after right cercus ablation and in insects exposed to EMF and treated with TGF‑β. Ablation of the right cercus caused an increase of activity of the left presynaptic part of the sensory path. Exposure to EMF and TGF‑β induced an increase of activity in both parts of the sensory path. This suggests strengthening efects of EMF and TGF‑β on the insect ability to recognize stimuli after one cercus ablation. Data from locomotor tests proved electrophysiological results. The takeover of the function of one cercus by the second one proves the existence of compensatory plasticity in the cockroach escape system, which makes it a good model for studying compensatory plasticity. We recommend further research on EMF as a useful factor in neurorehabilitation. Injuries in the nervous system caused by acute trauma, neurodegenerative diseases or even old age are hard to reverse and represent an enormous challenge for modern medicine. -

SENSORY MOTOR COORDINATION in ROBONAUT Richard Alan Peters
SENSORY MOTOR COORDINATION IN ROBONAUT 5 Richard Alan Peters 11 Vanderbilt University School of Engineering JSC Mail Code: ER4 30 October 2000 Robert 0. Ambrose Robotic Systems Technology Branch Automation, Robotics, & Simulation Division Engineering Directorate Richard Alan Peters II Robert 0. Ambrose SENSORY MOTOR COORDINATION IN ROBONAUT Final Report NASNASEE Summer Faculty Fellowship Program - 2000 Johnson Space Center Prepared By: Richard Alan Peters II, Ph.D. Academic Rank: Associate Professor University and Department: Vanderbilt University Department of Electrical Engineering and Computer Science Nashville, TN 37235 NASNJSC Directorate: Engineering Division: Automation, Robotics, & Simulation Branch: Robotic Systems Technology JSC Colleague: Robert 0. Ambrose Date Submitted: 30 October 2000 Contract Number: NAG 9-867 13-1 ABSTRACT As a participant of the year 2000 NASA Summer Faculty Fellowship Program, I worked with the engineers of the Dexterous Robotics Laboratory at NASA Johnson Space Center on the Robonaut project. The Robonaut is an articulated torso with two dexterous arms, left and right five-fingered hands, and a head with cameras mounted on an articulated neck. This advanced space robot, now dnven only teleoperatively using VR gloves, sensors and helmets, is to be upgraded to a thinking system that can find, in- teract with and assist humans autonomously, allowing the Crew to work with Robonaut as a (junior) member of their team. Thus, the work performed this summer was toward the goal of enabling Robonaut to operate autonomously as an intelligent assistant to as- tronauts. Our underlying hypothesis is that a robot can deveZop intelligence if it learns a set of basic behaviors ([.e., reflexes - actions tightly coupled to sensing) and through experi- ence learns how to sequence these to solve problems or to accomplish higher-level tasks. -

Instruction Sheet: Otitis Externa
University of North Carolina Wilmington Abrons Student Health Center INSTRUCTION SHEET: OTITIS EXTERNA The Student Health Provider has diagnosed otitis externa, also known as external ear infection, or swimmer's ear. Otitis externa is a bacterial/fungal infection in the ear canal (the ear canal goes from the outside opening of the ear to the eardrum). Water in the ear, from swimming or bathing, makes the ear canal prone to infection. Hot and humid weather also predisposes to infection. Symptoms of otitis externa include: ear pain, fullness or itching in the ear, ear drainage, and temporary loss of hearing. These symptoms are similar to those caused by otitis media (middle ear infection). To differentiate between external ear infection and middle ear infection, the provider looks in the ear with an instrument called an otoscope. It is important to distinguish between the two infections, as they are treated differently: External otitis is treated with drops in the ear canal, while middle ear infection is sometimes treated with an antibiotic by mouth. MEASURES YOU SHOULD TAKE TO HELP TREAT EXTERNAL EAR INFECTION: 1. Use the ear drops regularly, as directed on the prescription. 2. The key to treatment is getting the drops down into the canal and keeping the medicine there. To accomplish this: Lie on your side, with the unaffected ear down. Put three to four drops in the infected ear canal, then gently pull the outer ear back and forth several times, working the medicine deeper into the ear canal. Remain still, good-ear-side-down for about 15 minutes. -

Morphological and Functional Changes in a New Animal Model Of
Laboratory Investigation (2013) 93, 1001–1011 & 2013 USCAP, Inc All rights reserved 0023-6837/13 Morphological and functional changes in a new animal model of Me´nie`re’s disease Naoya Egami1, Akinobu Kakigi1, Takashi Sakamoto1, Taizo Takeda2, Masamitsu Hyodo2 and Tatsuya Yamasoba1 The purpose of this study was to clarify the underlying mechanism of vertiginous attacks in Me´nie`re’s disease (MD) while obtaining insight into water homeostasis in the inner ear using a new animal model. We conducted both histopatho- logical and functional assessment of the vestibular system in the guinea-pig. In the first experiment, all animals were maintained 1 or 4 weeks after electrocauterization of the endolymphatic sac of the left ear and were given either saline or desmopressin (vasopressin type 2 receptor agonist). The temporal bones from both ears were harvested and the extent of endolymphatic hydrops was quantitatively assessed. In the second experiment, either 1 or 4 weeks after surgery, animals were assessed for balance disorders and nystagmus after the administration of saline or desmopressin. In the first experiment, the proportion of endolymphatic space in the cochlea and the saccule was significantly greater in ears that survived for 4 weeks after surgery and were given desmopressin compared with other groups. In the second experiment, all animals that underwent surgery and were given desmopressin showed spontaneous nystagmus and balance disorder, whereas all animals that had surgery but without desmopressin administration were asymptomatic. Our animal model induced severe endolymphatic hydrops in the cochlea and the saccule, and showed episodes of balance disorder along with spontaneous nystagmus. -
Auditory System & Hearing
Auditory System & Hearing Chapters 9 part II Lecture 17 Jonathan Pillow Sensation & Perception (PSY 345 / NEU 325) Fall 2017 1 Cochlea: physical device tuned to frequency! • place code: tuning of different parts of the cochlea to different frequencies 2 The auditory nerve (AN): fibers stimulated by inner hair cells • Frequency selectivity: Clearest when sounds are very faint 3 Threshold tuning curves for 6 neurons (threshold = lowest intensity that will give rise to a response) Characteristic frequency - frequency to which the neuron is most sensitive threshold(dB) frequency (kHz) 4 Information flow in the auditory pathway • Cochlear nucleus: first brain stem nucleus at which afferent auditory nerve fibers synapse • Superior olive: brainstem region thalamus MGN in the auditory pathway where inputs from both ears converge • Inferior colliculus: midbrain nucleus in the auditory pathway • Medial geniculate nucleus (MGN): part of the thalamus that relays auditory signals to the cortex 5 • Primary auditory cortex (A1): First cortical area for processing audition (in temporal lobe) • Belt & Parabelt areas: areas beyond A1, where neurons respond to more complex characteristics of sounds 6 Basic Structure of the Mammalian Auditory System Comparing overall structure of auditory and visual systems: • Auditory system: Large proportion of processing before A1 • Visual system: Large proportion of processing after V1 7 Basic Structure of the Mammalian Auditory System Tonotopic organization: neurons organized spatially in order of preferred frequency • -

Status and Strategies Analysis on International Standardization of Auricular Acupuncture Points
Online Submissions:http://www.journaltcm.com J Tradit Chin Med 2013 June 15; 33(3): 408-412 [email protected] ISSN 0255-2922 © 2013 JTCM. All rights reserved. REVIEWTOPIC Status and strategies analysis on international standardization of auricular acupuncture points Lei Wang, Baixiao Zhao, Liqun Zhou aa Lei Wang, Baixiao Zhao, School of Acupuncture-Moxibus- Germany. Clinical AAP research was done in Italy, tion and Tuina, Beijing University of Chinese Medicine, Bei- Austria, Switzerland, Spain, the UK, Holland, Japan, jing 100029, China Russia, and Africa. However, AAP research was not Liqun Zhou, Department of Humanities of Traditional Chi- communicated internationally. The World Federa- nese Medicine, School of Basic Medical Sciences, Beijing Uni- tion of Acupuncture-Moxibustion Societies recom- versity of Chinese Medicine, Beijing 100029, China Supported by a Grant of Key Technology Standard Promo- mended international standard of auricular acu- tion Project (No. 2006BAK04A20) from the Ministry of Sci- puncture points (ISAAPs). Standardized nomencla- ence and Technology of China, and a Grant (No. 2009B26) ture and locations of AAPs would provide a solid from the World Federation of Acupuncture and Moxibustion basis to draft an international standard organiza- Societies tion. Correspondence to: Prof. Baixiao Zhao, School of Acu- puncture-Moxibustion and Tuina, Beijing University of Chi- CONCLUSION: Experts need to find common nese Medicine, Beijing 100029, China. baixiao100@gmail. points from different countries or regions, provide com evidence of different ideas, and list the proposal as Telephone: +86-10-64286737; +86-13911040781 a recommendation for an international standard. Accepted: January 27, 2013 © 2013 JTCM. All rights reserved. Abstract Key words: Acupuncture, ear; Reference standards; Information storage and retrieval OBJECTIVE: To supply literature for developing an international standard of auricular acupuncture points. -

Eardrum Regeneration: Membrane Repair
OUTLINE Watch an animation at: Infographic: go.nature.com/2smjfq8 Pages S6–S7 EARDRUM REGENERATION: MEMBRANE REPAIR Can tissue engineering provide a cheap and convenient alternative to surgery for eardrum repair? DIANA GRADINARU he eardrum, or tympanic membrane, forms the interface between the outside world and the delicate bony structures Tof the middle ear — the ossicles — that conduct sound vibrations to the inner ear. At just a fraction of a millimetre thick and held under tension, the membrane is perfectly adapted to transmit even the faintest of vibrations. But the qualities that make the eardrum such a good conductor of sound come at a price: fra- gility. Burst eardrums are a major cause of conductive hearing loss — when sounds can’t pass from the outer to the inner ear. Most burst eardrums are caused by infections or trauma. The vast majority heal on their own in about ten days, but for a small proportion of people the perforation fails to heal natu- rally. These chronic ruptures cause conductive hearing loss and group (S. Kanemaru et al. Otol. Neurotol. 32, 1218–1223; 2011). increase the risk of middle ear infections, which can have serious In a commentary in the same journal, Robert Jackler, a head complications. and neck surgeon at Stanford University, California, wrote that, Surgical intervention is the only option for people with ear- should the results be replicated, the procedure represents “poten- drums that won’t heal. Tympanoplasty involves collecting graft tially the greatest advance in otology since the invention of the material from the patient to use as a patch over the perforation. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists.