Special Focus on Government Experiences of CMAM Scale Up
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MZ 2-2016 Afrika V7 Final.Indd
ISSN 0259-7446 EUR 6,50 medienmedien Kommunikation in Vergangenheit und Gegenwart && zeitzeit Thema: Afrikanisch-Europäische Medienbeziehungen Imperiale Kommunikationsarbeit Von Lumumba bis Ebola Dekolonisierung des Blicks International News Reporting in the Multidimensional Network Against the Hypothesis of a China-EU Collaboration in Africa Research Corner: Eine Zeitung für Tibet 22/2016/2016 Jahrgang 31 m&z 2/2016 medien & zeit Impressum MEDIENINHABER, HERAUSGEBER UND VERLEGER Verein „Arbeitskreis für historische Kommunikationsforschung (AHK)“, Währinger Straße 29, 1090 Wien, Inhalt ZVR-Zahl 963010743 http://www.medienundzeit.at © Die Rechte für die Beiträge in diesem Heft liegen beim „Arbeitskreis für historische Kommunikationsforschung (AHK)“ HERAUSGEBERINNEN Barbara Metzler, Erik Bauer, Christina Krakovsky REDAKTION BUCHBESPRECHUNGEN Gaby Falböck, Roland Steiner, Thomas Ballhausen Imperiale Kommunikationsarbeit REDAKTION RESEARCH CORNER Zur medialen Rahmung von Mission im 19. Erik Bauer, Christina Krakovsky, Barbara Metzler, LEKTORAT & LAYOUT und 20. Jahrhundert Diotima Bertel, Julia Himmelsbach, Barbara Metzler, Judith Rosenkranz; Richard Hölzl 3 Diotima Bertel PREPRESS Grafikbüro Ebner, Wiengasse 6, 1140 Wien, Von Lumumba bis Ebola VERSAND ÖHTB – Österreichisches Hilfswerk für Taubblinde und Standarderzählungen in der österreichischen hochgradig Hör- und Sehbehinderte Afrika-Berichterstattung (1960-2015) Werkstätte Humboldtplatz 7, 1100 Wien, ERSCHEINUNGSWEISE & BEZUGSBEDINGUNGEN Martin Sturmer 18 medien & zeit erscheint vierteljährlich -
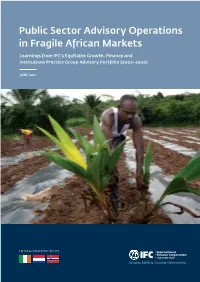
Public Sector Advisory Operations in Fragile African Markets
Public Sector Advisory Operations in Fragile African Markets Learnings from IFC’s Equitable Growth, Finance and Institutions Practice Group Advisory Portfolio (2002–2020) JUNE 2021 IN PARTNERSHIP WITH Disclaimer © International Finance Corporation [2021]. All rights reserved. 2121 Pennsylvania Avenue, N.W. Washington, D.C. 20433 Internet: www.ifc.org The material in this work is copyrighted. Copying and/or transmitting portions or all of this work without permission may be a violation of applicable law. IFC encourages dissemination of its work and will normally grant permission to reproduce portions of the work promptly, and when the reproduction is for educational and non- commercial purposes, without a fee, subject to such attributions and notices as we may reasonably require. IFC does not guarantee the accuracy, reliability, or completeness of the content included in this work, or the conclusions or judgments described herein, and accepts no responsibility or liability for any omissions or errors (including, without limitation, typographical errors and technical errors) in the content whatsoever or for reliance thereon. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. The findings, interpretations, and conclusions expressed in this volume do not necessarily reflect the views of the Executive Directors of The World Bank or the governments they represent. The contents of this work are intended for general informational purposes only and are not intended to constitute legal, securities, or investment advice, an opinion regarding the appropriateness of any investment, or a solicitation of any type. -

Jevgenia Viktorova Milne Phd Thesis
RETURNING CULTURE TO PEACEBUILDING: CONTESTING THE LIBERAL PEACE IN SIERRA LEONE Jevgenia Viktorova Milne A Thesis Submitted for the Degree of PhD at the University of St. Andrews 2009 Full metadata for this item is available in the St Andrews Digital Research Repository at: https://research-repository.st-andrews.ac.uk/ Please use this identifier to cite or link to this item: http://hdl.handle.net/10023/938 This item is protected by original copyright Jevgenia Viktorova Milne Returning Culture to Peacebuilding: Contesting the Liberal Peace in Sierra Leone PhD Thesis University of St Andrews School of International Relations 30 November 2009 2 I, Jevgenia Milne, hereby certify that this thesis, which is approximately 99,000 words in length, has been written by me, that it is the record of work carried out by me and that it has not been submitted in any previous application for a higher degree. I was admitted as a research student in September 2004 and as a candidate for the degree of PhD in September 2005; the higher study for which this is a record was carried out in the University of St Andrews between 2005 and 2009. date: 30 November 2009 signature of candidate ……………………. I hereby certify that the candidate has fulfilled the conditions of the Resolution and Regulations appropriate for the degree of ……… in the University of St Andrews and that the candidate is qualified to submit this thesis in application for that degree. date …………………………… signature of supervisor ……………………… In submitting this thesis to the University of St Andrews we understand that we are giving permission for it to be made available for use in accordance with the regulations of the University Library for the time being in force, subject to any copyright vested in the work not being affected thereby. -
What Role for Ethnicity? Political Behavior and Mobilization in Post-Conflict Sierra Leone and Liberia
Western Michigan University ScholarWorks at WMU Dissertations Graduate College 5-2010 What Role for Ethnicity? Political Behavior and Mobilization in Post-Conflict Sierra Leone and Liberia Fodei Joseph Batty Western Michigan University Follow this and additional works at: https://scholarworks.wmich.edu/dissertations Part of the Political Science Commons, and the Race and Ethnicity Commons Recommended Citation Batty, Fodei Joseph, "What Role for Ethnicity? Political Behavior and Mobilization in Post-Conflict Sierra Leone and Liberia" (2010). Dissertations. 501. https://scholarworks.wmich.edu/dissertations/501 This Dissertation-Open Access is brought to you for free and open access by the Graduate College at ScholarWorks at WMU. It has been accepted for inclusion in Dissertations by an authorized administrator of ScholarWorks at WMU. For more information, please contact [email protected]. WHAT ROLE FOR ETHNICITY? POLITICAL BEHAVIOR AND MOBILIZATION IN POST-CONFLICT SIERRA LEONE AND LIBERIA by Fodei Joseph Batty A Dissertation Submitted to the Faculty of The Graduate College in partial fulfillment of the requirements for the Degree of Doctor of Philosophy Department of Political Science Advisor: Jim Butterfield, Ph.D. Western Michigan University Kalamazoo, Michigan May 2010 UMI Number: 3410394 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. UMT Dissertation Publishing UMI 3410394 Copyright 2010 by ProQuest LLC. All rights reserved. -
Electoral Security Framework Technical Guidance Handbook for Democracy and Governance Officers
ELECTORAL SECURITY FRAMEWORK TECHNICAL GUIDANCE HANDBOOK FOR DEMOCRACY AND GOVERNANCE OFFICERS JULY 2010 This report was produced for review by the United States Agency for International Development. It was prepared by Creative Associates International, Inc.The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development (USAID) or the United States Government. TABLE OF CONTENTS ACKNOWLEDGEMENTS ......................................................................................................................................................1 EXECUTIVE SUMMARY ........................................................................................................................................................2 Electoral Security Assessment ...............................................................................................................................................................................................3 Electoral Security Planning ......................................................................................................................................................................................................3 Electoral Security Programming ...........................................................................................................................................................................................3 Monitoring and Evaluation ......................................................................................................................................................................................................4 -

Sierra Leone
Sierra Leone Factsheets of Health Statistics 2010 Figure 1 : Sierra Leone and neighboring countries Guinea Liberia Sierra Leone Figure 2 : Population size (in thousands) in Sierra Leone and neighboring countries, 2008 Sierra Leone 5,560 Guinea 9,833 Liberia 3,793 1. Health Status Life expectancy Figure 3 : Life expectancyi at birth in years, in Sierra Leone and neighboring countries, 2008 and 1990 2008 1990 49 Sierra Leone 41 54 Guinea 46 54 Liberia 36 53 African Region 51 Figure 4 : Life expectancy at birth in years, in Sierra Leone and neighboring countries, by sex, 2008 Male Female 48 Sierra Leone 50 53 Guinea 55 53 Liberia 55 52 African Region 54 i Definition: average number of years that a newborn is expected to live if current mortality rates continue to apply Figure 5 : Healthy life expectancyii at birth in years, in Sierra Leone and neighboring countries, by sex, 2007 Male Female 34 Sierra Leone 37 46 Guinea 48 47 Liberia 49 45 African Region 46 Mortality Figure 6 : Adult mortality rateiii per 1,000 population in Sierra Leone and neighboring countries, 2008 and 1990 2008 1990 393 Sierra Leone 469 340 Liberia 717 336 Guinea 410 392 African Region 371 ii Definition: average number of years that a person can expect to live in “full health” by taking into account years lived in less than full health due to disease and/or injury iii Definition: probability that a 15-year-old person will die before reaching his/her 60th birthday. Mortality data. Geneva, World Health Organization, 2010 (www.who.int/healthinfo/statistics/mortality/en/) -

Addis Ababa University
ADDIS ABABA UNIVERSITY SCHOOL OF GRADUATE STUDIES THE ROLE OF PRIVATE MILITARY AND SECURITY COMPANIES IN AFRICAN CONFLICTS: WITH PARTICULAR REFERENCE TO CONFLICTS IN SIERRA LEONE AND ANGOLA BY EYASU GIZAW WOLDE ADDIS ABABA APRIL 2011 THE ROLE OF PRIVATE MILITARY AND SECURITY COMPANIES IN AFRICAN CONFLICTS: WITH PARTICULAR REFERENCE TO CONFLICTS IN SIERRA LEONE AND ANGOLA BY EYASU GIZAW WOLDE A THESIS SUBMITTED TO THE SCHOOL OF GRADUATE STUDIES OF ADDIS ABABA UNIVERSITY IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTER OF ARTS IN INTERNATIONAL RELATIONS ADVISOR DR. TAREKEGN ADEBO ADDIS ABABA UNIVERSITY SCHOOL OF GRADUATE STUDIES COLLEGE OF SOCIAL SCIENCES DEPARTMENT OF POLITICAL SCIENCE AND INTERNATIONAL RALATIONS ADDIS ABABA APRIL 2011 ADDIS ABABA UNIVERSITY SCHOOL OF GRADUATE STUDIES THE ROLE OF PRIVATE MILITARY AND SECURITY COMPANIES IN AFRICAN CONFLICTS: WITH PARTICULAR REFERENCE TO CONFLICTS IN SIERRA LEONE AND ANGOLA BY EYASU GIZAW WOLDE COLLEGE OF SOCIAL SCIENCES DEPARTMENT OF POLITICAL SCIENCE AND INTERNATIONAL RALATIONS ADDIS ABABA APRIL 2011 ADDIS ABABA UNIVERSITY SCHOOL OF GRADUATE STUDIES The Role of Private Military and Security Companies in African Conflicts: With Particular Reference to the Conflicts in Sierra Leone and Angola BY EYASU GIZAW WOLDE APPROVED BY BOARD OF EXAMINERS SIGNATURE DATE _______________ _________ ______ ADVISOR ________________ _________ _______ EXAMINER ADDIS ABABA APRIL 2011 Table of Contents Page Table of contents…………………………….…………………………..……………….……….i Acronyms……………………………………………………………………………....…………iv -
![National Electoral Commission [NEC] Sierra Leone](https://docslib.b-cdn.net/cover/4156/national-electoral-commission-nec-sierra-leone-7364156.webp)
National Electoral Commission [NEC] Sierra Leone
National Electoral Commission [NEC] Sierra Leone ANNUAL REPORT SEPTEMBER 2006 – SEPTEMBER 2007 NEC HQ under Construction NOVEMBER, 2007 National Electoral Commission [NEC] Sierra Leone ANNUAL REPORT SEPTEMBER 2006 – SEPTEMBER 2007 NOVEMBER, 2007 MISSION STATEMENT The National Electoral Commission [NEC] is a public institution, whose mission is to organize, conduct and supervise all public elections and referenda, register all eligible voters, demarcate constituency boundaries and make regulations for the efficient performance of its functions. The National Electoral Commission shall impartially serve all stakeholders in the electoral process, and shall undertake voter education programmes for the citizens of Sierra Leone as a means of promoting and sustaining democracy good governance and an enlightened citizenry. VISION The vision of the National Electoral Commission [NEC] is that of an independent, credible and well-resourced institution which promotes democracy and good governance by continually administering elections in such a manner that the results are acceptable to all FOREWORD This report covers the period 1st September 2006 – 31st September 2007. During the period under review, the National Electoral Commission (NEC) was mainly occupied with the laying of a solid foundation for the conduct of the 2007 Presidential and Parliamentary elections, which is part of the Commission’s mandate. The production of this annual report is also in fulfilment of our constitutional responsibility. The National Electoral Commission successfully conducted the 2007 Presidential and Parliamentary elections. NEC is grateful for the sustained financial and moral support received from the Government of Sierra Leone, the International Development Partners, the United Nations System, the general public and the people of Sierra Leone during the last twelve months. -
West Africa's Evolving
Vol 17 Cover D1 5/14/07 9:17 AM Page 2 As the security architecture of the Economic Community of West African States (ECOWAS) evolves, the organisation will continue to be confronted with conflict management challenges that span the areas of: • Governance (elections and democratic transitions); • Development (gender inequality and HIV/AIDS); and SECURITY ARCHITECTURE: EVOLVING WEST AFRICA’S • Security sector reform and post-conflict peacebuilding. Meeting these challenges effectively could largely determine whether West Africa is at peace or at war in the new millennium. This seminar report captures the essence of the current debate surrounding these pressing concerns. LOOKING BACK TO THE FUTURE TO BACK LOOKING WEST AFRICA’S EVOLVING SECURITY ARCHITECTURE LOOKING BACK TO THE FUTURE CENTRE FOR CONFLICT RESOLUTION CAPE TOWN, SOUTH AFRICA UNIVERSITY OF CAPE TOWN C/O RHODES GIFT POST OFFICE 7707 CAPE TOWN, SOUTH AFRICA CENTRE FOR TEL: +27 21 689 1005 FAX: +27 21 689 1003 E-MAIL: [email protected] CONFLICT http://ccrweb.ccr.uct.ac.za RESOLUTION CAPE TOWN, SOUTH AFRICA POLICY SEMINAR REPORT 30 AND 31 OCTOBER 2006, LA PALM HOTEL, ACCRA, GHANA 17 Vol 17-WA Report Final 5/14/07 10:29 AM Page 1 WEST AFRICA’S EVOLVING SECURITY ARCHITECTURE LOOKING BACK TO THE FUTURE POLICY SEMINAR REPORT LA PALM HOTEL, ACCRA, GHANA 30 AND 31 OCTOBER 2006 RAPPORTEURS ANGELA NDINGA-MUVUMBA AND ABDUL LAMIN Vol 17-WA Report Final 5/14/07 10:29 AM Page 2 Vol 17-WA Report Final 5/14/07 10:29 AM Page 3 Table of Contents Acknowledgements 5 About the Organisers and Rapporteurs 5 Executive Summary 6 1. -

Measuring Gender Equality & Women's Empowerment in Africa
Measuring Gender Equality & Women’s Empowerment in Africa Measuring Gender Equality & Women’s Empowerment in Africa Measuring Gender Equality & Women’s Empowerment in Africa To order copies of Measuring Gender Equality and Women’s Empowerment in Africa, please contact: Publications Section Economic Commission for Africa P.O. Box 3001 Addis Ababa, Ethiopia Tel: +251 11 544-9900 Fax: +251 11 551-4416 E-mail: [email protected] Web: www.uneca.org © 2019 Economic Commission for Africa Addis Ababa, Ethiopia All rights reserved First printing July 2019 Material in this publication may be freely quoted or reprinted. Acknowledgement is requested, together with a copy of the publication. The designations employed in this report and the material presented in it do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations Economic Commission for Africa or the African Union concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Designed and printed in Addis Ababa, Ethiopia by the ECA Printing and Publishing Unit. ISO 14001:2004 certified. Printed on chlorine free paper Cover photos: Shutterstock.com Contents Abbreviations and acronyms ............................................................................................... xii Acknowledgements ............................................................................................................. xiii 1.Introduction and background -

Research Proposal
Investigating the Inclusion of Ethno-Depoliticization within Peace-Building Policies in Post- Conflict Sierra Leone Matilda Josephine Cole Thesis Submitted to the Faculty of Graduate and postdoctoral Studies In partial fulfilment of the requirements For the MA in Globalization and International Development School of International Development and Global Studies Faculty of Social Sciences University of Ottawa October, 2012 © Matilda Josephine Cole, Ottawa, Canada, 2012 Table of Contents ABBREVIATIONS ..................................................................................................................................... iv LIST OF FIGURES ..................................................................................................................................... vi LIST OF TABLES...................................................................................................................................... vii ABSTRACT ............................................................................................................................................ viii ACKNOWLEDGEMENTS .......................................................................................................................... ix DEDICATION ............................................................................................................................................ x Chapter 1 Introduction ........................................................................................................................... 1 Background History -

Sierra Leone
SIERRA LEONE Economic Freedom Score 50 25 75 Least Most free 0 100 free World Rank: 148 Regional Rank: 34 50.5 ierra Leone’s economic freedom score is 50.5, making its Seconomy the 148th freest in the 2014 Index. Its score is 2.2 Freedom Trend points higher than last year, with substantial increases in half 52 of the 10 economic freedoms including the control of govern- ment spending, property rights, business freedom, and labor 51 freedom. Sierra Leone is ranked 34th out of 46 countries in the Sub-Saharan Africa region, and its overall score is below 50 the world average. 49 Over the 20-year history of the Index, Sierra Leone’s economic freedom score has improved by 0.7 point. Improvements in 48 half of the 10 economic freedoms include double digit growth in trade freedom, fiscal freedom, and freedom from corrup- 47 tion. Grading of Sierra Leone was suspended from 2001 to 2002 due to internal conflicts. 46 2010 2011 2012 2013 2014 Achieving its highest economic freedom score ever in the 2014 Index, Sierra Leone has advanced from economically “repressed” for the second time. Reforms have been target- Country Comparisons ed at improving regulatory efficiency and strengthening the enforcement of contracts. However, weak protection of prop- Country 50.5 erty rights and pervasive corruption still jeopardize the emer- World gence of a sustainable private sector. Average 60.3 BACKGROUND: Opposition candidate Ernest Bai Koroma Regional was elected president in 2007 in Sierra Leone’s first peace- Average 54.6 ful transition of power since independence in 1961.